Article Text

Abstract
Background: Patients with hypertrophic cardiomyopathy (HCM) exhibit a difference in left ventricular outflow tract (LVOT) obstruction, independently of basal septal thickness (BST). Some patients with HCM have a steeper left ventricle to aortic root angle than controls.
Objective: To test the predictors of the LV-aortic root angle and the association between LV-aortic root angle and LVOT obstruction using three-dimensional imaging.
Patients: 153 consecutive patients with HCM (mean (SD) age 46 (14) years, 68% men) and 62 patients with hypertensive heart disease of the elderly (all >65 years of age, 73 (6) years, 34% men) who underwent whole-heart three-dimensional cardiac magnetic resonance (CMR) angiography (1.5 T) and Doppler echocardiography. Forty-two controls (age 43 (11) years, 38% men) who underwent contrast-enhanced multidetector computed tomography and were free of cardiovascular pathology were also studied.
Main outcomes: LV-aortic root angle, BST and maximal non-exercise LVOT gradient were measured in patients with HCM and in hypertensive-elderly patients. Additionally, LV-aortic root angle and BST were measured in controls.
Results: The mean (SD) LV-aortic root angle was significantly different (p<0.001) in the three groups: HCM (134 (10)°), hypertensive-elderly (128 (10)°), control (140 (7)°). There was an inverse correlation between age and LV-aortic root angle in the three groups (all p<0.001): HCM (r = −0.56), hypertensive-elderly (r = −0.35), control (r = −0.48). On univariate analysis, in the HCM group, LV-aortic root angle (β = −0.34, p<0.001), age (β = 0.23, p = 0.01) and end-systolic volume index (β = −0.20, p = 0.02), but not BST (β = 0.02, p = 0.8), were associated with LVOT gradient. On multivariate analysis, only LV-aortic root angle was associated with LVOT gradient.
Conclusions: Patients with HCM have a steeper LV-aortic root angle than controls. In patients with HCM, a steeper LV-aortic root angle predicts dynamic LVOT obstruction, independently of BST.
Statistics from Altmetric.com
Hypertrophic cardiomyopathy (HCM) is a complex disorder, with a broad phenotypic spectrum.1 2 3 4 5 The most common phenotypic presentation is characterised by basal septal hypertrophy and associated systolic anterior motion of the mitral valve associated with dynamic left ventricular outflow tract (LVOT) obstruction, which has been shown to be an independent predictor of progression to severe heart failure symptoms and death.6 The cause of LVOT obstruction has classically been attributed to septal hypertrophy and systolic anterior motion of the mitral valve leaflet. However, patients with HCM with similar degree of basal septal hypertrophy have different degrees of LVOT obstruction; and in some cases significant LVOT obstruction is seen with minimal septal hypertrophy.7 As a result, other mechanisms contributing to LVOT obstruction such as concomitant mitral valvular and subvalvular pathology8 9 10 11 12 13 14 15 have been extensively explored.
We have observed that LVOT and the aortic root are oriented at a steep (acute) angle to the left ventricle in many patients with HCM, as compared with normal subjects (figs 1 and 2). Similar observations of steep aortoseptal angles have been made in patients with aortic stenosis and subaortic stenosis.16 17 One study demonstrated that patients with aortic stenosis and a steep aortoseptal angle are more likely to have asymmetric septal hypertrophy.16 18 However, these older observations were made using two-dimensional echocardiography, which lacks adequate spatial resolution, results in image foreshortening and cannot visualise in a three-dimensional format. With the emergence of cardiac magnetic resonance (CMR), high-resolution assessment of cardiac morphology and left ventricular (LV) volumes can be performed in multiple user-defined axes.19 20 At our institution, we now routinely perform CMR, along with Doppler echocardiography in patients with suspected or documented HCM, as part of a comprehensive HCM evaluation. For a more comprehensive assessment of the left ventricle, LVOT and subvalvular and papillary muscle morphology, we have recently adapted the whole-heart coronary MR angiographic sequence which enables us to obtain free-breathing, non-contrast, three-dimensional volumetric images of the heart (figs 2B–D).21 22 23 The aims of this multimodality imaging study were (a) to assess if the LVOT and aortic root are positioned at a steeper (more acute) angle in patients with HCM than in non-HCM controls and (b) to determine if there is an association between the acuity of the LV-aortic root angle and the extent of dynamic LVOT obstruction in patients with HCM.

