Article Text

Abstract
Objective To analyse characteristics and outcomes of infective endocarditis (IE) on bicuspid aortic valves (BAV) and to compare the risk of death according to the presence or absence of BAV.
Design 5-year observational study.
Setting Population of 856 patients with definite IE according to the Duke criteria from two tertiary centres (Amiens and Marseille, France).
Patients 310 consecutive patients with definite native aortic valve IE enrolled between 1991 and 2007.
Interventions Patients underwent transthoracic and transoesophageal echocardiography during hospitalisation. Surgery was performed on a case-by-case basis according to conventional guidelines.
Main outcome measures In-hospital mortality and 5-year overall mortality.
Results Patients with BAV IE (n=50, 16%) were younger, had fewer comorbidities and a higher frequency of aortic perivalvular abscess (50%). Presence of BAV (OR 3.79 (1.97–7.28); p<0.001) was independently predictive of abscess formation. Early surgery was performed in 36 BAV patients (72%) with a peri-operative mortality of 8.3%, comparable to that of patients with tricuspid aortic valve IE (p=0.89). BAV was not independently predictive of in-hospital mortality (OR 0.89 (0.28–2.85); p=0.84) or 5-year survival (HR 0.71 (0.37–1.36); p=0.30). Age, comorbidities, heart failure, Staphylococcus aureus and uncontrolled infection were associated with increased 5-year mortality in BAV patients.
Conclusion BAV is frequent in adults with native aortic valve IE. Patients with BAV IE incur high risk of abscess formation and require early surgery in almost three-quarters of cases. IE is a severe complication in the setting of BAV and warrants prompt diagnosis and treatment.
- Bicuspid aortic valves, infective endocarditis
- outcome
- surgery
- surgery-valve
- echocardiography (transoesophageal)
- endocarditis
- aortic valve disease
Statistics from Altmetric.com
- Bicuspid aortic valves, infective endocarditis
- outcome
- surgery
- surgery-valve
- echocardiography (transoesophageal)
- endocarditis
- aortic valve disease
There is increasing awareness that patients with bicuspid aortic valves (BAV) are at high risk for cardiovascular complications such as aortic valve dysfunction,1–3 infective endocarditis (IE),4 ascending aortic aneurysm5–7 and aortic dissection.8 9 As BAV is the most common congenital cardiac abnormality,10–12 the frequency of cardiac and vascular events associated with BAV might be greater than the combined cardiovascular morbidity of all other congenital heart diseases.1 High rates of cardiovascular adverse events in adults with BAV have been recently reported by two large studies.13 14
Despite undeniable improvement in medical and surgical management over the last decades, IE remains a life-threatening condition and a challenge for the treating physician. Clinical characteristics and prognosis of IE in adults with BAV remain poorly defined. To our knowledge, only two studies have specifically addressed the issue of BAV complicated by IE.4 15 These reports included few patients15 and provided few outcome data.4 15 Therefore, we performed an analysis of our registry including consecutive patients with definite IE according to the Duke criteria, prospectively enrolled between 1991 and 2007 in two French referral centres (Amiens and Marseille). Our aims were to describe the clinical characteristics of patients with BAV IE and to analyse the risk of death according to the presence or absence of a BAV.
Methods
Patients
Between January 1991 and May 2007, we prospectively enrolled 856 consecutive patients with definite IE according to the Duke criteria16 referred to the echocardiography laboratories of two French referral centres (University Hospital of Amiens and University Hospital of Marseille). All patients were examined by transthoracic echocardiography (TTE) and transoesophageal echocardiography (TEE). Patients without native aortic valve involvement (mitral valve IE, prosthetic valve IE and right-sided IE) were excluded. The study population comprised 310 patients with aortic valve IE (isolated aortic IE in 221 cases—71%; aortic and mitral IE in 89 cases—29%). Blood culture results were obtained from bacteriology laboratories and comprised identification of pathogens and antibiotic susceptibility testing. Two hundred and seventy-two patients (88%) had positive blood cultures, and 38 (12%) had negative blood cultures. Among patients with positive blood cultures, in 149 patients (55%), streptococcal IE was identified, 47 patients (17%) had Staphylococcus aureus IE, 31 patients (11%) had enterococcal IE, 18 patients (7%) had Staphylococcus epidermidis IE, and 27 patients (10%) had IE due to uncommon micro-organisms. Among the 38 patients with negative blood cultures, 14 had previously received antibiotic therapy, and six operated patients had positive valve cultures. All patients were scheduled to receive antibiotics for at least 4 weeks, according to susceptibility testing.
