Article Text

Abstract
Background Percutaneous mitral valve repair (MVR) using the MitraClip system has become a valid alternative for patients with severe mitral regurgitation (MR) and high operative risk.
Objective To identify clinical and periprocedural factors that may have an impact on clinical outcome.
Design Multi-centre longitudinal cohort study.
Setting Tertiary referral centres.
Patients Here we report on the first 100 consecutive patients treated with percutaneous MVR in Switzerland between March 2009 and April 2011. All of them had moderate–severe (3+) or severe (4+) MR, and 62% had functional MR. 82% of the patients were in New York Heart Association (NYHA) class III/IV, mean left ventricular ejection fraction was 48% and the median European System for Cardiac Operative Risk Evaluation was 16.9%.
Interventions MitraClip implantation performed under echocardiographic and fluoroscopic guidance in general anaesthesia.
Main outcome measures Clinical, echocardiographic and procedural data were prospectively collected.
Results Acute procedural success (APS, defined as successful clip implantation with residual MR grade ≤2+) was achieved in 85% of patients. Overall survival at 6 and 12 months was 89.9% (95% CI 81.8 to 94.6) and 84.6% (95% CI 74.7 to 91.0), respectively. Univariate Cox regression analysis identified APS (p=0.0069) and discharge MR grade (p=0.03) as significant predictors of survival.
Conclusions In our consecutive cohort of patients, APS was achieved in 85%. APS and residual discharge MR grade are important predictors of mid-term survival after percutaneous MVR.
- Valvular Disease
Statistics from Altmetric.com
Introduction
Mitral regurgitation (MR) is the most common cardiac valvular heart disease with a prevalence in a general population of approximately 10% among individuals above 75 year of age1 ,2 contributing substantially to morbidity and mortality,3–7 even independently of left ventricular (LV) function.8 Surgical mitral valve repair (MVR) is considered the treatment of choice based on its superior long-term results compared with mitral valve replacement or medical therapy.9 ,10 However, many patients with symptomatic severe MR and significant comorbidities or advanced age are denied surgery because of a high surgical risk.11 Percutaneous MVR using the MitraClip-system (Abbott Vascular, Abbott Park, Illinois, USA) has recently emerged as a promising novel transcatheter technique for the treatment of severe MR. This technique is based on the surgical edge-to-edge repair described by Alfieri12 where MR is reduced by approximating the edges of both mitral leaflets, thereby restoring valvular coaptation and creating a double-orifice mitral valve. Its safety, feasibility, high procedural success rates and mid-term durability have been established in several clinical registries in the USA13 and Europe.14–18 A recent randomised trial yielded superior safety of the MitraClip procedure compared with surgical MVR; however, after exclusion of transfusion, safety was similar in both groups, whereas surgery provided better efficacy regarding sustained MR reduction.19 Of note, these series as well as other recently published US reports13 ,20 included predominantly patients with degenerative MR, preserved LV function and low surgical risk, and therefore potentially excluded a large group of patients which may benefit from the procedure. However, a few small studies have shown feasibility and high procedural success rates together with improved short-term echocardiographic and clinical outcomes in higher risk populations with predominantly functional MR, reduced LV function and high surgical risk.17 ,21
In spite of these encouraging studies, clinical outcome following MitraClip treatment is not well documented. It has been proposed that immediate haemodynamic changes such as an increase in cardiac index and a decrease in pulmonary artery and wedge pressures may predict short-term outcomes, and are associated with a low event rate at follow-up.22 ,23 Nevertheless, data on other predictors of mid-term clinical success or survival after percutaneous MVR are currently lacking.
The aim of the present study was to identify clinical and periprocedural factors predicting mid-term clinical outcomes in the first 100 patients undergoing percutaneous MVR using the MitraClip system. This registry represents the entire population treated by percutaneous MVR in Switzerland prior to April 2011.
