Article Text

Abstract
Objectives To investigate long-term efficacy of catheter ablation for atrial fibrillation (AF) and the impact of ablating complex or fractionated electrograms (CFEs) in addition to pulmonary vein isolation and linear lesions in persistent AF (PeAF).
Methods Consecutive cases from 2002–2007 were analysed. All the patients underwent a wide-area circumferential ablation with confirmation of electrical isolation. For PeAF, linear lesions were added, with additional targeting of CFE from 2005. Data were collected in a prospective database. Attempts were made to contact all patients for follow-up.
Results 285 patients underwent 530 procedures. The mean (SD) age was 57 (11) years, 75% were male, 20% had structural heart disease and 53% had paroxysmal AF (PAF). The mean number of procedures was 1.9 per patient (1.7 for PAF and 2.0 for PeAF). Procedural complications included stroke or transient ischemic attack in 0.6% and pericardial effusion requiring drainage in 1.7%. During 2.7 years (0.2 to 7.4 years) of follow-up from the last procedure, there were seven deaths (unrelated to their ablation or AF) and three strokes or transient ischemic attack (0.3% per year). Freedom from AF/atrial tachyarrhythmia was 86% for PAF and 68% for PeAF. Late recurrence was 3 per 100 years of follow-up after >3 years. The Kaplan–Meier analysis showed that CFE ablation improved the outcome for PeAF after the first cluster of procedures (p=0.049), with a trend towards improved final outcome (p=0.130).
Conclusions Long-term freedom from AF is achievable in most patients with PAF and PeAF with low rates of late recurrence. Additional targeting of CFE improves outcome for PeAF. Late adverse events including stroke are few.
- AF
- catheter ablation
- outcome
- efficacy
- follow-up
- CFE
- radiofrequency ablation (RFA)
- atrial fibrillation
Statistics from Altmetric.com
Catheter ablation (CA) is now successful in restoring sinus rhythm for most patients with paroxysmal (PAF) and persistent AF (PeAF) in the short term, with studies typically reporting freedom from AF or other atrial tachyarrhythmias (ATs) in 70%–90% of patients up to a year.1–6 However, follow-up is often short and success is usually reported after the last procedure, meaning patients with late recurrence who undergo successful repeated procedures are counted as successes. This may distort perception of success and patterns of recurrence.
CA of AF at St Bartholomew's Hospital has consistently used wide-area circumferential ablation (WACA) with confirmation of electrical isolation of the pulmonary veins (PVs) as a procedural end point since 2002.7 For PeAF, additional substrate modification has been performed. This was initially limited to linear lesions but has incorporated targeting of complex or fractionated electrograms (CFEs) since 2005.
It was hypothesised that once sinus rhythm is successfully restored, late recurrence occurring more than a year later is uncommon, as is typically reported for final-procedure success in the literature.3 8–10 To ascertain this, a prospective registry at St Bartholomew's Hospital was analysed to determine long-term success after (1) a single procedure, (2) the first cluster of procedures (ie, from when AF is first successfully eliminated, whether after one procedure or several) and (3) final success. For patients with PeAF, the efficacy of targeting of CFE was evaluated.
Methods
All consecutive patients undergoing CA of AF between 1 April 2002 and 1 June 2007 were included for analysis. All the procedural data and baseline patient information were obtained from a prospective registry. The patients were defined as PAF or PeAF according to the American College of Cardiology/American Heart Association/European Society of Cardiology guidelines.11 The patients with long-standing PeAF have been included with PeAF.
Periprocedural management
If the patients were on warfarin, this was stopped 5 days preprocedure, and the patients self-administered low–molecular-weight heparin (subcutaneous enoxaparin 1.5 mg/kg once daily). The patients underwent transoesophageal echocardiography within 24 h of CA to exclude intracardiac thrombus. The patients were given 5,000 units of unfractionated heparin after insertion of sheaths and a further 5,000 units after trans-septal puncture. Activated clotting time was checked every 30 min and maintained between 300–400 seconds with further heparin boluses. Low–molecular-weight heparin was administered while reloading warfarin.
Catheter ablation of AF
Our technique for CA of AF has been described previously.7 In brief, under local anaesthesia (lidocaine) and conscious sedation (midazolam and diamorphine), a decapolar catheter was inserted into the coronary sinus, and after double trans-septal puncture, a PV mapping catheter and ablation catheter were introduced to the left atrium. The ablation catheters were irrigated with 2 ml/min heparinised saline, increased to ≤30 ml/minute where temperature increase limited energy delivery. Power was limited to 25 W and 50°C near the PV ostia, 30 W and 50°C in the body of the left atrium and 40 W and 45°C at the cavotricuspid isthmus.