Clinical parameters
Age, sex, presence of comorbidity (history of diabetes, cancer, renal failure, hypertension) and history of valvular heart disease were recorded. The Charlson comorbidity index17 was computed for each patient. The Charlson index takes into account both the age and the comorbid diseases (number and seriousness) of the patient.17 The following acute clinical events present on admission or occurring during hospitalisation were also recorded: heart failure, neurological events, peripheral embolism and uncontrolled infection. Heart failure during the initial hospitalisation was diagnosed according to Framingham criteria.18 The diagnosis of embolism was based on clinical signs and data derived from non-invasive procedures (cerebral and thoraco-abdominal computed tomography scan performed in 70% of patients).19 A major neurological event was defined by the development of ischaemic stroke with hemiplegia, haemorrhagic stroke, cerebral abscess, features of encephalopathy or coma.20–22
Echocardiography
Echocardiography was performed on ultrasound machines using 2.5-MHz TTE transducers and 5-MHz TEE transducers. TTE was systematically completed by TEE. All echocardiographic studies were performed according to standard techniques by experienced echocardiographers during the acute phase of IE without complications. Diagnosis of BAV was based on TEE short-axis (40–60°) views of the aortic valve showing the existence of only two commissures delimiting two aortic valve leaflets. The presence, size, sites of valvular vegetations or perivalvular abscesses were evaluated.19 Standard definitions were used for vegetations, abscesses or other infective cardiac lesions. All TEE recordings were reviewed by an experienced echocardiographer to measure the maximum length of vegetations in various planes. The mobility of vegetations was graded from 1 to 4, with severe mobility corresponding to grade 4.23 Aortic valvular regurgitation was quantified by Doppler echocardiography using standard methods.21
Follow-up
Follow-up data included surgical treatment and death occurring during hospitalisation or follow-up. Surgical therapy was indicated on a case-by-case basis, according to the judgement of a multidisciplinary team (cardiologist, neurologist, radiologist and cardiac surgeon) in agreement with conventional guidelines,24 predominantly the presence of complications such as embolism, large vegetations, heart failure, uncontrolled infection, severe regurgitation or perivalvular abscess.
Early surgery was defined as surgery performed within 30 days after the diagnosis of IE.25 Peri-operative mortality was defined as any death occurring during the initial hospitalisation or within 30 days of operation for discharged patients.26 In-hospital mortality was defined as death occurring during the hospitalisation for IE.25 Five-year mortality was defined as death occurring during the hospitalisation for IE or during the first 5 years after the hospitalisation for IE.
Statistical analysis
Statistical analysis was performed with SPSS 13.0 (SPSS Inc and S-Plus 8.0 (Insightful Inc., Seattle, Washington, USA)). Continuous variables were expressed as mean (SD) and were compared between groups by Student t tests. Categorical variables were summarised by frequency percents and analysed by χ2 tests or Fisher exact tests for binary variables, as appropriate. Survival curves were generated by the Kaplan–Meier method and compared using a two-sided log-rank test. Mortality analyses were conducted to assess the impact of BAV on short-term and long-term mortality. Logistic regression models were used for the multivariable analyses of in-hospital and peri-operative mortality. Univariate and multivariable analyses of 5-year mortality were performed using Cox proportional hazards models. Multivariable analyses were systematically adjusted for the main prognostic factors on the basis of epidemiological knowledge (ie, comorbidity index, uncontrolled infection, heart failure, embolic event, abscess, and early surgery). Early surgery was entered in the Cox models as a time-dependent covariate. Adjusted survival curves were used to graphically illustrate results of multivariable Cox analyses. The proportional hazards assumption and the assumption of linearity were confirmed using statistics and graphs based on the Schöenfeld residuals. For all analyses, a p value <0.05 (two-sided) was considered statistically significant.
Ethics
The study conforms to the principles outlined in the Declaration of Helsinki and was approved by local institutional review boards. Informed consent was obtained from the patients before entering data into the electronic database.