Methods
Study sample
Between February 2009 and April 2011, we consecutively included the first 100 patients undergoing percutaneous MVR using the MitraClip system in a prospective national registry. Four cardiac centres in Switzerland had introduced the procedure, that is, Cardiocentro Ticino, the University Hospitals of Zurich and Basel and Cantonal Hospital of Lucerne. All patients had moderate-to-severe (3+) or severe (4+) MR of functional or degenerative origin as graded according to current recommendations of the American Society of Echocardiography.24 Patients were considered for the procedure if they met class I or IIa indications for mitral valve surgery as recommended by the European Society of Cardiology European Association for Cardio-Thoracic Surgery guidelines on the management of valvular heart disease 201210 and had a high surgical risk (defined by a logistic European System for Cardiac Operative Risk Evaluation (EuroSCORE) mortality >15% or the presence of specific surgical risk factors not covered by the EuroSCORE (ie, frailty, immunosuppressive therapy, porcelain aorta or extensive mediastinal radiation)). Furthermore, patients with functional MR and a class IIb indication10 were eligible for percutaneous MVR. Absolute exclusion criteria were rheumatic heart disease and florid endocarditis, whereas the originally applied ‘Everest criteria’20 (ie, a mitral valve orifice area <2.0 cm2, extensive prolapse of flail leaflets (prolapse width >25 mm, flail gap >20 mm) or any interventional or surgical procedure within 30 days following the index procedure) were only considered as reference parameter but not as absolute exclusion criteria. Indications for treatment of MR and individual surgical risk were assessed by an interdisciplinary HEART team consisting of interventional cardiologists, echocardiographers, cardiac anaesthetists and cardiac surgeons. The local institutional review board approved the study protocol. All patients gave written informed consent to be entered into the database.
Percutaneous MVR procedure
Percutaneous MitraClip implantation was performed under general anaesthesia with echocardiographic (transesophageal) and fluoroscopic guidance, as extensively described previously.13–16 ,19 ,20 ,22 In brief, after trans-septal puncture a 24-French catheter-based delivery system is placed via the femoral vein in the left atrium. Thereafter, the MitraClip is fed through the catheter and directed towards the mitral valve where it is aligned with the maximum jet originating from the regurgitant lesion. Grasping and approximating the edges of the mitral leaflets in the area of the maximal regurgitation jet results in a double mitral orifice and a significant reduction of the MR. Acute procedural success (APS) was defined as successful implantation of one or more clips with a reduction of the MR to ≤2+.
Follow-up and outcome variables
Clinical and echocardiographic follow-up was scheduled at 6 months after the MVR procedure. Echocardiographic parameters were assessed in each individual centre. The severity of MR was graded according to recommendations of the American Society of Echocardiography.24 LV volumes and LV ejection fraction (LVEF) were assessed using the biplane Simpson's method.25 LV end-diastolic and end-systolic diameters (LVEDD and LVESD) as well as left atrial diameter were measured on M-mode in the parasternal long axis view. Systolic pulmonary pressures were estimated from measuring the pressure gradient between right ventricle and right atrium in systole.
Clinical endpoints included all-cause mortality, NYHA functional class26 and mitral valve surgery due to failure of percutaneous MVR. For regression analyses to yield potential predictors of outcome, clinical and echocardiographic outcome variables were grouped into a combined clinical efficacy endpoint consisting of survival, freedom from mitral valve surgery, absence of postimplant congestive heart failure and persistent MR ≤2+ at 6 months follow-up. Bleeding was assessed according to the Valve Academic Research Consortium (VARC) criteria.27
Statistical analysis
Descriptive statistics of the baseline characteristics are expressed as number of observations (n), median and IQR or mean and SD respectively for continuous variables whereas categorical data are shown as percentages. To associate a nominal variable to another nominal variable, we provided a frequency table as well as a p value of either a χ2 or Fisher's exact test, whichever was appropriate. To compare a continuous variable between two groups, we used Wilcoxon test or alternatively Student t test presuming that the normality assumption has been met. As for comparison of changes from baseline to follow-up, we provided results of a t test applied to paired data. To associate a continuous response variable to covariate while adjusting for the baseline value of the response, we performed analysis of covariance.