All the procedures were guided by three-dimensional mapping systems, either Carto (Biosense Webster, Diamond Bar, California, USA) or Ensite NavX (St Jude Medical, Minneapolis, Minnesota). Since 2004, computed tomography or magnetic resonance imaging was used routinely for image integration.12 13
WACA lesions were placed 1–2 cm outside the PV ostia, isolating them as ipsilateral pairs, with confirmation of electrical isolation. All the patients with PeAF had linear lesions added at the mitral isthmus (between the mitral valve and the left-sided WACA ring), the roof between the WACA rings and the cavotricuspid isthmus in the patients with a history of typical atrial flutter. Block was verified by examining the activation sequence at either side of the linear lesions after restoration of sinus rhythm. From 2005, after WACA and linear lesions if the patient remained in AF, CFEs were systematically targeted throughout the left then right atria. CFEs were identified visually with operators using a common consensus definition: electrograms with (1) prolonged complexes with continuous deflections from baseline, (2) a rapid cycle length (<120 ms) or (3) complexes with multiple deflections (without distinguishing between high- and low-amplitude signals). Examples of what our group consider to be CFE has been published previously.14 If at any point AF organised into AT, this was mapped and ablated. If sinus rhythm was not restored after these lesions, the patient was cardioverted with a DC shock.
Follow-up
The patients were discharged the day after the procedure, having stopped all antiarrhythmic medication. As early recurrences often settle spontaneously, a 3-month blanking period was observed, during which recurrences were managed medically.10 15 Those with PeAF/AT or symptomatic PAF at 3 months were offered a repeated procedure. Anticoagulation was continued for a minimum of 3 months, and ongoing anticoagulation was advised if the CHADS2 score was ≥2 (regardless of rhythm) as per current guidelines.16 17
The patients were followed-up at 3 months and again at 6 months if symptomatic initially, with a period of ambulatory monitoring of 2–7 days (83% were either monitored once since their last procedure or had AF/AT documented on electrocardiogram). There was open access to arrhythmia nurse specialists subsequently and further monitoring prompted by symptoms (29% underwent monitoring >8 months after their last procedure). Late follow-up with an electrocardiogram was obtained from the referring physician for 96% of the patients at a median of 18 months. Attempts were made to contact all the patients for review between 1 September 2009 and 16 October 2009 to determine any adverse events, recurrences of AF/AT, current medications and symptoms. Symptoms were assessed using the recent Canadian Cardiovascular Society Severity of AF (CCS-SAF) scale.18 As this was not available preprocedure, no objective comparison with the preprocedure state is possible, so the patients were asked for a subjective assessment of whether their symptoms were improved.
Measures of success
Success was defined as freedom from symptoms and/or documented AF/AT lasting >30 s after the 3-month blanking period. Success rates are reported after
the first procedure
the first cluster of procedures (defined below)
the last procedure
the last 6 months (to account for those whose symptoms settled with adjustment of medications subsequent to the blanking period).
The end of the first cluster was defined as the point in time, whether after one CA or several, when ablation was first considered a success as defined above (or the patient declined a further procedure). Late recurrence of AF/AT was analysed starting from the last procedure in the cluster because analysis after the final procedure does not take into account late recurrence occurring before successful repeated procedures.
Statistics
Continuous variables are reported as mean (SD) or median (range) if not normally distributed. Continuous data were compared by Student t test. The Kaplan–Meier curves were used to analyse AF-free survival, and the curves were compared using the log-rank test. Multivariate analysis of predictors of recurrence was by Cox regression. The patient factors were analysed for their effect on the success of the final procedure (figure 1A), whereas procedural factors were analysed for their effect on the single-procedure success (figure 1B,C).

Multivariate analysis of factors predicting recurrence of AF. The figures show hazard ratios for recurrence of AF derived from Cox regression analysis, with p values shown to the right. (A) Patient factors predicting recurrence after the final procedure. (B) Procedural factors affecting recurrence after a single procedure. (C) Procedural factors affecting recurrence for patients with PeAF after a single procedure.
Results
Patients and procedures
The analysis included 285 patients aged 56.5 (10.5) years. Fourteen per cent were >65 years of age, and 75% were male. One hundred and fifty-one (53%) had PAF, 134 (47%) had PeAF and most of these (84%) were long-lasting PeAF (ie, continuous for >1 year). Twenty per cent had structural heart disease, 37% had hypertension and 5% previously had stroke or transient ischemic attack (TIA). The left atrial diameter was 4.3 (0.8) cm, and 17% had left ventricular systolic dysfunction (ejection fraction <50%).
