Article Text

Abstract
Background Left ventricular longitudinal diastolic functional reserve (DFR), as assessed by the change in early diastolic mitral annular velocity (E′) during exercise, is abnormal in patients with type 2 diabetes mellitus (DM). However, the impact of left ventricular longitudinal DFR on clinical outcome has not been explored. This study evaluated the incremental prognostic value of left ventricular DFR in patients with type 2 DM without overt heart disease.
Methods Of 1485 patients who were referred for exercise stress echocardiography, 197 consecutive patients (mean age, 58 years; 84 men) with type 2 DM without overt heart disease were identified. Left ventricular longitudinal DFR was defined as the change in E′ from resting to exercise (ΔE′). The endpoint was a composite of death and hospitalisation for heart failure (HF).
Results During a median follow-up of 57 months (range 6–90), 18 of 197 patients (9.1%) had adverse events (12 deaths, six hospitalisations for HF). Independent predictors of adverse events in a Cox regression analysis were estimated glomerular filtration rate (HR 0.97; 95% CI 0.95 to 0.98; p<0.001), DM duration (HR 1.07; 95% CI 1.01 to 1.14; p=0.018) and ΔE′ (HR 0.58; 95% CI 0.40 to 0.85; p=0.005). In an incremental model, the addition of stress echo data significantly increased the χ2 of the clinical and resting left ventricular function model, from 40.5 to 46.6 (p=0.005).
Conclusion Assessment of left ventricular longitudinal DFR during exercise provided incremental prognostic information in patients with type 2 DM without overt heart disease.
- Diabetes mellitus
- diastole
- diastolic dysfunction
- echocardiography
- exercise
Statistics from Altmetric.com
Ischaemic heart disease is a leading cause of death in patients with diabetes mellitus (DM). The detection of ischaemic heart disease has thus been the main focus of stress testing and other non-invasive diagnostic tools. However, independent of coronary artery disease (CAD), DM can also lead to cardiac structural and functional changes, supporting the presence of diabetic heart disease.1–3 Diabetic heart disease progresses from a normal heart to subclinical left ventricular diastolic and systolic dysfunction, followed by clinically overt symptomatic heart failure (HF).4 Notably, subclinical left ventricular dysfunction is common in patients with DM. More than 60% of asymptomatic, normotensive patients with type 2 DM have subclinical diastolic dysfunction in the absence of CAD when assessed with tissue Doppler imaging.5 In addition to subclinical left ventricular dysfunction at rest, the recent application of sophisticated echocardiographic techniques, such as myocardial velocities, strain and strain rate imaging under pharmacological or exercise stress, have demonstrated that left ventricular functional reserve during stress is significantly reduced in patients with diabetes compared with controls, suggesting a higher prevalence of early myocardial disease in patients with diabetes.6–9 However, whether the assessment of left ventricular functional reserve during stress can provide additional prognostic information in patients with DM and a low risk for cardiovascular disease is unknown. In this study, we hypothesised that left ventricular longitudinal diastolic functional reserve (DFR) during exercise would have incremental prognostic value in patients with type 2 DM without overt heart disease.
Methods
Between February 2003 and October 2009, 1485 patients consisting of heterogeneous populations of those with hypertension, DM, cardiomyopathies and chronic kidney disease who were referred for exertional dyspnoea, chest pain, and for an evaluation of baseline left ventricular functional reserve underwent exercise stress echocardiography. Among them, we consecutively identified 300 patients with type 2 DM, and then excluded 103 patients with DM because of reduced left ventricular ejection fraction (LVEF <50%), angina, a history of CAD, inducible ECG changes, rest or inducible wall motion abnormalities, cardiomyopathy, significant valvular heart disease, or a significant arrhythmia. Consequently, the final study population consisted of 197 patients with type 2 DM but without overt heart disease. Referral reasons for diastolic stress echocardiography were to assess exertional dyspnoea in 67 (34%) patients and to evaluate left ventricular functional reserve during exercise in 130 (66%) patients. All patients provided informed consent. Study approval was obtained from the institutional review board of Yonsei University College of Medicine.