Survival time is associated with a nominal variable using log-rank test and to a continuous variable using Cox regression. In addition, a Kaplan–Meier estimate is provided for all patients, including a CI for the 75% quantile of time to survival, given the fact that the median time of survival has not been reached. Follow-up was assessed using inverted Kaplan–Meier estimates.28 All CIs are computed at a confidence level of 95%. Given the large number of statistical tests (42 correlation tests to survival and to the combined clinical efficacy endpoint, respectively) performed in this analysis the probability of a type I error may be importantly inflated. For this reason we decided to provide, whenever possible and reasonable, CIs rather than statistical testing in this analysis. For all tests, we considered a p value of <0.05 as statistically significant. All analyses are done using ‘R’ (R Development Core Team, 2010).
Results
Patient sample and baseline characteristics
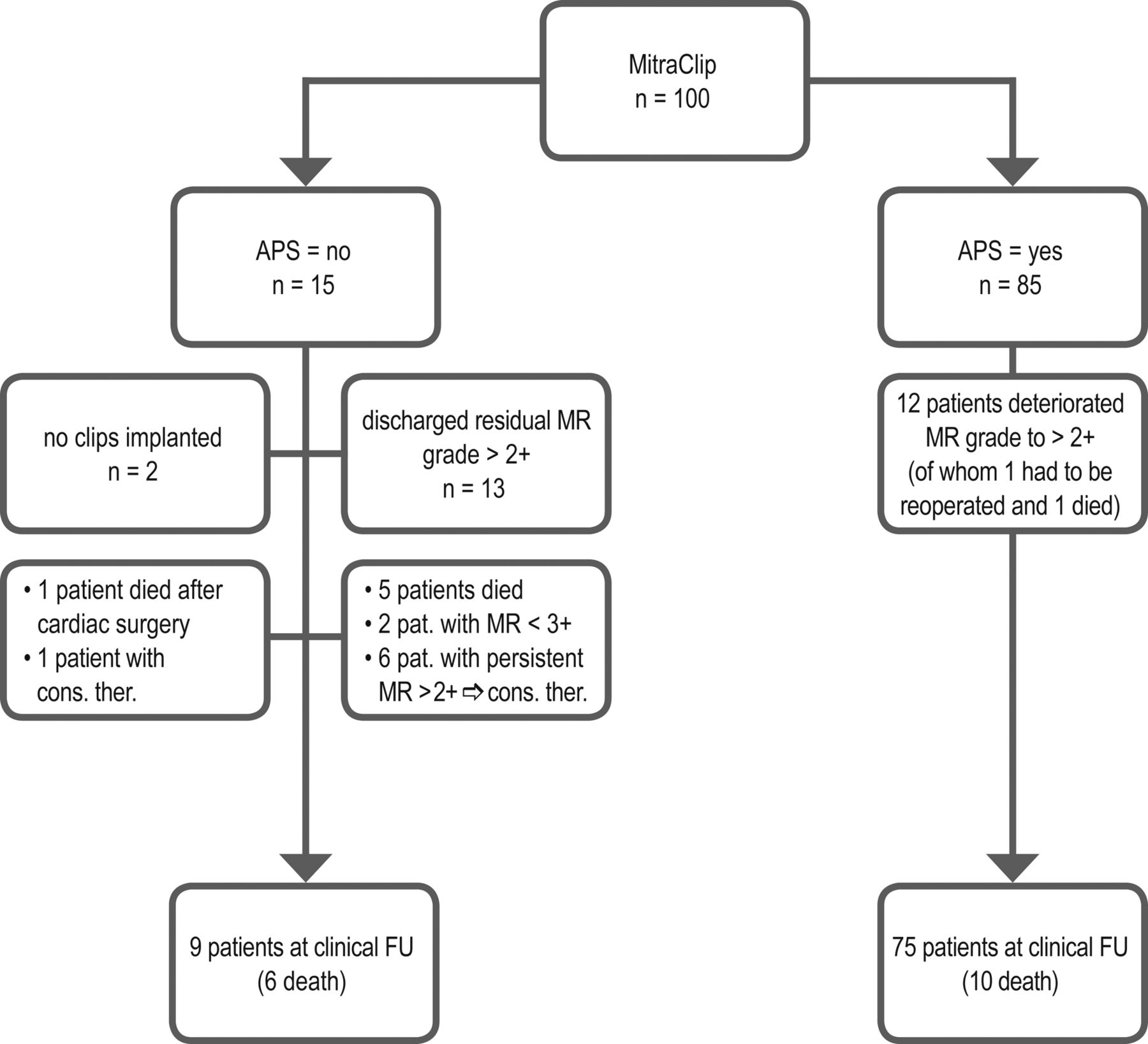
Between February 2009 and April 2011, 100 consecutive patients treated in four centres were prospectively included in the MitraSwiss registry (patient flow is shown in figure 1). This represents the entire population of patients treated by MitraClip edge-to-edge MVR in Switzerland since its clinical introduction. The median patient age was 77 years (IQR 18.5) and 23% were female patients. All patients had MR grade 3+ or 4+. MR aetiology was functional in 62% of patients and degenerative in 38%. Mean LVEF was 0.48 (SD 0.19) and the majority of the patients were in functional class NYHA III or IV (82%) or had a history of decompensated heart failure in the near past (77%). The median surgical risk, as assessed by the logistic EuroSCORE, was 17% (IQR 19). The remainder of the patient baseline characteristics is given in table 1.