Schematic representation of the left ventricle-aortic root angle in controls and patients with hypertrophic cardiomyopathy.

(A) Multiplanar reformatted computed tomographic image of a normal subject demonstrating normal thickness of the basal septum with a left ventricle to aortic root angle of 141°. (B) Multiplanar reformatted three-dimensional, whole-heart MR image of a patient with hypertrophic cardiomyopathy (HCM) and a basal septum measuring 1.9 cm, LV-aortic root angle of 146° and maximal left ventricular outflow tract (LVOT) gradient of 23 mm Hg. (C) Multiplanar reformatted three-dimensional, whole-heart MR image of a patient with HCN and a basal septum measuring 2.3 cm, LV-aortic root angle of 121° and maximal LVOT gradient of 150 mm Hg. (D) Multiplanar reformatted three-dimensional, whole-heart MR image of a hypertensive-elderly patient with basal septum measuring 1.9 cm, LV-aortic root angle of 122° and maximal LVOT gradient of 85 mm Hg.
Methods
Group with HCM and hypertensive-elderly patients
Between October 2006 and March 2008, 255 consecutive patients, referred for an initial consultation to our institution with suspected HCM, underwent a comprehensive evaluation, which included a thorough clinical assessment, Doppler echocardiography and CMR (performed at baseline before surgery). These patients were entered into a registry. For this study, subjects with contraindications for CMR (including pacemakers, defibrillators, aneurysm clips and severe claustrophobia) were excluded. Also, we excluded 40 patients because their clinical and multimodality imaging evaluation at our institution was not consistent with HCM. HCM was defined by a hypertrophied and non-dilated left ventricle in the absence of another cardiac or systemic disease that could produce a similar magnitude of hypertrophy.1 2 3 While some of the patients had a history of hypertension, it was clinically thought to be not significant enough to cause the degree of LV hypertrophy. The final group with HCM evaluated in this study comprised 153 patients. Also, we separated 62 patients >65 years of age (who also underwent CMR) who were diagnosed with hypertensive heart disease of the elderly, along with dynamic LVOT obstruction. The diagnosis of hypertensive heart disease of the elderly was based upon a thorough clinical evaluation, history of longstanding hypertension and the presence of a characteristic sigmoid septum and ovoid LV cavity on echocardiography and CMR.24 25 Clinical, medication, echocardiographic, Holter monitor (performed at our institution) and surgical data were recorded from the electronic medical record (DHK and MYD). This registry is approved by local institutional review board with waiver of individual informed consent.
Doppler echocardiography
Transthoracic echocardiography was performed using commercially available HDI 5000 (Philips Medical Systems, NA, Bothell, Washington, USA) and Acuson Sequoia (Siemens Medical Solutions USA, Malvern, Pennsylvania, USA) machines. Resting LVOT peak velocity was measured by continuous-wave Doppler echocardiography, and resting LVOT pressure gradient was estimated by a simplified Bernoulli equation.26 Care was taken to avoid contamination of the LVOT waveform by the mitral regurgitation jet.6 In patients with resting LVOT gradients <30 mm Hg, provocative manoeuvres, including Valsalva and amyl nitrite, were also used to measure a provocable LVOT gradient. The maximal LVOT gradient was defined as the highest recorded LVOT gradient (resting or provocable) in a patient. In patients with resting peak LVOT gradient >100 mm Hg, provocative manoeuvres were not used. The presence of an intrinsic mitral leaflet (anterior mitral leaflet prolapse or redundancy) and subvalvular abnormalities (chordal or direct papillary muscle attachment to the base of the anterior mitral leaflet) was recorded on surface echocardiography, based upon visual assessment and a consensus clinical agreement between authors experienced in HCM and echocardiography (MYD, MT and HML). The degree of resting mitral regurgitation was assessed by colour Doppler and quantified by a flow convergence method, on a scale of 0–4+ (0, none; 1+, mild; 2+, moderate; 3+. moderately severe; 4+, severe).27 The average time between acquisition of echocardiographic and CMR images was ⩽1 day.