In total, 530 procedures were performed, with a mean per patient of 1.9 (1) (1.7 (0.9) for PAF and 2.0 (1.0) for PeAF). One hundred and twenty-two patients had 1 CA, 105 had 2, 41 had 3, 11 had 4, 5 had 5 and 1 had 6. The patients underwent 1.5 (0.7) procedures in their initial cluster, with a further 0.4 ablations for late recurrence. The mean time between procedures in the first cluster was 6.9 months. The mean period between the first cluster of procedures and the ablation for late recurrence was 1.4 years. Of those with recurrent arrhythmia, 70% had AF, 29% had left atrial flutter and 1% had typical right atrial flutter.
The median procedure time was 240 (145–510) min, with fluoroscopy time of 53 (17–120) min. Ablation to sinus rhythm occurred in 12.5% of CA for PeAF. Procedural complications (shown in table 1) included stroke or TIA in 0.6% and pericardial effusion requiring drainage in 1.7%. Of these nine tamponades, two occurred during transseptal puncture, one occurred after a pop was heard while isolating the right-sided veins and six occurred late despite the absence of an effusion on the echocardiogram routinely performed after cases (five within 12 h, and one presented to another hospital at 10 days).
Procedural complications of CA for AF
Follow-up
Of the 285 patients, 15 could not be traced and were excluded from the analysis, leaving 270 patients. Of these, 125 (46%) had PeAF and 145 (54%) had PAF. The patients were followed-up for a median of 3.3 (2.4–7.5) years from their first procedure, 3.1 (1.3–7.5) years from their initial cluster of procedures and 2.7 (0.2–7.4) years from their last procedure.
Adverse events during follow-up