Results
Characteristics of patients with BAV IE
Among the 310 included patients with aortic valve IE (253 men and 57 women; mean age: 59 (15) years), a BAV was identified in 50 patients (16.2%). In a large majority of patients with BAV IE (92%, n=46), the presence of a BAV was incidentally discovered at the time of IE diagnosis. Baseline characteristics, overall and according to the presence of a BAV, are presented in table 1. In the total population, vegetations were visualised in 91% of cases, and a perivalvular abscess was identified in 25% of patients. IE affected solely the aortic valve in 71% of cases and both mitral and aortic valves in 29% of cases. Heart failure was present in 121 patients (39%), severe valvular regurgitation in 200 patients (65%), embolic events in 133 patients (43%), neurological events (stroke and transient ischaemic attack (TIA)) in 62 patients (20%) and uncontrolled infection in 39 patients (13%). Streptococcus was the microorganism responsible for IE in 48% of patients, and S aureus was isolated in 15% of cases. Patients in whom an abscess was identified were younger (54 vs 60 years, p=0.002), had more often BAV (33% vs 11%, p<0.001), less frequently vegetations on echocardiography (78% vs 95%, p<0.001) and more often received antibacterial agents before hospitalisation (25% vs 14%, p=0.02). Comorbidity index was comparable in patients with and without abscesses (2.2 vs 2.7, p=0.10). Staphylococcus was more frequently identified in aortic IE complicated by abscess (34% vs 17%, p=0.001), whereas Streptococcus was responsible for the majority of cases of IE without abscess (53% vs 33%, p=0.002). Early surgery was significantly more often performed in the presence of an abscess (82% vs 57%, p<0.001).
Baseline clinical characteristics of the study population, overall and according to the presence or absence of a BAV
Compared with the group of patients with IE on tricuspid aortic valves (TAV), the 50 patients with BAV IE were significantly younger (45 (16) vs 61 (14) years; p<0.001) and had lower comorbidity index (1.6 vs 2.8; p=0.003). The delay between the onset of symptoms and the diagnosis of IE in BAV patients was not significantly different from that observed in patients with TAV IE (57 (109) vs 48 (58) days; p=0.55). Clinical examination identified less often a new heart murmur in patients with BAV. Echocardiography showed the presence of a perivalvular abscess in 50% of BAV cases compared with 20% of patients with TAV IE (p<0.001; table 1). On multivariable logistic regression, the presence of BAV (odds ratio (OR) 3.79 (1.97–7.28); p<0.001) and uncontrolled infection (OR 1.89 (1.10–4.02); p=0.04) were the two independent predictors of abscess formation. Clinical and echo findings, as well as complications and rates of early surgery, were similar in patients with abscess on BAV and patients with abscess on TAV.
With regard to microbiological characteristics, patients with BAV IE received more often antibacterial agents before the index admission for IE (p=0.005), had a higher frequency of negative blood cultures (p=0.006) and less often presumed bacteraemia of gastrointestinal origin (p<0.001) compared with the TAV group. Streptococcus was the most frequently encountered pathogen in patients with BAV IE (34% of cases) followed by Staphylococcus (20% of patients). However, in BAV patients the frequency of Streptococcus IE and Enterococcus IE were lower compared with patients with TAV. The complication rate (with the exception of abscess formation) was comparable between patients with BAV and TAV IE (table 1). Early surgery tended to be more frequently performed in patients with BAV IE (72% vs 61%; p=0.15).
Prognosis and factors influencing survival in BAV IE
In-hospital mortality
Thirty-seven patients died during the index hospitalisation for IE (12%) in the overall cohort. In-hospital mortality was similar in IE patients with BAV and TAV (10% vs 12.3%; p=0.63). After adjustment for the prognostic factors, BAV was not independently associated with in-hospital mortality (OR 0.89 (0.28–2.85); p=0.84). Uncontrolled infection (OR 5.08 (2.10–12.3); p<0.001) and heart failure (OR 2.33 (1.02–5.29); p=0.044) were independently predictive of in-hospital mortality. Five patients (10%) with BAV IE died during the index hospitalisation. The causes of death were: severe sepsis complicated with multiple organ failure in three cases, postoperative myocardial infarction with cardiogenic shock in one case and stroke in one patient. On univariate analysis, older age (p=0.006), diabetes mellitus (p=0.002), heart failure (p=0.03), renal failure (p=0.01), uncontrolled infection (p=0.001) and S aureus IE (p=0.016) were factors associated with in-hospital mortality in patients with IE on BAV.