Two-dimensional and exercise Doppler echocardiography (diastolic stress echocardiography)
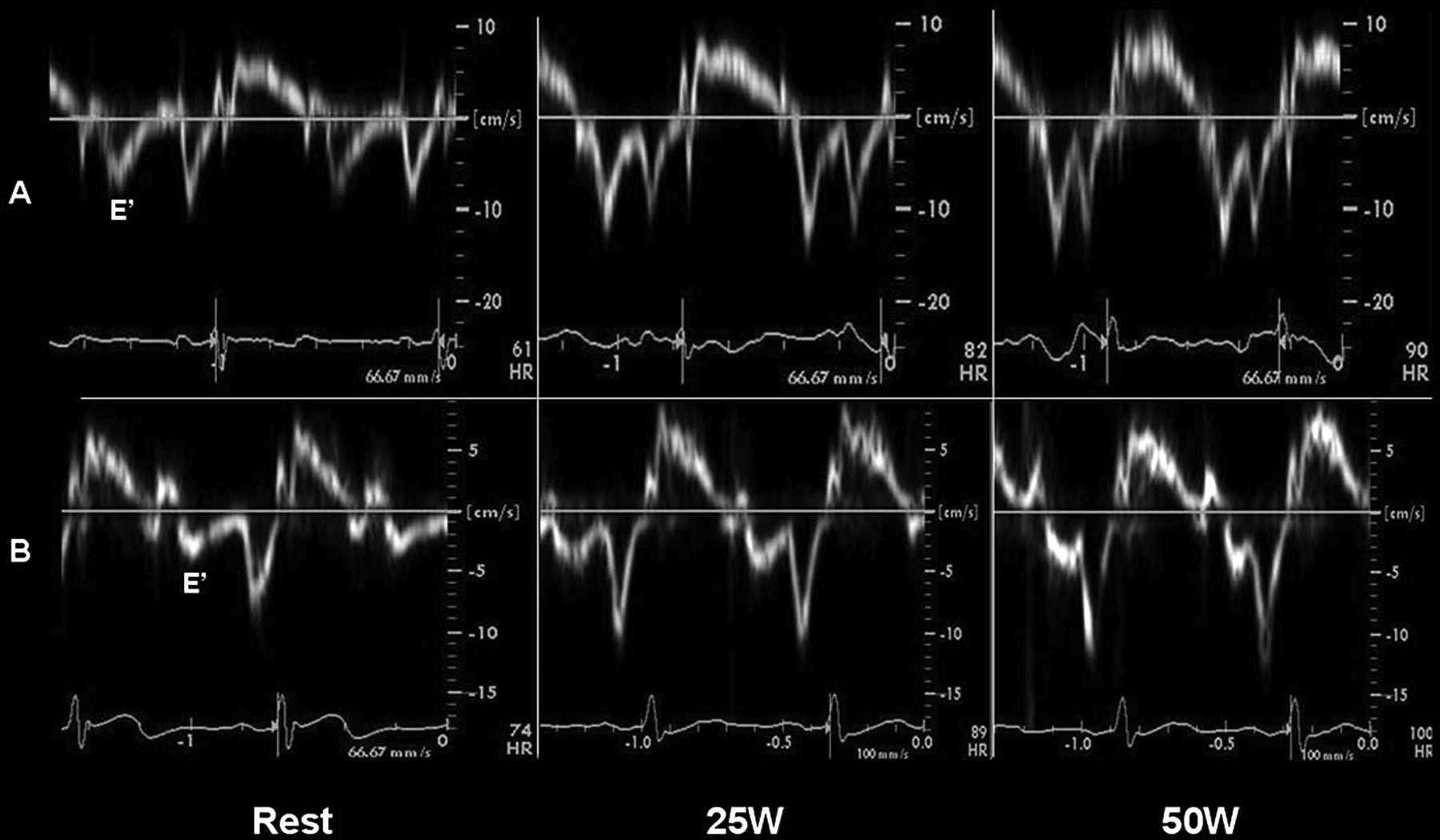
Echocardiography was performed using a GE Vingmed System 7 (GE Medical, Milwaukee, Wisconsin, USA) ultrasound system with a 2.5-MHz transducer for image acquisition. Standard two-dimensional measurements were obtained with the patient in the left lateral position. LVEF was calculated by the biplane Simpson's method using apical four and two-chamber views, as described previously.10 Left ventricular mass was calculated as 0.80×((IVST+LVED+PWT)3−(LVED)3)×1.04+0.6 g (IVST, interventricular septal thickness; LVED, left ventricular end-diastolic dimension; PWT, posterior wall thickness).11 Lentricular mass was divided by the body surface area to obtain the left ventricular mass index. Left ventricular hypertrophy was defined as a left ventricular mass index greater than 110 g/m2 in women and greater than 134 g/m2 in men.12 Left atrial volumes were calculated by the prolate ellipsoid method using the parasternal long axis view and apical four-chamber view.13 The left atrial volume index was calculated as left atrial volume/body surface area (ml/m2). Mitral inflow velocity was assessed by pulsed wave Doppler recordings from the apical four-chamber view by positioning the sample volume at the tip of the mitral leaflets. Gain and filter settings were adjusted to allow for clear tissue signals and to minimise background noise. The E and A-wave velocities, E/A ratio, and deceleration time were measured from the mitral inflow profile.14 The tissue Doppler imaging of the mitral annulus was obtained from the apical four-chamber view using a 1–2-mm sample volume placed in the septal corner of the mitral annulus, and peak systolic (S′), peak early (E′) and late (A′) diastolic velocities were also measured. Diastolic dysfunction was defined as impaired relaxation, a pseudo-normalised filling pattern, or a restrictive filling pattern.15 After obtaining resting images from the standard parasternal and apical views, a multistage supine bicycle exercise test was performed with a variable load bicycle ergometer (Medical Positioning, Inc, Kansas City, Missouri, USA). Subjects pedalled at a constant speed, beginning at a workload of 25 W, with an increment of 25 W every 3 min. Two-dimensional and Doppler echocardiographic measurements were performed at baseline, at each stage of exercise and during recovery 2, 5 and 10 min after cessation of exercise in the same sequence. All data were stored digitally and measurements were made at the end of each study. Left ventricular longitudinal DFR and systolic functional