There were seven deaths in the cohort, two of which were cardiac. One occurred at 27 days postprocedure because of myocardial infarction; the other was a sudden cardiac death in a patient with pre-existing heart failure and an implantable cardioverter defibrillator (ICD) in situ >2 years postablation. The non-cardiac deaths were due to three malignancies and two pneumonias complicating pre-existing pulmonary disease. Other adverse events during follow-up included one myocardial infarction, two TIAs and a stroke that resolved without long-term neurological deficit. There were no cases of new onset heart failure. Two patients went on to have AV node ablation and pacemaker implantation.
Freedom from AF
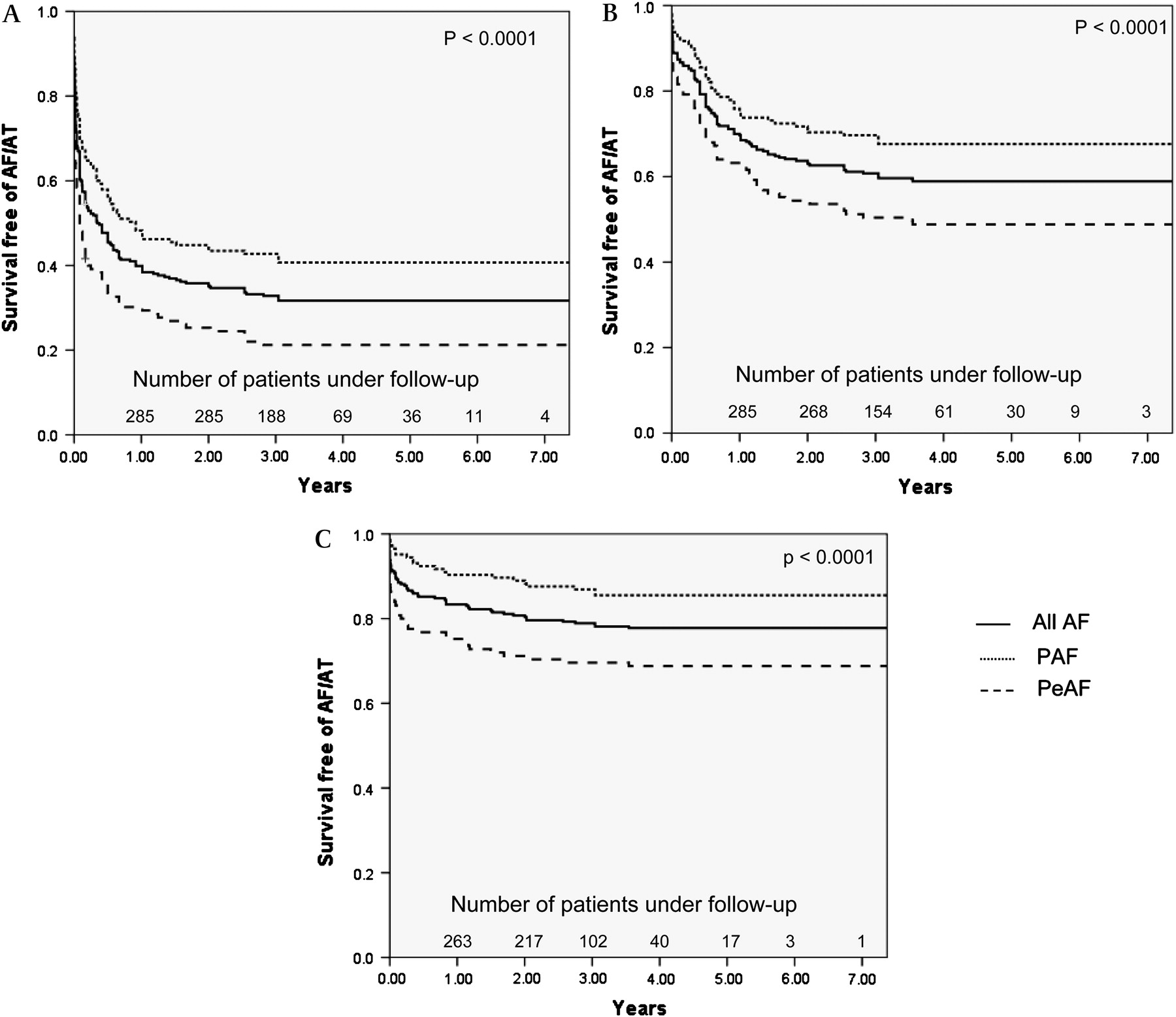
Freedom from AF/AT with and without anti-arrhythmic medication is shown in table 2. AF-free survival was significantly better for PAF than PeAF after the first procedure, the initial cluster and the final procedure (p<0.001 for each; figure 2). There was no difference in success for repeated procedures whether the recurrent arrhythmia was AF (53%) or left atrial tachycardia (47%).
Freedom from AF after CA
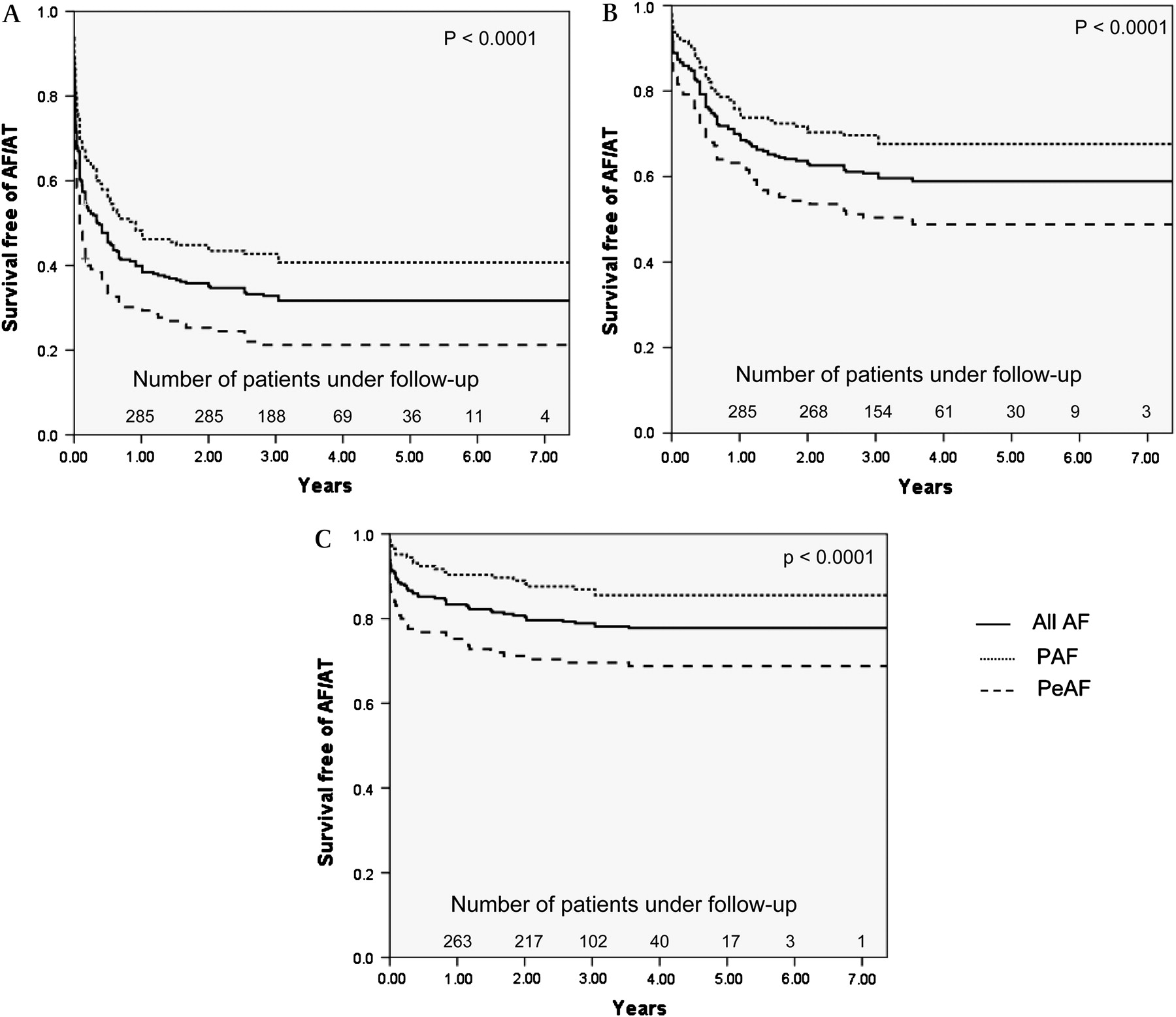
Long-term outcome after CA of AF. The Kaplan–Meier curves showing AF-free survival (A) after the first procedure, (B) after the first cluster of procedures and (C) after the final procedure. Significance was assessed using the log-rank test. Late recurrence of AF/AT was analysed starting from the last procedure in the cluster (B) because recurrence of AF/AT after the final procedure (C) does not take into account late recurrence occurring before successful repeated procedures.