Baseline characteristics of the first 100 patients

Flowchart showing the fate of the 100 patients, treated with MitraClip. APS, acute procedural success; MR, mitral regurgitation.
Results of the implantation procedure
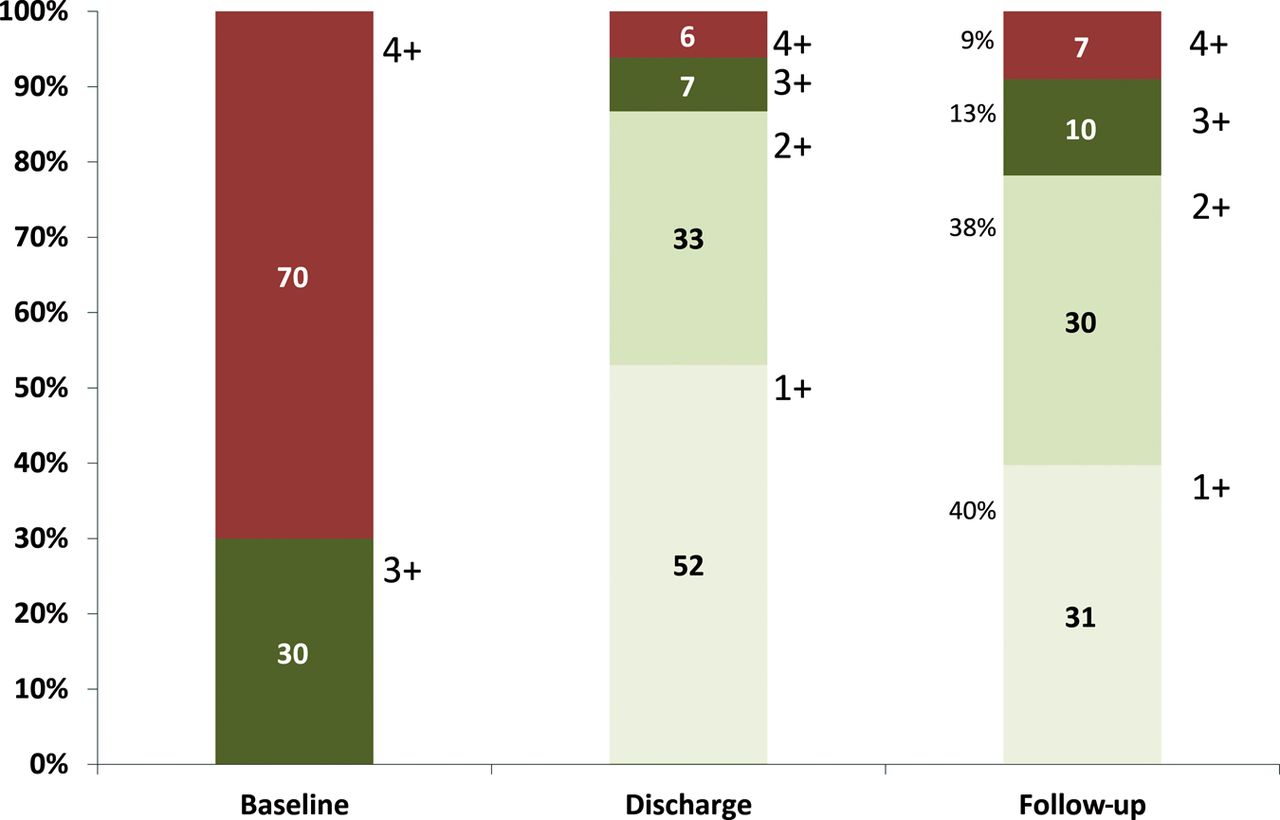
The acute procedural results are summarised in table 2. In 54% a single clip was sufficient, whereas in 40% two clips and in 4% of the patients three clips were implanted. APS was achieved in 85% of the cases (figure 2). In 52% of the patients MR grade was reduced to 1+ and in 33% to 2+. We did not identify any clinical or morphological factors predicting APS and there was no statistical difference in the APS rate when comparing functional (APS=79%) or degenerative (APS=92%) MR. The duration of the intervention decreased along with growing experience of the operators. For the first 10 cases of each centre, device time, defined as the time from guide catheter insertion to withdrawal of the delivery system into the guide catheter, was 124 min (IQR 76; 95% CI 105 to 141). This parameter significantly decreased to 72.5 min (IQR 45.25; 95% CI 68 to 102) for the last 10 patients (p=0.004) indicating a relevant learning curve for the technique (table 3). Similarly, an increase in APS rate from 85% to 93% could be observed over the same time period, although this change fell short of statistical significance.
Periprocedural results and safety
Learning curve of the four implanting centres

Change of mitral regurgitation grade from baseline to discharge and to Follow-up.
Inhospital outcomes
Overall, serious life-threatening or fatal complications related to the MitraClip procedure were rare. In all, 98% were extubated immediately after or within 2 h after the procedure. Inhospital death was 4% (table 2) and all cases occurred within the very early individual experience of the technique: there was one periprocedural death due to rupture of a papillary muscle in an 84-year-old patient with severe MR and cardiogenic shock 10 days after acute