reserve during exercise were defined as ΔE′ (change in E′ from resting to exercise, figure 1) and ΔS′ (change in S′ from resting to exercise). Because a summation of mitral annular velocities was noted in achieving more than 75 W of workload with increasing heart rate, we assessed left ventricular functional reserve at 25 W and 50 W of workloads. All reported echocardiographic measurements were the average of three to five consecutive cardiac cycles.

Mitral tissue Doppler patterns of two patients with diabetes who underwent diastolic stress echocardiography. Note the increase in early diastolic annular (E′) velocities with an increase in workload. If left ventricular diastolic functional reserve (DFR) is defined as ΔE′=E′exercise−E′rest, then the DFR of patient (A) was higher than that of patient (B).
Statistical analyses
Data for continuous variables are expressed as means±SD, and categorical data are presented as frequencies and percentages. Differences in haemodynamic and Doppler parameters at rest and during exercise were compared with repeated measures analysis of variance. Univariate and multivariate associations of clinical and echocardiographic variables with the endpoint were assessed using a Cox proportional hazards regression analysis. Significant univariate variables (p<0.05) were entered into a multivariate model in a stepwise manner, with entry and retention set at a significance level of less than 0.05. We calculated the model χ2 to examine the incremental prognostic value of the clinical, resting and exercise echocardiographic parameters. Cumulative event-free survival curves were constructed using the Kaplan–Meier method, and differences between curves were tested for significance using the log-rank test. A p value of less than 0.05 was considered to indicate statistical significance. Intraobserver variability was examined in a sample of 10 randomly selected subjects by measuring Doppler echocardiographic parameters three times at each of three stages (ie, resting, 25 W, 50 W). Interobserver variability was examined by comparing the mean values of the Doppler echocardiographic parameters at each of three stages measured by three experienced observers. The intraclass correlation coefficient (ICC) was used as an index of intra and interobserver variability for absolute agreement. An ICC value greater than 0.75 was interpreted as excellent, 0.4–0.75 as fair to good, and less than 0.4 as poor. ICC values for intraobserver and interobserver variability of the Doppler echocardiographic parameters were excellent at the three stages of exercise echocardiography (ICC 0.92, ICC 0.81, respectively).