CMR acquisition and analysis
The CMR examinations were performed in supine position on 1.5 T MR Scanner (Avanto, 45 mT/m maximum gradient strength, 200 T/m/s maximum slew rate; Siemens Medical Solutions, Erlangen, Germany), using a phased-array coil and four-lead vector electrocardiographic gating. Initial scout images were obtained during free breathing in three orthogonal directions to help determine the positions of the heart and diaphragm. For comprehensive assessment of cardiac volumes and ventricular wall thickness, balanced steady state free precession (bSSFP) images were acquired in multiple short- and long-axis orientations: TE = 1.6 ms, TR = 3.3 ms, flip angle = 70° and slice thickness = 6 mm (long-axis images) or 8–10 mm (contiguous short-axis images from apex to base). For short-axis images, the spatial resolution was 1.5–2.1 mm (x direction) by 1.1–1.4 mm (y direction). In long-axis images, the spatial resolution was 1.5–2.1 mm (x direction) by 1.1–1.6 mm (y direction). For patients able to suspend their respiration, breath-hold duration was 10–15 s, depending on the heart rate; otherwise, images were acquired using three signal averages.
Subsequently, for a three-dimensional assessment of cardiac morphology, we obtained whole-heart MR angiography images. For these images, window timing was selected to coincide with the quiescent period of the right coronary artery using a non-breath-hold cine bSSFP acquisition (TR 29 ms, TE 2.6 ms, flip angle 60°, 192×156 matrix, 3 NSA, 11 lines/segment) performed in the horizontal long-axis orientation. The motion of the right coronary artery was visually assessed by scrolling through the transverse cine MR images, and the rest period of minimal displacement during diastole was defined as the optimal acquisition window and a subject-specific trigger delay time was determined accordingly. Subsequently, high-resolution images of the whole heart were acquired using an ECG-triggered, fat-saturated, T2-prepared, segmented three-dimensional SSFP technique. This sequence has been described elsewhere for application to coronary artery imaging.21 22 23
For the current application, axial images were acquired during free breathing using a crossed-pair navigator, perpendicular to the dome of the right hemi-diaphragm, using motion adaptive gating, a 7 mm acceptance window and a constant correction factor of 0.6. Imaging parameters were as follows: TR = 3.8 ms, TE = 1.9 ms, flip angle = 70°, acquired matrix = 175–216 (phase direction) by 256 (readout direction) points (no interpolation), Grappa factor of 2, 24 reference lines and sampling bandwidth = ±125 kHz. Typically, 60–70 slices were acquired at 1.5 mm thickness (interpolated) to cover the heart. The in-plane resolution was typically 1.3–1.6 mm. Images were acquired during a 150 ms data acquisition window in mid-to-late diastole. This modified whole-heart imaging sequence added ∼5–10 min to the entire acquisition. CMR assessment was blinded from all other analyses.
LV ejection fraction and volumes (end-systolic and end-diastolic) were measured in a standard fashion, using Argus software (Siemens Medical Solutions, Erlangen, Germany) and indexed to body surface area. Maximal end-diastolic basal interventricular septal thickness was recorded. Subsequently, the whole-heart MR images were loaded on a standard offline three-dimensional work station (Leonardo, Siemens Medical Solutions) for analysis of the LV-aortic root angle. This angle was measured in a multiplanar reformatted LVOT view as an angle between LV inflow and outflow. Specifically, the LV inflow line bisected the mitral valve and the LV apex in two views, while the LV outflow line was drawn through the long axis of the aortic root (figs 2B–D).
Control group
The control group comprised 42 consecutive people who underwent contrast-enhanced 64-multidetector computed tomography (MDCT) coronary angiography (with radiation dose modulation) for evaluation of clinically suspected coronary artery disease in 2006. These subjects were <65 years of age, without a documented history of hypertension (including no antihypertensive drug use), no documented valvular, myocardial or aortic diseases. Furthermore, there was no evidence of coronary atherosclerosis on MDCT analysis. Also, we only included subjects whose images were reconstructed during the diastolic (typically 75%) phase of the cardiac cycle. Patients with a diastolic basal septal thickness >1.2 cm were also excluded. A detailed description of the MDCT coronary angiography acquisition techniques from our institution has been described previously.28 Briefly, these were retrospectively gated spiral scans obtained after administration of 90 ml of iodinated contrast. Additionally, clinical, medication and MDCT data were recorded from the electronic medical record (DHK and MYD). These subjects are also part of an institutional review board approved registry with waiver of individual informed consent.