myocardial infarction. This patient consented to the MitraClip procedure as a salvage therapy in the face of rapid medical deterioration without further therapeutic options. A second patient died in hospital 2 months after unsuccessful MitraClip procedure on the waiting list for heart transplantation. In a third patient, an increase of the mean transvalvular aortic gradient from 27 to 60 mm Hg occurred after successful placement of one clip, with deterioration of LV function and subsequent severe heart failure and death 2 days after the percutaneous MVR. In two patients (2%), the procedure was complicated by a chordal rupture with acute worsening of the MR. One of them immediately underwent surgical mitral valve replacement but died 5 days postoperatively, whereas the second patient was treated with intra-aortic balloon counterpulsation and underwent successful mitral valve surgery 7 days later.
Follow-up outcomes
Clinical follow-up was complete within the surviving population while echocardiographic follow-up was available in 78% of patients. Missing echocardiographic data (n=22) included loss to echocardiographic follow-up (n=10) and death (n=12 at 6 months).
The percentage of patients with MR grade ≤ 2+ at follow-up was 78%, whereas 13% presented an MR grade 3+ and 9% an MR grade 4+ (figure 2). Overall, 20% of the patients remained in NYHA class III, and 80% of the patients were in class I or II (figure 3). LV end-diastolic volume (LVEDV), indexed LVEDV, LV end-systolic volume (LVESV), LV diameters (LVEDD and LVESD) and systolic pulmonary artery pressure decreased significantly between baseline and follow-up (table 4). In an analysis of covariance, predictors for improvement of pulmonary artery pressure at follow-up with respect to baseline were APS (p=0.0017) and low MR grade at discharge (p global=0.0078; p=0.0024 for MR >2+). No significant change in LVEF and left atrial diameter were seen during the follow-up.
Echocardiographic and biohumoral changes from baseline to follow-up.