Follow-up
The endpoint was a composite of death and hospitalisation for HF. The hospitalisation criteria for HF were a hospital stay requiring the management of aggravated dyspnoea or orthopnoea, with evidence of pulmonary congestion on a physical examination or on chest radiography. Follow-up data were obtained by a review of medical records, telephone contact, or information via the Korea National Statistical Office. During 57 months of follow-up, 60 of 197 patients were lost. However, the occurrence of death or HF could be identified in those 60 patients using National Statistical Office data including the disease code.
Results
Baseline characteristics
The mean patient age was 58 years, and 84 (42%) were men. The mean duration since the diagnosis of DM was 9.5±8.1 years. Baseline characteristics are presented in table 1. The mean duration of exercise was 7.8±3.1 min and the median workload was 75 W (range 25–125 W). Reasons for termination of the exercise stress test were leg fatigue due to exhaustion in 140 patients (71%), dyspnoea in 45 (23%) and achievement of the target heart rate in 10 (6%) patients.
Baseline characteristics of the study population
Echocardiographic characteristics at rest and during exercise
At resting left ventricular function, mean LVEF was 67±7%, and diastolic function was normal in 28 (14%) patients, impaired relaxation in 152 (77%) and a pseudo-normalised filling pattern in 17 (9%). The prevalence of echocardiographic left ventricular hypertrophy was 37%. Table 2 shows the haemodynamic and Doppler echocardiographic parameters of the patients throughout exercise and recovery. Left ventricular longitudinal DFR (ΔE′) was evaluated at 25 W of exercise in 197 (100%) patients ranging from −2.0 cm/s to 7.0 cm/s, and at 50 W in 153 (77.7%) patients ranging from −0.5 cm/s to 13.5 cm/s, respectively.
Haemodynamic and Doppler parameters throughout exercise and recovery
Predictors of adverse outcomes
The median follow-up duration was 57 months (range 6–90). Among 197 patients evaluated at 25 W of workload, 18 (9.1%) patients had adverse events (eight cardiovascular deaths, four non-cardiovascular deaths, six hospitalisations for HF). Also, 153 patients evaluated at 50 W of workload had 13 (8.5%) adverse events (four cardiovascular deaths, three non-cardiovascular deaths, six hospitalisations for HF). Univariate and multivariate predictors of adverse events are presented in table 3. Independent predictors of adverse events at 25 W of workload were estimated glomerular filtration rate (eGFR; HR 0.97; 95% CI 0.95 to 0.98; p<0.001), DM duration (HR 1.07; 95% CI 1.01 to 1.14; p=0.018), and ΔE′25 W (HR 0.58; 95% CI 0.40 to 0.85; p=0.005). Independent predictors of adverse events at 50 W of workload were eGFR (HR 0.97; 95% CI 0.95 to 0.98; p<0.001) and ΔE′50 W (HR 0.70; 95% CI 0.50 to 0.99; p=0.044). eGFR and DFR (ΔE′) remained as independent predictors of adverse events with an increase in workload. When patients were classified into two groups according to the median ΔE′25 W and ΔE′50 W values, patients with a lower ΔE′ had significantly worse outcomes than those with a higher ΔE′ (p=0.01, p=0.04 by log-rank test, respectively, figure 2).
Independent predictors of adverse events

Kaplan–Meier estimates of event-free survival according to the median value of the change in early diastolic mitral annular velocities from rest to exercise at 25 and 50 W (ΔE′25 W and ΔE′50 W).