Early surgery was performed in 36 of the 50 patients with BAV IE (72%) on the basis of the following main indications: heart failure due to severe aortic regurgitation in 47% of cases (n=17); abscess in 8% of cases (n=3); large vegetations with embolic risk in 6% of cases (n=2) and uncontrolled infection in 3% of cases (n=1). In 25% of cases (n=9), there were two indications for surgery (heart failure due to aortic regurgitation associated with either abscess or large vegetations), and four patients (11%) had ≥3 indications for surgery. Compared with medically managed patients with BAV IE (n=14), patients with BAV IE who underwent early surgery had echocardiographic markers of more severe valvular and perivalvular lesions (table 2). Among these 36 operated patients, aortic valve repair was performed in two cases, while 34 patients underwent aortic valve replacement (mechanical prostheses in 14 cases, bioprostheses in six cases, and aortic homografts in 14 cases). Aortic valve repair was performed in two patients with BAV IE. Both patients were young, had thin aortic leaflets with leaflet perforation and mild-to-moderate aortic regurgitation. There was no evidence of perivalvular involvement on TEE. Surgical approach consisted in closure of the defect with a pericardial patch and commissuroplasty. The patients were discharged in good condition with only mild aortic regurgitation at TTE. Both patients were alive after 5 years. Three operated patients with BAV IE (8.3%) died during the peri-operative period (multiple organ failure in two patients and postoperative myocardial infarction in one case). On univariate analysis, comorbidity index (p=0.017), diabetes mellitus (p=0.014), uncontrolled infection (p=0.027), and S aureus IE (p=0.06) were factors associated with peri-operative death in patients with BAV IE. Peri-operative mortality of patients with BAV IE was not significantly different from that of patients with TAV IE (8.3% vs 7.5%, p=0.89). On multivariable analysis, the presence of a BAV was not associated with increased peri-operative mortality (OR 1.39 (0.29–6.81); p=0.68).
Comparison of baseline characteristics of patients with IE on BAV according to the therapeutic strategy (medical management or early surgery)
Five-year outcome
The overall 5-year estimated survival of the 310 patients with aortic valve IE was 64 (3)% (figure 1A). Fifty-six deaths occurred during post-discharge follow-up in the overall cohort. Older age (p<0.001), greater comorbidity index (p<0.001), diabetes mellitus (p=0.012), renal failure (p<0.001), cancer (p=0.002), presence of severe regurgitation (p=0.035), S aureus IE (p<0.001) and uncontrolled infection (p<0.001) were univariate predictors of 5-year mortality. Streptococcus IE was associated with better prognosis (p=0.003). Patients who underwent early surgery had improved 5-year outcome (p=0.002). Uncontrolled infection (hazard ratio (HR) 2.84 (1.74–4.65); p<0.001), heart failure (HR 1.35 (0.98–1.93); p=0.052) and comorbidity index (HR 1.17 (1.08–1.25); p<0.001) were independently predictive of poorer 5-year survival. Early surgery was independently associated with improved 5-year survival (HR 0.96 (0.93–0.98); p=0.006).