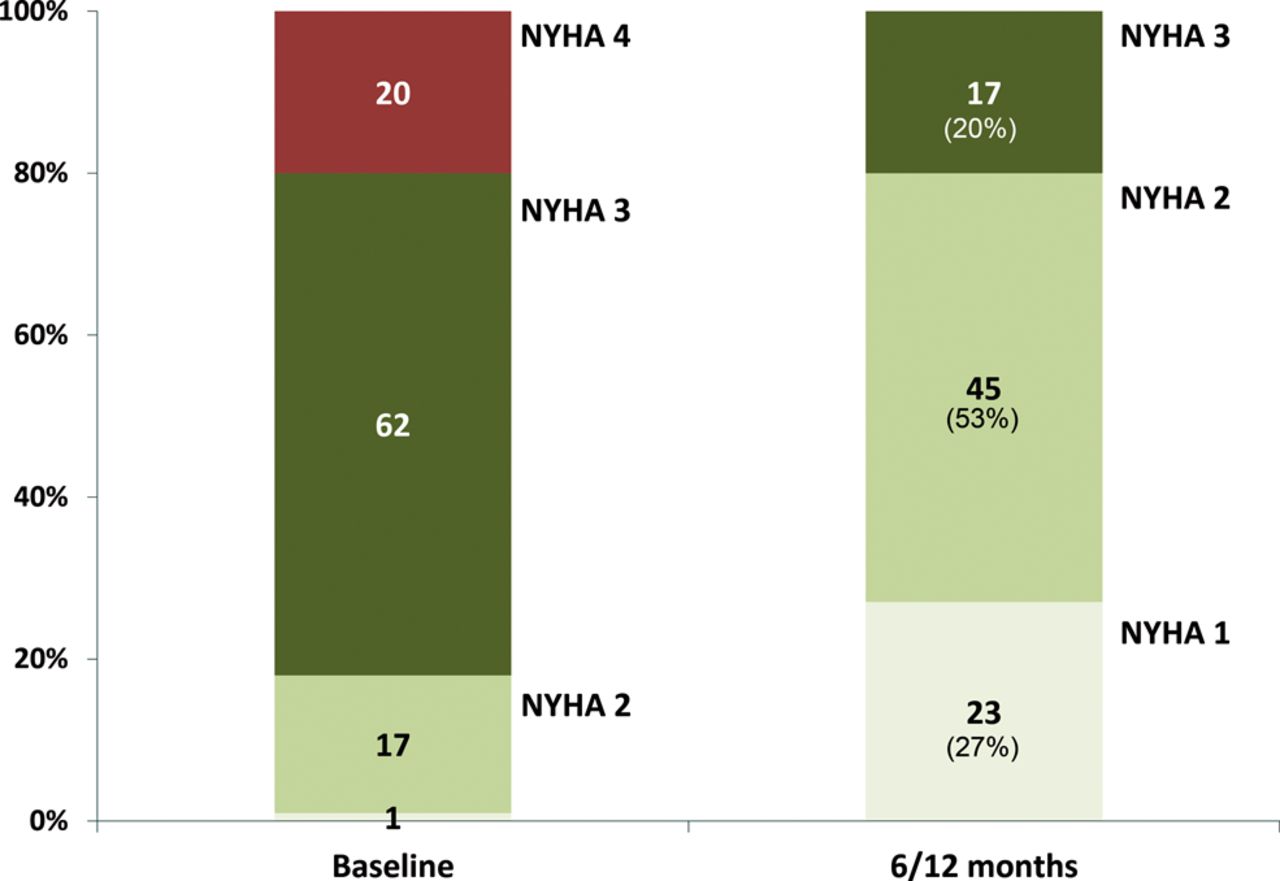
Change of NYHA class from baseline to FU.
LVEF, LV volumes and LV diameters have then been analysed splitting the entire patient sample according to the mechanism of MR (supplementary table S1). Not unexpected, the significant improvement in LV remodelling of the entire patient sample seems to be mainly driven by the subgroup with functional MR, where most of the decrease in LVEDV, LVESV, LVEDD and LVESD appeared. On the other hand, the significant decrease in pulmonary artery pressure in the entire patient sample was mainly driven by changes in the subgroup with degenerative MR where a significant decrease of nearly 10 mm Hg was observed (p=0.02).