MDCT analysis
MDCT images were loaded on a standard offline three-dimensional work station (Leonardo, Siemens Medical Solutions, Erlangen, Germany) for analysis. The maximal end-diastolic basal interventricular septal thickness was recorded. Similar to CMR analysis, LV-aortic root angle was measured in a multiplanar reformatted LVOT view as the angle between LV inflow and outflow (figs 1 and 2A).
Statistical analysis
Baseline demographics, risk factors and clinical variables are descriptively summarised. Continuous variables are expressed as mean (SD). Interquartile range is also presented, where deemed necessary. If the continuous variable demonstrated significant deviation from normal distribution on a Kolmogorov–Smirnov test, variance was stabilised by appropriate transformations. Categorical data are presented as the percentage frequency. Differences between groups were compared with the Student t test and analysis of variance for continuous variables and the χ2 test for categorical variables. Inter- and intraobserver concordance of LV-aortic root angle measurement (DHK and MYD) was assessed in 14 patients with HCM using an intraclass correlation coefficient. The association between variables was performed using univariate and multivariate regression analysis. For univariate analysis, we selected the variables that had a potential pathophysiological basis to be associated with the dependent variables (ie, LV-aortic root angle (see table 4) and LVOT gradient (see table 5)). For multivariate analysis, variables with a p value <0.05 on univariate analysis were included. Data assembly and basic statistical comparisons were performed with JMP software version 6.0.2 (Cary, North Carolina, USA). Advanced statistical analysis was performed using SPSS, version 11 (Chicago, Illinois, USA). A p value <0.05 was considered significant.
Regression analysis testing the association between left ventricle-aortic root angle and various potential predictors in the group with hypertrophic cardiomyopathy
Regression analysis testing the association between maximal LVOT gradient and various potential predictors in the group with hypertrophic cardiomyopathy
Results
HCM versus other groups
Three groups were studied: control group (n = 42), group with HCM (n = 153), and hypertensive-elderly group (n = 62). Table 1 shows a comparison of the baseline characteristics of the three groups.
Baseline characteristics of the three groups
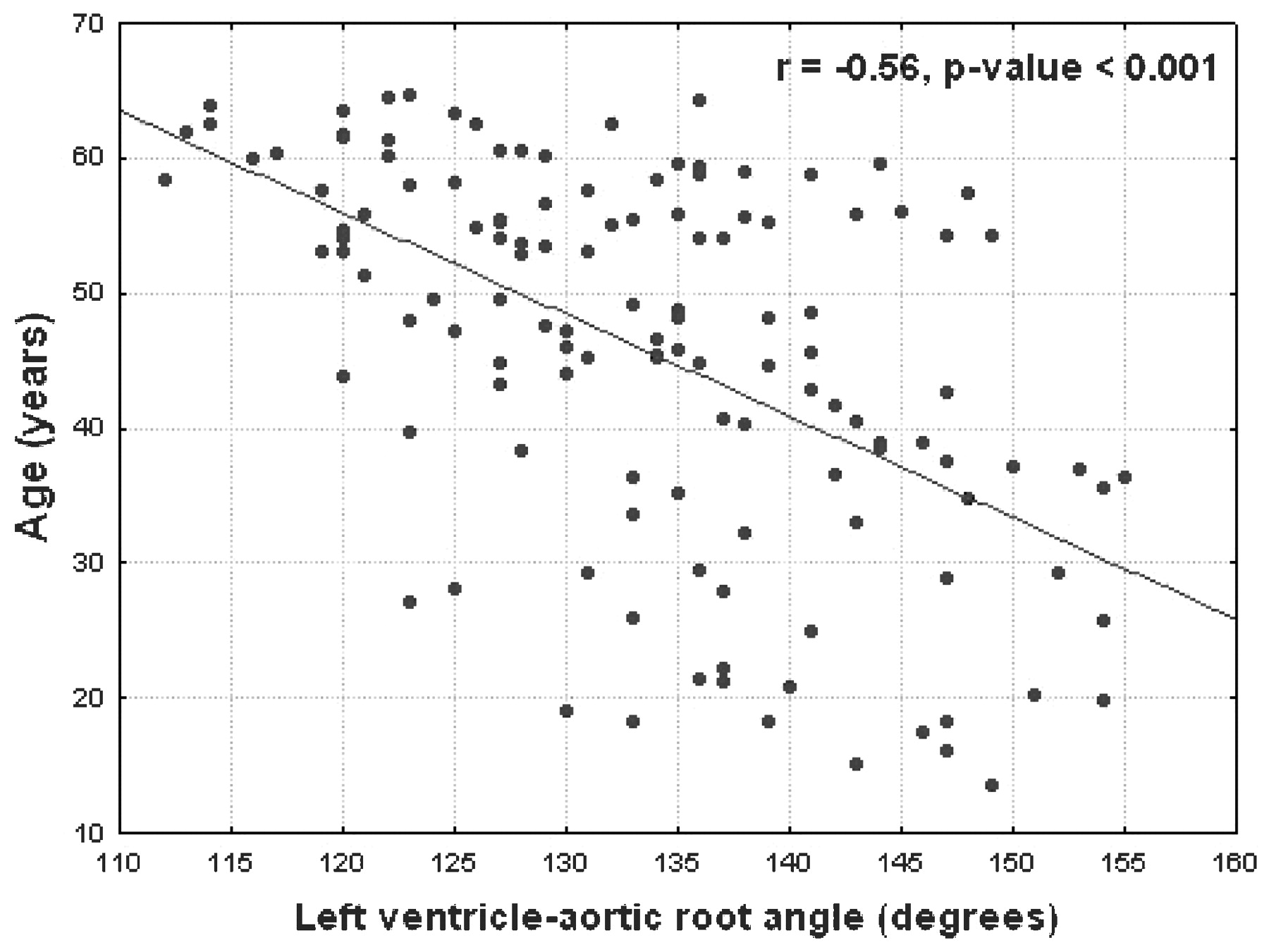