Incremental prognostic value of DFR
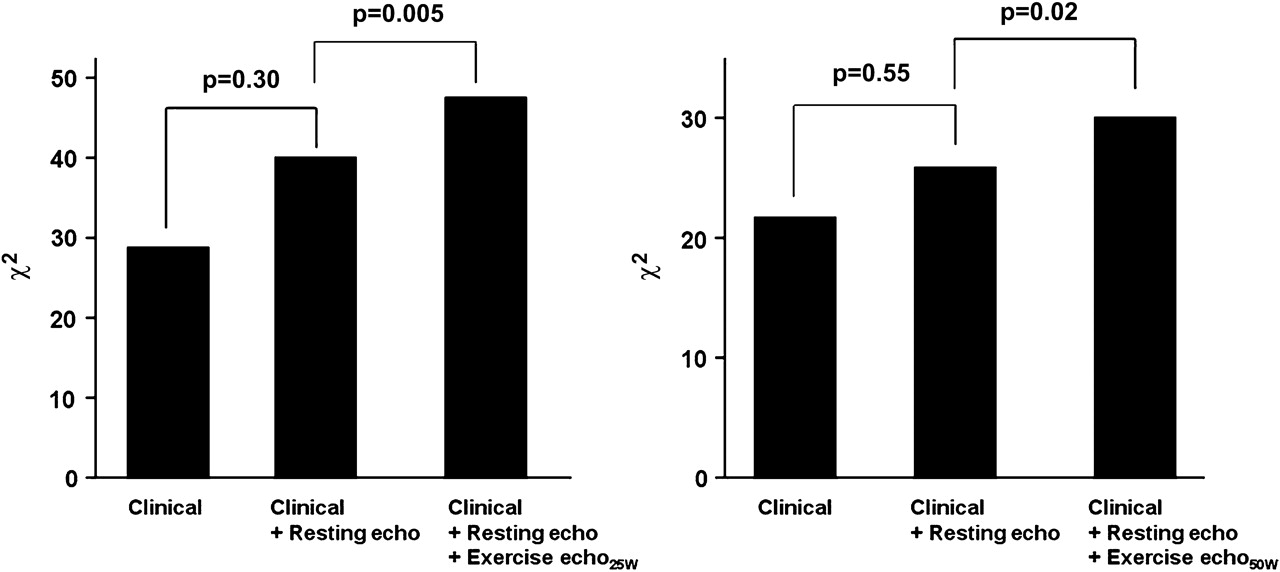
In sequential multivariate models (figure 3), no significant difference was observed for the overall χ2 values when adding the resting left ventricular function to the clinical data in both groups. However, adding the stress echo data to the clinical data and resting left ventricular functional parameters significantly increased the χ2 value at 25 W of workload (p=0.005) and at 50 W of workload (p=0.02), indicating the incremental prognostic value of diastolic stress echocardiography.

{kind=link}
{kind=link}
{kind=link}
Incremental value (expressed on the y-axis as χ2 values) of diastolic stress echocardiography in addition to clinical and resting echocardiographic data for predicting adverse events.
Discussion
The principal findings of this study were that left ventricular longitudinal DFR, as assessed by the change in E′ during exercise, was an independent predictor of adverse events in patients with type 2 DM but without overt heart disease, and that diastolic stress echocardiography showed incremental prognostic value in addition to clinical data and resting left ventricular functional parameters. The present study is the first to demonstrate the prognostic impact of left ventricular longitudinal DFR in patients with type 2 DM without overt heart disease.
Prognostic value of diastolic stress echocardiography
The absolute numbers of patients with DM and subclinical left ventricular dysfunction are increasing with the rapidly increasing prevalence of DM.16 Given that the presence of subclinical cardiovascular disease and DM are associated with an increased risk of death and clinical cardiovascular disease,17 risk stratification should be considered, even for patients at low risk. In this population, the clinical parameters with independent associations to adverse events were eGFR and DM duration, consistent with previous findings that chronic kidney disease and longer duration of DM have significant associations with all-cause and cardiovascular mortality in patients with DM.18 19 However, resting left ventricular functional parameters did not show any incremental prognostic impact above the clinical data. When the stress echo data were added to the model with clinical data and resting left ventricular functional parameters, the model fit for predicting adverse events improved significantly, indicating the incremental value of diastolic stress echocardiography for risk stratification in these patients.
Although we could not assess the DFR during maximal exercise because of the summation of mitral annular velocity with increasing heart rate, we demonstrated that DFR, even at low exercise levels, provided independent prognostic information for predicting adverse events in patients with DM without overt heart disease.