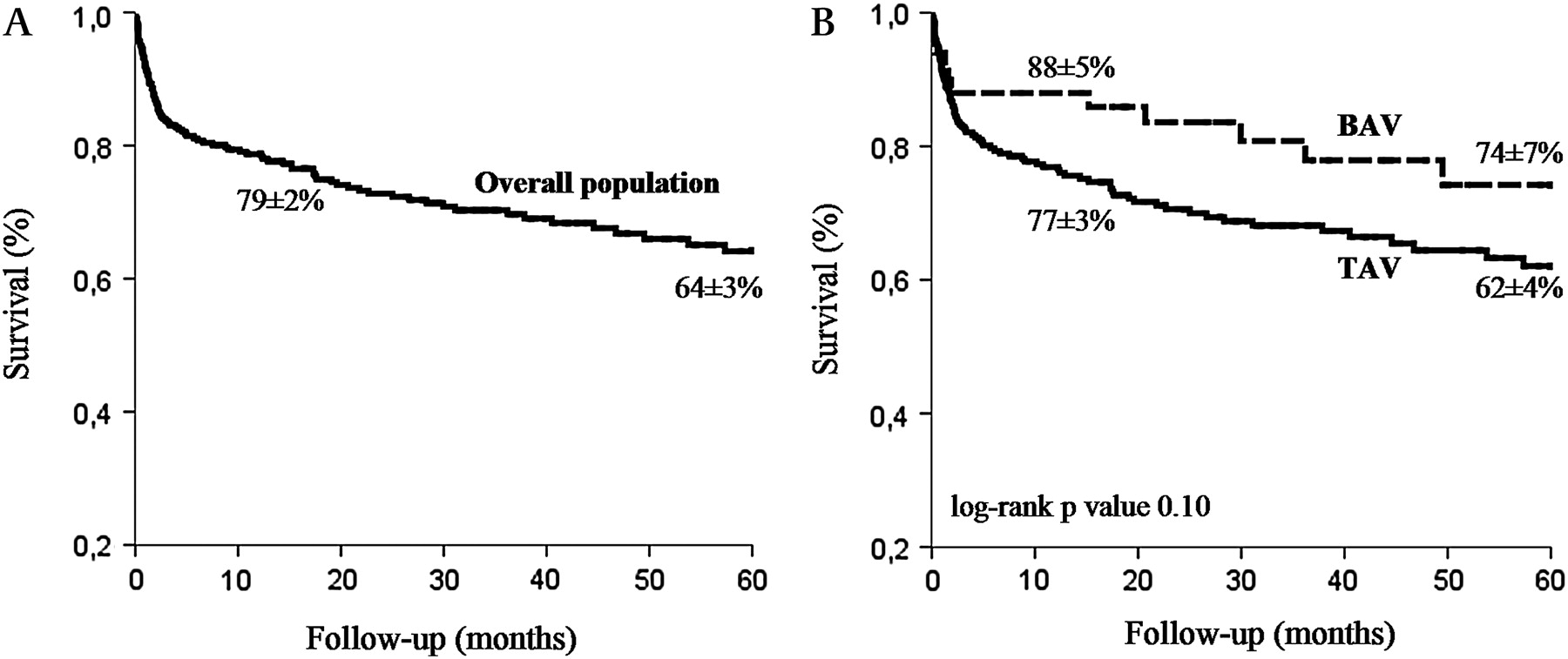
Kaplan–Meier survival curves of patients with aortic valve IE, overall (A) and according to the presence or absence of BAV (B). Patients with BAV IE had slightly higher although not significantly different 1-year (p=0.11) and 5-year (p=0.10) survival rates compared with the group with TAV IE. BAV, bicuspid aortic valve; IE, infective endocarditis; TAV, tricuspid aortic valve.
Compared with the 1- and 5-year estimated survival of patients with TAV IE, 1- and 5-year estimated survival tended to be better in the BAV group, although the difference did not reach statistical significance (88 (5)% vs 77 (3)%; p=0.11 and 74 (7)% vs 62 (4)%; p=0.10, respectively—figure 1B). After adjustment for age, there was no difference in 5-year survival between the two groups (HR 0.96 (0.49–1.89); p=0.90—figure 2A). Five-year survival remained comparable (HR 0.75 (0.40–1.41); p=0.37—figure 2B) between the two groups after adjustment for comorbidity index (including age). On Cox multivariable analysis, BAV did not emerge as an independent predictor of improved 5-year survival (HR 0.71 (0.37–1.36); p=0.30). Six deaths were recorded in patients with IE on BAV during post-discharge follow-up: two deaths were sudden, one patient died of heart failure, one of stroke, and there was one non-cardiovascular death. In one patient, the cause of death was unknown. During follow-up, recurrence of IE occurred in two patients in the BAV group (one case occurred in a patient who did not undergo surgery during the index hospitalisation, and the second patient developed prosthetic aortic valve IE). No redo surgery was performed. On univariate analysis, older age (p=0.014), greater comorbidity index (p=0.005), diabetes mellitus (p=0.003), heart failure (p=0.039), S aureus IE (p=0.001), and uncontrolled infection (p<0.001) were associated with increased 5-year mortality in patients with BAV.