Among adverse events which occurred during follow-up five patients presented with single leaflet clip detachment, of which four had degenerative MR. In three cases this was associated with early clinical deterioration, and all three patients underwent redo clipping (9–12 months after the initial intervention). In two cases detachment was found at 3 and 6 months follow-up, respectively, without any signs of clinical impairment. Both these cases have been managed conservatively so far.
In one patient mitral valve replacement had to be performed because of severe mitral stenosis detected 3 months after the implantation of two clips. Reoperation rate at mid-term was 5%.
Predictors of long-term efficacy
The combined clinical efficacy endpoint was met in 58 (64%) of the patients at 6 months follow-up. Predictors for long-term efficacy were body mass index (inversely predictive) and MR grade at discharge (table 5). The proportion of the efficacy endpoint was significantly higher (p value Fisher‘s exact test: 0.0000002) among patients with an MR grade of 1+ at discharge (89%) compared with the patients with MR grade of 2+ (48%) or MR grade of >2+ (15%). The mechanism of MR (p=0.63) and LV volumes at baseline (p=0.78 for LVEDV and p=0.56 for LVESV) did not directly influence on efficacy.
Predictors for clinical efficacy
The 75% quantile of overall survival was 23.4 months (95% CI 12.10; Inf) with a median follow-up time of 15.77 months (95% CI 14.20 to 18.07). A total of 20 deaths occurred. A low MR grade at discharge (p=0.03) and APS (p=0.0069) were identified as predictors of survival, highlighting the importance of the initial procedural result (figure 4; supplementary table S2). Interestingly, patients with MR grade 1+ at discharge had a better prognosis than patients with an MR grade of 2+ or more at discharge. Furthermore, congestive heart failure before clip-implantation (p=0.04) and prior coronary artery bypass grafting (CABG) (p=0.008) were identified as predictors of mortality. Of note that 15 of 16 CABG patients had Functional mitral regurgitation (FMR), and only in one patient, degenerative origin of the MR was predominant. The combination of functional MR and CABG is effectively a potent predictor of mortality (p=0.0042), whereas functional MR without prior CABG (47 out of 62 patients) is not (figure 4; supplementary table S2). Likewise, the presence of coronary artery disease alone and baseline LV parameters (i.e. LV volumes; LVEF) did not influence on patient's survival.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier curves of survival. (A) Survival depending on mitral regurgitation (MR) grade after MitraClip implantation (MR grade 1+: black line; MR grade 2+: red line; MR grade >2+: green line). (B) Survival of patients with (red line) or without acute procedural success (black line). (C) Survival of patients with (red line) or without (black line) episodes of congestive heart failure in their clinical history before MitraClip implantation. (D) Survival of patients with functional MR (FMR) without associated coronary artery bypass grafting (CABG) in medical history. (E) Survival of patients with FMR and CABG in medical history.
Discussion
The present report represents the Swiss experience with MitraClip edge-to-edge percutaneous MVR. It consists of the first 100 patients treated by this technique and entered prospectively into the MitraSwiss registry, a large nationwide collaborative network database of centres in which this procedure is performed. The results from this database indicate that the MitraClip procedure is feasible and safe in a heterogeneous population consisting of patients with predominantly functional MR and reduced ejection fraction. APS (a reduction of MR to 2+ or less during the procedure), the severity of residual MR at discharge and inhospital congestive heart failure emerged as predictors of mid-term outcome. This emphasises the importance of obtaining an optimal result and a predischarge echocardiography to predict the prognosis of the patient after MVR.
Percutaneous MVR, using the MitraClip system, is expanding all over the world and particularly in Europe. Worldwide, the system has already been used in more than 6000 patients. Even in high-risk patients the technique has been shown to be safe and feasible. However, evidence is limited to a few open-label registries13–16 ,18 ,20 and one randomised study.19 Two series focused on patients with severe LV dysfunction17 or patients refractory to cardiac resynchronisation therapy and reported similar results.21 In the European cohorts14–18 the majority of the patients had functional MR, whereas in the endovascular valve edge-to-edge repair study (EVEREST) II19 trial the majority had degenerative mitral valve disease.