There was a significant difference in the LV-aortic root angle between the three groups. There was a moderately strong correlation between age and LV-aortic root angle for all three groups: HCM group (r = −0.56, p<0.001, fig 3), control group (r = −0.48, p<0.001) and hypertensive-elderly group (r = −0.35, p<0.001). The correlation between age and LV-aortic root angle in the two groups (HCM and hypertensive-elderly groups) merged together was also significant (r = −0.59, p<0.001). However, men and women had similar mean (SD) LV-aortic root angles in all three groups: HCM group (138 (5)° vs 141 (8)°, p = 0.2), control group (134 (10)° vs 136 (10)°, p = 0.2) and hypertensive-elderly group (126 (5)° vs 128 (6)°, p = 0.2). Of note, no patient had a dilated aorta or aortic root (>4 cm).

{kind=link}
{kind=link}
{kind=link}
Linear regression demonstrating association between age and LV-aortic root angle in the group with hypertrophic cardiomyopathy.
HCM group analysis
Table 2 shows the detailed baseline clinical characteristics of the groups with HCM.
Clinical characteristics of the group (n = 153) with hypertrophic cardiomyopathy
Seventy (46%) patients had significant symptoms with New York Heart Association class III (no patient was in class IV). There were 73% patients receiving β blockers and 29% receiving calcium channel blockers for symptomatic relief. Table 3 shows the characteristics of the group with HCM, separated on the basis of significant symptoms (New York Heart Association class >II).
Characteristics of the group with hypertrophic cardiomyopathy, separated on the basis of New York Heart Association (NYHA) class
Table 4 shows the results of the univariate and multivariate regression analysis, testing the association between LV-aortic root angle and various potential predictors.
Of all the potential factors influencing the LV-aortic root angle, only age and basal septal thickness (albeit, to a much smaller extent) maintained their significance on multivariate regression analysis. There was a significant increase in steepness of the LV-aortic angles for patients with HCM divided into quartiles, based on age (p<0.001): 142 (9)° (first quartile, ⩽36 years), 137 (9)° (second quartile, 37–47 years), 132 (9)° (third quartile, 48–56 years) and 127 (9)° (fourth quartile, >56, but <65 years). Furthermore, there was no difference in LV-aortic angles in patients with HCM divided according to the presence or absence of the following: syncope (134 (10)° vs 134 (10)°, p = 0.8), atrial fibrillation (132 (11)° vs 134 (10)°, p = 0.2) and Holter monitor documented ventricular tachycardia (135 (10)° vs 134 (11)°, p = 0.8).
The intraclass correlation coefficient for intraobserver (0.91) and interobserver (0.88) concordance of LV-aortic root angles in the group with HCM was very high (both p values <0.001).