Symptom severity assessed using the CCS-SAF scale is shown in figure 3. Overall, 95.1% of the patients reported improved symptoms compared with preablation.
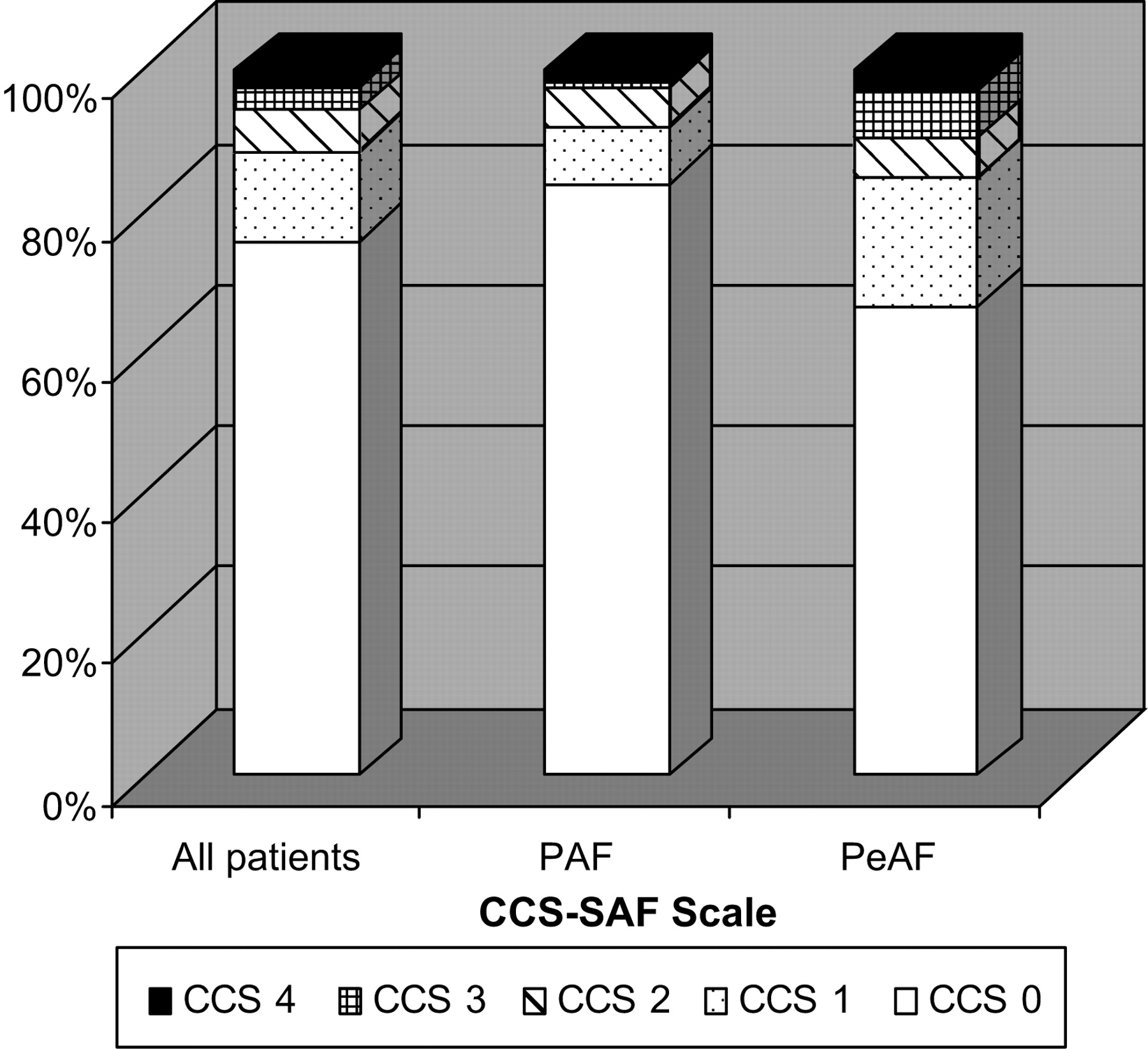
Symptomatic benefit after CA of AF. This bar chart shows the symptomatology of the patients at follow-up. The symptoms were assessed using the Canadian Cardiovascular Society Severity of AF scale. On this validated scale, patient symptoms and limitation are scored from 0 (asymptomatic) to 4 (disabling symptoms).
At final follow-up, 24.4% of the cohort remained on antiarrhythmic drugs: 1.1% on amiodarone, 3.8% on digoxin, 5.7% on class 1 agents, 5.0% on sotalol, 11.0% on other β-blockers and 9.9% on rate-controlling calcium channel blockers.
Late recurrence
The Kaplan–Meier analysis showed that most recurrences occur within 1–2 years (figure 2). Actuarial analysis of the rate of recurrence per 100 patient-years of follow-up showed recurrence beyond 3 years in only 3% per year (table 3).
Actuarial analysis of recurrence of AF/AT after the first cluster of ablation procedures for AF
Multivariate analysis
Patient factors predicting success after the final procedure are shown in figure 1. Independent predictors of recurrence were PeAF (p<0.01), female sex (p<0.05) and structural heart disease (p<0.001), with a non-significant trend towards an effect of time spent in AF (p=0.148). No procedural factors analysed impacted significantly on first-procedure success (figure 1). Analysing PeAF cases alone, there was a trend towards improved first-procedure success with the use of image integration (p=0.059; figure 1C). There was no independent effect of a later time of inclusion in the cohort.