In contrast to the EVEREST13 ,19 ,20 series, 62% of the patients in the present study had functional MR and many of them had severe LV dysfunction and were therefore not considered suitable for surgery. The rate of successful MitraClip implantation and the APS rate were over 80% and the acute treatment effects were similar to the EVEREST13 ,19 ,20 series. Long-term clinical results are characterised by an elevated rate of all-cause mortality (16% at 12 months), which is not surprising for this high-risk patient population. In the surviving population, the treatment effects are shown to be durable over time. Nevertheless, there are still several questions regarding patient selection and predictors of treatment success.
As previously reported by Franzen et al,17 our data indicate that treatment of patients with severely depressed LVEF using the MitraClip is feasible and safe. A potential explanation for this is that the acute reduction in volume overload by reducing the regurgitant volume could compensate for the immediate afterload increase, thus challenging the ‘pop-off’ valve concept.22 In fact no acute decompensation was seen in our heart failure population even in those with a severely enlarged LV and impaired LV function. Furthermore, our data do not indicate that APS or clinical efficacy depend on whether the aetiology of the MR was functional or degenerative.
The challenge for the future will be to perform further analyses in order to define well-validated clinical or echocardiographic predictors of procedural success and to test the intervention in a large randomised outcome trial. The so-called echocardiographic `EVEREST criteria` may be of help to predict feasibility and success of the intervention as well as to reduce the rate of treatment failure. However, in European case series many patients have been treated successfully despite not meeting these criteria.
Failure of surgical MVR is generally defined as recurrence of moderate MR or worse. Therefore, a surgical intervention may be considered successful only if the acute echocardiographic result does not exceed residual trace or mild MR. Acute success in percutaneous MVR has not been clearly defined by an expert committee. In the American series, Feldman and colleagues20 proposed the term APS for those MitraClip interventions with technically successful delivery of one or more clips resulting in an MR grade of 2+ or better, which correlates to less stringent criteria when compared with surgical MVR. The acceptance of partial MR reduction as treatment result after percutaneous MVR may have been partially driven by the idea that complete reduction of MR may be harmful, especially in patients with functional MR and severe LV depression. Our data emphasise the importance of an optimal echocardiographic result directly after MitraClip implantation independent of LV function. Patients with residual MR of grade 1+ or less had a better prognosis than those with grade 2+ or more in terms of all-cause mortality and the combined clinical efficacy endpoint at 6 months. Our data therefore clearly indicate that every effort should be undertaken to avoid an insufficient primary result of the MitraClip procedure. APS remains to be an important objective, but echocardiographic MR grade of 1+ may be the optimal `treatment goal` for patients after percutaneous MVR using the MitraClip system.
In conclusion, our data confirm feasibility, safety and mid-term efficacy of percutaneous MVR using the MitraClip system, even in a high-risk patient population with predominant functional MR. Our data also clearly suggest that a patient's prognosis may depend directly on the initial procedural results (MR reduction to <2+). Operators should therefore aim for an optimal acute result, even in patients with a severely depressed LV function.
The limitations of the study are its observational nature and open-label design and the absence of a control group. Furthermore, multiple statistical testing may enhance the probability of a type I error. Obviously the study has not been powered to distinguish differences such as survival between subgroups. The results of our study should therefore be considered as exploratory and ‘hypothesis-generating’. Larger, ideally core-lab based studies, are needed to confirm them.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 4
- Data supplement 2 - Online table 6
Footnotes
-
Contributors All coauthors contributed in a substantial way to the article, including conception and design of the registry, acquisition of data or analysis and interpretation of data. All of them revised the article critically and finally approved the article.
-
Funding Fondazione Cardiocentro Ticino, Lugano, Switzerland, Cantonal Hospital Lucerne, Switzerland, Cardiovascular Research Foundation, Zurich, Switzerland, University Hospital Zurich, Switzerland, and University Hospital Basel, Switzerland.
-
Competing interests Oliver Gaemperli and Roberto Corti received lecture fees from Abbott Vascular, Oliver Gaemperli, Roberto Corti and Thomas F. Lüscher received an institutional grant from Abbott Vascular. All the remaining authors have nothing to disclose directly related to the article.
-
Patient consent Obtained.
-
Dat sharing No additional data available.
-
Ethics approval Regional ethical committees.
-
Provenance and peer review Not commissioned; externally peer reviewed.