Association of LVOT gradients and various predictive factors in the group with HCM
On Doppler echocardiography, the vast majority (80%) of patients had an elevated (>49 mm Hg) maximal resting (either provoked or unprovoked) LVOT gradient. There was a significant inverse correlation between LV-aortic root angle and maximal LVOT gradient (β = −0.34, p<0.001). Table 5 shows the results of the univariate and multivariate regression analysis testing the association between maximal LVOT gradient and various predictors.
Subsequently, we divided the patients with HCM into two subgroups, based upon the presence of a high maximal LVOT gradient (⩾50 mm Hg). Table 6 shows the differences in various clinical and imaging variables.
Characteristics of patients with hypertrophic cardiomyopathy separated on basis of LVOT gradient
Of the group with HCM, 69 (45%) patients with HCM have undergone myectomy for relief of symptomatic LVOT obstruction (72% of which were isolated myectomies and the rest were combined with an additional mitral valvular/subvalvular procedure). The average (SD) time between the CMR study and myectomy was 48 (64) days. Patients undergoing myectomy were older (48 (13) vs 43 (15) years, p = 0.02), had higher maximal LVOT gradients (111 (50) vs 58 (56) mm Hg, p<0.001) and had a steeper LV-aortic root angle (132 (9) vs 136 (11), p = 0.008), despite a similar degree of basal septal hypertrophy (2.1 (0.6) vs 1.9 (0.7), p = 0.1), as compared with those who did not undergo myectomy.
Discussion
Using three-dimensional non-invasive imaging with multiplanar post processing, we demonstrate that the LV-aortic root angle is significantly steeper (more acute) in patients with HCM and in hypertensive-elderly patients as compared with normal controls (figs 2A–D). The LV-aortic root angle had a significant inverse association with age (including in the control group), but only a weak association with maximal basal septal thickness. Furthermore, using multimodality imaging, we also demonstrate that in patients with HCM, there was a significant, inverse association between LV-aortic root angle and maximal LVOT gradient. This association was stronger then other factors, including age, degree of basal septal hypertrophy and end-systolic volume index. However, the correlation coefficients between LVOT gradient and the LV-aortic root angle were relatively weak, probably reflecting the fact that the LVOT gradient is affected by multiple factors. Patients with worse symptoms had a steeper LV-aortic root angle, despite a similar degree of basal septal hypertrophy. Finally, patients who underwent myectomy (after imaging evaluation), due to persistent symptoms despite maximal medical treatment, also had a steeper LV-aortic root angle and increased maximal LVOT gradient, as compared with those who did not, despite having a similar degree of basal septal hypertrophy.
The findings of this study further raise the question as to whether the acuity of the LV-aortic root angle is part of the broad morphological spectrum of HCM, which contributes to LVOT obstruction, or if the LVOT obstruction results in LV remodelling in such a way as to steepen this angle. From a clinical standpoint, there is a wide heterogeneity in the degree of septal hypertrophy and dynamic LVOT obstruction.7 While some of this heterogeneity might be a result of mitral valvular and subvalvular abnormalities,8 9 10 11 12 13 14 15 there seem to be additional factors that might be contributing. In this study, mitral valvular and subvalvular abnormalities were deemed to be contributing to LVOT obstruction only in a small proportion of cases (as demonstrated by a relatively high percentage of isolated myectomies). Conceivably, potential factors including the LV-aortic root angle add to the pathophysiology of dynamic LVOT obstruction.