Impact of CFE ablation on outcome
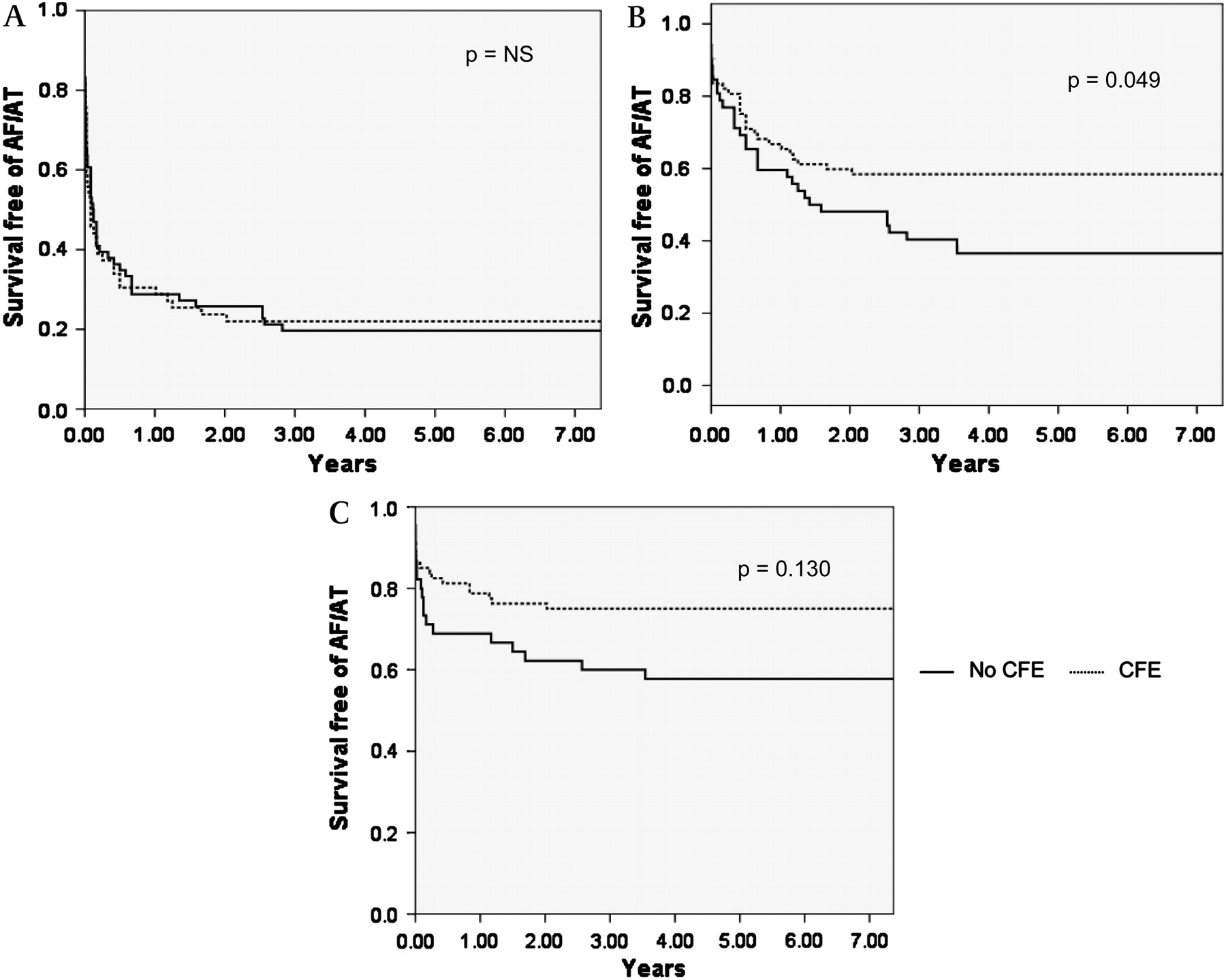
AF-free survival was assessed according to whether patients had CFEs targeted during their first procedure (49% of cohort, figure 4A), whether they had CFEs targeted in at least one procedure in their first cluster (59% of cohort, figure 4B) and whether CFEs were targeted at least once in any of their procedures (65% of cohort, figure 4C). Since CFE were targeted only from 2005 onwards, those who did not have CFE targeted were followed-up longer. To avoid temporal bias, the log-rank test was calculated for follow-up truncated at 3 years. Although there was no effect of CFE ablation on single-procedure outcome, there was a 21.6% absolute increase in success after the first cluster of procedures (p=0.049). This translated to a non-significant trend towards improved final outcome with CFE ablation (13.4% absolute difference; p=0.130). There was also a non-significant trend towards reduced late recurrence with CFE ablation (p=0.086 for recurrences between 2 and 3 years; table 3). There was no difference in the procedure time or the number of procedures (in the first cluster or in total). CFE ablation did not affect the proportion of recurrences after the first procedure due to left atrial tachycardia (22.0% in those who had CFE targeted versus 17.5% in those who did not; not significant).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Impact of additional CFE ablation on outcome after PeAF. The Kaplan–Meier curves showing AF-free survival (A) after the first procedure, (B) after the first cluster of procedures (ie, when AF is first eliminated whether after one