{kind=link}
{kind=link}
Adjusted survival in patients with aortic valve IE according to the presence or absence of BAV: (A) Cox proportional analysis adjusted for age; (B) Cox proportional analysis adjusted for comorbidity. BAV, bicuspid aortic valve; IE, infective endocarditis; TAV, tricuspid aortic valve.
Discussion
The current study provides novel insights on the features and outcome of IE in patients with BAV. We report for the first time long-term outcome in BAV complicated by IE. According to our results, in adults with aortic valve IE, BAV is frequently the underlying valvular abnormality. BAV IE occurs more often in young individuals with few associated diseases and leads to severe valvular and perivalvular destructive lesions (aortic abscess in 50% of patients). Although BAV IE is associated with a relatively high rate of negative blood cultures due to antibacterial treatment administered before hospitalisation, in patients with positive blood cultures the most frequently encountered pathogen is Streptococcus. In-hospital mortality in BAV IE is not significantly different from that of TAV IE. Almost 75% of patients with BAV IE undergo valvular surgery with a peri-operative mortality of about 8%. After adjustment for age, patients with BAV and TAV IE have similar 5-year mortality. Age, comorbidity, heart failure, S aureus IE and uncontrolled infection are associated with long-term mortality in patients with BAV.
BAV is the most common congenital cardiac anomaly with an incidence between 0.5% and 2% and a clear male predominance.10–12 Although quite often BAV is an incidental echocardiographic finding, numerous reports suggest that patients with BAV are at increased risk for cardiac and vascular complications.1–9 13 14 In a recently published series of adults with BAV, Tzemos et al14 reported a 25% cardiac event rate during a mean follow-up of 9 years. Michelena et al13 observed that 33% of asymptomatic residents from Olmsted County, Minnesota with normal or minimally dysfunctional BAV have incurred cardiovascular medical events over a 20-year follow-up with cardiac or vascular surgery rates as high as 27%. The presence of BAV dysfunction at diagnosis was associated with increased event rates in both studies.13 14 Previous small necropsy and surgical series have suggested that 25% to 50% of all infected aortic valves were bicuspid.27 28 In the study by Lamas and Eykyn, BAV IE represented 12% of patients with native valve IE.4 Kahveci et al have reported 22 cases of BAV IE (43%) among 51 patients with definite aortic IE in a recent retrospective study.15 In our cohort of 310 patients with aortic valve IE, a BAV was identified in 16% of cases. In the study by Tzemos et al including 642 adults with BAV, IE occurred in 13 patients during a 9-year follow-up,14 while in the Olmsted County study, 4 out of 212 patients with BAV developed IE during a follow-up of 20 years.13 In our experience, we observed four cases of IE (2.7%) among 148 patients with echocardiographically diagnosed BAV between January 2005 and May 2009 at our tertiary centre (Amiens University Hospital, France). All four patients had significant regurgitation (moderate to severe in two cases and severe in two cases) and underwent aortic valve replacement (unpublished data). These observations suggest that the risk of IE in adults with BAV is rather low, whereas BAV is common in cases with confirmed aortic valve IE.