Impaired DFR in patients with DM
Several clinical and experimental studies have suggested that abnormal myocardial function in patients with DM is due to multifactorial mechanisms, including disturbances in myocyte metabolism, autonomic dysfunction, alterations in structural proteins and interstitial fibrosis.1 2 20 Myocardial fibrosis is the main histopathological finding in diabetic heart disease and is related to increasing myocardial wall stiffness,2 21 22 which is thought to contribute to the high prevalence of diastolic dysfunction in these patients. Most patients with DM and early myocardial disease have a wide spectrum of diastolic dysfunction with unknown clinical significance, and myocardial dysfunction may be concealed by various compensatory mechanisms at rest.23 Therefore, an assessment of left ventricular performance during exercise helps reveal left ventricular systolic and diastolic functional abnormalities that are not evident at rest.24 During exercise, patients with DM have an impaired haemodynamic response that manifests as a blunted response in heart rate and blood pressure, and a reduced exercise capacity.25–27 The impaired haemodynamic response in patients with DM is attributed to autonomic dysfunction,25 26 and the reduced exercise capacity in patients with DM is related to left ventricular diastolic dysfunction.27 28 Practically, an assessment of maximal exercise capacity is difficult in a considerable number of older patients with DM, obesity or degenerative arthritis. Although only 22% of patients were on β-blockers, most of the patients did not reach the target heart rate by early termination before achieving maximal exercise due to leg fatigue. Also, the summation of Doppler parameters during tachycardia contributed to the difficulty in assessing left ventricular performance at maximal exercise.
A plausible explanation for the change in E′ as an indicator of DFR is that E′ is a less load-dependent index of left ventricular relaxation.29 In normal individuals, E′ is augmented during exercise by increased sympathetic tone.30 However, it remains unchanged despite an increased transmitral gradient during exercise in subjects with significant diastolic dysfunction.29 Another explanation is that because longitudinal myocardial function is controlled by subendocardial fibres, which are vulnerable to ischaemia and interstitial fibrosis, the change in E′ may be a sensitive marker of subclinical myocardial dysfunction.7 21 31 Recent studies using myocardial velocities, strains and strain rates have demonstrated that left ventricular functional reserve is impaired during pharmacological or exercise stress in patients with DM but without CAD.6–9 Few studies have demonstrated the clinical impact of impaired left ventricular functional reserve in patients with DM. In this study, DFR was found to be a sensitive marker of diastolic dysfunction and remained an independent predictor of adverse events in patients with type 2 DM without overt heart disease. Our results emphasise the prognostic importance of the early identification of left ventricular dysfunction, and that more aggressive strategies for screening patients who are at risk are mandatory to prevent a progression to clinically overt heart disease.
Study limitations
The main limitation was a selection bias that excluded patients with CAD, which may have limited the ability to extrapolate these results to the general population with DM. Small numbers of events in our population may have constrained statistical power by overfitting. This also has a relationship to patient characteristics with a low risk, and further studies with more patients and longer follow-up are needed to confirm our results. Although patients with angina, a history of CAD, inducible ECG changes, or rest or stress wall motion abnormalities were ineligible, the likelihood that CAD could not be excluded by the limited sensitivity of stress echocardiography in patients undergoing submaximal exercise, and the potential influence of coronary microvascular dysfunction, could not be entirely excluded either. Hypertension is independently associated with impaired left ventricular functional reserve, and shows a negative effect on left ventricular systolic and diastolic function.6 Therefore, it may not be easy to tease out the exact impact of hypertension on DFR in this study, although no significant difference in left ventricular DFR was observed in patients with or without hypertension.
We only measured septal mitral annular velocities, and neither longitudinal functional reserve at the lateral mitral annulus nor the average of both annuli was assessed.
Conclusions
In patients with type 2 DM without overt heart disease, left ventricular longitudinal DFR during exercise provided prognostic information incremental to clinical and echocardiographic variables under resting conditions, emphasising the need for more aggressive strategies to identify myocardial dysfunction early and to prevent progression to overt heart disease.
References
Footnotes
Funding This work was supported by the Korea Science and Engineering Foundation (KOSEF) grant funded by the Korean government (M10642120001-06N4212-00110).
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the institutional review board of Yonsei University College of Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.