CA or several) and (C) after the final procedure. The cohort has been divided according to whether patients had CFE targeted during their first procedure (A), whether they had CFE targeted in at least one procedure in their first cluster (B) and whether CFE were targeted at least once in any of their procedures (C). Significance was assessed using the log-rank test. Because CFEs were targeted only from 2005 onwards, those who did not have CFEs targeted were followed-up longer. To avoid temporal bias, the log-rank test was calculated for follow-up truncated at 3 years.
Discussion
Main findings
Long-term freedom from AF is achievable in 86% of the patients with PAF and 68% with PeAF. Recurrence occurs mostly in the first year, with only 3% per year recurring after 3 years. Despite conflicting evidence previously, we have demonstrated incremental benefit in targeting CFE in PeAF. Stroke and other adverse sequelae were infrequent over long-term follow-up.
Efficacy of CA for AF
The final procedure success was comparable with other high turnover centres, typically in the region of 70%–90%.1–3 5 The low CCS-SAF scores suggest that those with recurrent AF may still have derived symptomatic benefit; indeed, 95% of the patients reported improved symptoms.
The single-procedure efficacy of CA for PeAF was disappointing but in keeping with other reports.2 19–21 A recent study reported excellent long-term single-procedure success. Their use of intracardiac echo to monitor tissue contact may have reduced PV reconnection.5 New technologies such as robotic navigation to improve catheter stability or catheters that allow monitoring of tissue contact may improve outcomes.