Features of IE in patients with BAV have not been previously well characterised as very few studies specifically addressed this issue.4 Patients with BAV IE in the present series were young, mostly men and had relatively few associated diseases. As in the study by Lamas and Eykyn,4 Streptococci were the most frequently identified pathogens, followed by Staphylococci. However, the frequency of Streptococcus IE in BAV patients was lower compared with patients with TAV. The 24% rate of negative blood cultures was high in our BAV patients, probably due to empiric pre-hospital antibacterial treatment administered in 28% of BAV patients. Compared with previous studies4 15 that did not systematically use TEE, all our patients had a comprehensive TEE examination to establish the characteristics of the aortic valve (bicuspid or tricuspid), to define IE destructive lesions and to quantify the severity of these lesions. Destructive IE lesions (valvular regurgitation, perforation and abscess) were frequent in BAV IE. Thus, a peri-valvular abscess was identified in 50% of our BAV IE patients compared with 30% in the study by Lamas and Eykyn.4 Periannular complications were observed in 14 of the 22 patients with BAV IE (64%) in the report by Kahveci et al.15 Moreover, we found that the presence of a BAV was independently associated with abscess formation in aortic valve IE. This finding is important as patients with aortic valve IE complicated by peri-valvular abscesses are more likely to undergo surgery.29 Current European guidelines on the prevention, diagnosis, and treatment of IE from 200930 recommend TEE in most adults with suspected IE even in the presence of a positive TTE exam due to its higher sensitivity and specificity for the diagnosis and assessment of intracardiac lesions (class IIa, level of evidence C). Given the high frequency of perivalvular abscesses in BAV IE, our study supports systematic use of TEE in all BAV patients in whom IE is suspected on clinical and laboratory data, irrespective of TTE findings. The explanation for the propensity of BAV patients to develop perivalvular lesions remains poorly understood. It might be related to a morphologically abnormal aortic wall with increased susceptibility to infection. As abscesses generally occur late in the course of IE, one could suspect that empirical antibacterial therapy administered before the diagnosis of IE in BAV patients rendered symptoms and signs less obvious and contributed to a delayed diagnosis. However, according to our results, we cannot conclude that the high rate of abscesses in BAV IE patients is a consequence of a delayed diagnosis as the time interval between symptoms onset and diagnosis was not significantly different in BAV and TAV patients. We cannot exclude the presence of more aggressive pathogens in BAV IE patients with negative blood cultures leading to extensive valvular and perivalvular lesions. Uncontrolled infection and heart failure were frequent in our series, occurring in 16% and 32% of patients with BAV, respectively.
IE is still associated with high in-hospital mortality rates, ranging between 15% and 20% in recent series.31 Surgical therapy is currently performed in about 50% of cases of IE and is associated with improved survival.31 Patients with BAV IE seem to have lower in-hospital and peri-operative mortality rates (10% and 8%, respectively), probably due to the younger age of this group. Despite this more favourable in-hospital outcome, BAV IE remains a serious disease requiring surgery in almost 75% of cases. This high rate of surgical therapy reflects the serious local and systemic complications in BAV IE and also the fact that this group of patients is relatively free of severe comorbidities which might lead to a prohibitive operative risk. The 5-year survival in patients with BAV IE was slightly better compared with the survival of the TAV IE group. After adjustment for age, comorbidity and other classical prognostic factors, 5-year outcome was similar in patients with BAV and TAV IE. The comparable long-term outcome of BAV and TAV IE suggests that, despite the younger age and lower comorbidity, patients with BAV IE do not have a benign prognosis and require prompt assessment of valvular and perivalvular lesions with TEE and, on a case-by-case basis, early surgery.
We cannot rule out the possibility that our patients might represent a selected cohort from referral centres with more severe disease than the average population. In this observational study, the decision to perform early surgery was based on the clinical judgement of the medico-surgical team according to conventional guidelines. The number of BAV IE cases might have been underestimated in our cohort as some patients with echocardiographically diagnosed BAV did not undergo surgery. However, the diagnosis of BAV was based on TEE (systematically performed in all patients), and the characteristics of the aortic valve, as assessed by TEE (bicuspid or tricuspid), were confirmed by the surgeon in all operated patients. In our study, the presumed origin of bacteraemia was identified based on history, clinical data and paraclinical exams performed at the time of IE diagnosis. Any pathological states, lesions or previous invasive procedures that might have been associated with IE were considered as a “presumed” origin of bacteraemia. Thus, patients with presumed origin of bacteraemia did not necessarily have gastrointestinal, upper respiratory tract or urinary procedures before the diagnosis of IE. The appropriateness of antibacterial prophylaxis at the time of invasive procedures potentially responsible for bacteraemia was not assessed and is therefore unavailable in our database.
Conclusion
BAV is a frequent finding in adults admitted to hospital for aortic valve IE. BAV IE is associated with severe complications and significant in-hospital mortality. Half of patients with BAV IE develop a peri-valvular abscess, and almost three-quarters require early surgery. Although the risk of developing IE seems relatively low in adults with BAV, BAV IE is a serious disease requiring preventive measures as specified by the recent IE guidelines.30 Individuals with BAV need to be aware of the risk of developing IE, and in case of fever of unexplained origin, blood cultures should be performed. Due to the high frequency of peri-valvular destructive lesions, TEE is mandatory in this form of IE.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the Local institutional review boards.
Provenance and peer review Not commissioned; externally peer reviewed.