We hypothesise that a steep LV-aortic root angle could potentially increase the turbulence of blood flowing from the left ventricle into the aorta, leading to remodelling of the LVOT owing to increased left intracavitary ventricular pressure. Indeed, fluid modelling studies testing the effect of variable flow angulation have demonstrated that the shear stress on the basal septal surface increases with a steeper aortoseptal angle; with altered fluid shear stress being linked to development of vascular obstruction in animal models.29 30 Such a concept has been supported by previous studies illustrating similar findings in other conditions which increase the intracavitary pressure (eg, subaortic membrane).16 17 31 32 33 34 However, this hypothesis does need to be validated in the context of HCM. This process appears to be strongly associated with age, and to a lesser extent with basal septal thickness. Therefore, an acute LV-aortic root angle, in the setting of basal septal hypertrophy, may be one of the potential mechanisms by which elderly patients with long-standing hypertension develop dynamic LVOT obstruction. Our study does suggest that LV outflow remodelling, as represented by a steeper LV-aortic root angle appears to manifest in an exaggerated fashion in HCM, albeit at a much earlier age. Also, several previous studies have demonstrated that the aortoseptal angle is more acute in patients with fixed LVOT obstruction, as seen in isolated subaortic stenosis and aortic stenosis.16 17 31 32 33 34
Compared with previous reports that have used “aortoseptal angle”,16 17 31 32 33 34 we chose the angle between LV “inflow” and “outflow” to avoid the potential confounding that would be generated by varying degrees of septal hypertrophy. In recent years, CMR has become the standard of care in our institution as part of a comprehensive multi-imaging modality assessment (which includes Doppler echocardiography) of patients who are being evaluated for HCM.8 35 36 In order to comprehensively assess volumetric LV morphology and be able to use multiplanar reformatting in patients with HCM, we have modified the recently described free-breathing, whole-heart coronary MR angiogram sequence21 22 23 to significantly reduce the time of acquisition to <5 min in almost all cases. To compare the LV-aortic root angle with that of age-matched controls, we selected consecutive subjects who had undergone MDCT (for evaluation for suspected coronary artery disease), as there were not enough “true normal subjects” who had undergone a CMR assessment (including whole-heart MR angiogram sequence). Measurement of the LV-aortic root angle in these patients was done using the exact methodology and the same workstations as those used for the CMR group. Hence, the likelihood of a difference in measurement because of different imaging modalities was small.
Limitations
Because this observational study was conducted at a tertiary referral centre, there is significant selection bias. The patients in our study were referred to our centre for a cardiac evaluation owing to the presence of significant symptoms or because they had a family member with known HCM. Patients with standard CMR contraindications were excluded, further adding to the selection bias. Approximately one-third of the patients with HCM had a concomitant diagnosis of hypertension. However, no patient with HCM had hypertension clinically deemed severe enough to account for dynamic LVOT obstruction. We separated patients aged >65 years to avoid confounding the results with patients who might potentially have hypertensive heart disease of the elderly (leading to LVOT obstruction).24 25 The dynamic nature of LVOT obstruction and its susceptibility to a multitude of factors, including heart rate, arrhythmia, body position and volume status, should be noted when assessing the strength of the correlation between LV-aortic root and LVOT obstruction. Furthermore, occasionally maximal gradients can be missed using Valsalva or amyl nitrite. Assessment of the LV-aortic root angle by CMR has not previously been studied and is not standardised. However, the assessment in this study was found to be highly reproducible, as it was performed by constructing a standard LVOT view using three-dimensional reconstructions in all subjects. A more comprehensive study which includes a large cohort of normal patients as well as a larger group of the more typical/ordinary patient with HCM would need to be conducted to establish the normal range for an LV-aortic root angle and the threshold above which there is a higher frequency of LVOT obstruction. Although the association between LV-aortic root angle and LVOT gradient is modest, this finding may demonstrate an additional morphological manifestation in the broad phenotypic expression of HCM.
Potential clinical implications
The observations from this study are predominantly hypothesis-generating and raise the following questions which would have to be answered using a prospective longitudinal study design: Does the LV-aortic root angle progress over time and correlate with progression of clinical symptoms? Is the angle part of the broad spectrum of different morphological expressions of HCM or is it a result of a particular genetic mutation? Is an acute angle associated with adverse outcomes? And can the acute angle be reversed by medical treatment and/or myectomy, and does this correlate with improvement in symptoms and long-term outcomes? At our institution, with the common utilisation of “more extensive myectomy” as well as papillary muscle reorientation surgery, use of three-dimensional CMR in preoperative planning (along with its utility in myocardial scar assessment) has become the standard of care.37 38 With the future emergence of robotic myectomy, this comprehensive assessment (including LV-aortic root angle measurements) might be of added clinical utility.
Conclusions
When compared with normal subjects, patients with HCM have a steeper LV-aortic root angle, as measured by three-dimensional imaging. In patients with HCM, LV-aortic root angle is associated with maximal LVOT gradient, independently of the degree of basal septal hypertrophy. Further prospective longitudinal studies are required to determine if acuity of the LV-aortic root angle is progressive and associated with adverse outcomes.
Acknowledgments
We thank Ms Joan Weaver, RT (MR) and Angel Lawrence, RT (MR) for acquisition of the CMR images.
REFERENCES
Footnotes
See Editorial, page 1725
Competing interests None declared.
Ethics approval Approved by the Cleveland Clinic IRB.
Provenance and Peer review Not commissioned; externally peer reviewed.