Multivariate analysis identified structural heart disease, PeAF and female sex as independent predictors of recurrent arrhythmia. The impact of sex has been noted previously and may relate to subtle differences in cardiac anatomy or possibly more non-PV triggers.5 Left atrial size was not an independent predictor of recurrence despite being identified previously, perhaps because there is a relationship between this and time spent in AF.5
Patterns of recurrence
Studies report flattening of the AF-free survival curve after 1–3 years.3 8–10 However, this effect may be artificial because of diminished numbers at longer follow-up and relisting patients with late recurrence, preventing counting them as failures. To circumvent these issues, we examined recurrence after the initial cluster of procedures, with late recurrences counted as failures. Most recurrences occurred by 1 year. The Kaplan–Meier curves flattened by 3 years, with only three recurrences per 100 years of follow-up subsequently (ie, 3% per year).
Impact of CFE ablation
There has been difficulty reproducing Nademanee's early success using CFE ablation alone.19 22 The incremental benefit of CFE ablation in addition to PV isolation has been demonstrated over the short term,2 23 24 though not consistently.20 25
The lack of benefit after a single procedure may reflect the fact that most early recurrence is associated with PV reconnection.26 Once AF was eliminated after the first cluster of procedures, CFE ablation resulted in a 21.6% absolute increase in the number, maintaining sinus rhythm long term. Hence, the decreased ability of the modified atrial substrate to initiate and sustain AF may not become apparent until PV triggers/drivers are removed.
Although the Kaplan–Meier analysis showed an early benefit of CFE ablation, there was also a trend towards reduced late recurrence. CFE ablation did not affect the proportion of recurrence because of AF and AT, suggesting that fears over increased propensity to macro–re-entry are unfounded. Repeated procedures for late recurrence may diminish the difference in outcomes observed, as there was only a trend towards improved final outcome (13.4% absolute difference). There may have been insufficient numbers to clearly demonstrate this more modest overall effect.
Safety of CA of AF
The 3.1% major complication rate is comparable with that reported by other high turnover centres (typically 2–3%) and consisted mostly of stroke/TIA and tamponade.1–3 10 19 21 27 Stroke/TIA was infrequent (0.6%) and all resolved. However, our aggressive anticoagulation policy may have resulted in a slightly higher tamponade rate of 1.7% (0.4%–1.3% in other large series), although all were drained without sequelae.4 5 28 Two thirds of tamponades were late, emphasising the need for vigilance postprocedure. The three PV stenoses occurred in the first 50 cases, and with more caution to avoid the PV ostia, there were none subsequently.
Over 3.3 years, the seven deaths were unrelated to CA or AF. The CHADS2 score for the cohort was 0.8, with an expected stroke rate of 2%–3% (1% if anticoagulated).17 The rate of 0.3% per year confirms the low stroke rate after CA of AF.1 3 5
Limitations
Aggressive screening has revealed that a proportion of apparently cured patients have episodes of asymptomatic AF.29 Although patients underwent ambulatory monitoring, it is recognised that further screening may uncover an increment in asymptomatic recurrent AF. However, the extent to which asymptomatic patients were screened for arrhythmia was comparable with that reported for many other registries and trials. 1 3 4 20 21 24 25
Over the 5 years of this cohort study, it is possible that factors other than CFE ablation have improved outcome in later patients. However, (1) the procedure has been consistent throughout other than the addition of CFE ablation, (2) multivariate analysis did not show a significant effect of any procedural factors and (3) inclusion of time as a covariate showed no benefit of later inclusion in the cohort. Nevertheless, we acknowledge that registry data can be flawed and further confirmation from randomised trials is needed.
Conclusions
CA of AF can achieve long-term sinus rhythm for the majority of patients. The addition of CFE ablation to PV isolation may improve outcome. As most recurrences occur within a year, trials reporting on efficacy in CA of AF should perhaps consider this a minimum for reporting results. Those considering cessation of anticoagulation in patients prone to stroke should be mindful of the small but significant late attrition of 3% per year.
References
Footnotes
Linked articles 194613.
Funding RJH is supported by a grant from the British Heart Foundation (PG/08/130). ID is supported by a grant from Boston Scientific.
Competing interests RJS is a member of the scientific advisory board for Biosense Webster. He is listed on the Speakers Bureau for Endocardial Solutions and has received payment for lectures sponsored by them. RJS, SS, MJE, MD, DA and GT have also received support for travel to international meetings from Guidant, Medtronic, St Jude Medical, Endocardial Solutions, and Biosense Webster.
Provenance and peer review Not commissioned; externally peer reviewed.