Article Text

Abstract
Objective We hypothesised that abnormal global longitudinal strain (GLS) would predict outcome in hypertrophic cardiomyopathy (HCM) better than current echocardiographic measures.
Methods Retrospective analysis of risk markers in relation to outcomes in 472 patients with HCM at a single tertiary institution (2006–2012). Exclusion criteria were left ventricular (LV) hypertrophy of other origin, patients in atrial fibrillation, lost to follow-up and insufficient image quality to perform strain analysis. Standardised echocardiogram recordings were reviewed and standard variables and LV GLS were measured. The primary end-point included all cardiac deaths, appropriate defibrillator shocks and heart failure (HF) admissions. The secondary end-point was death by HF and admissions related to HF.
Results Mean age was 50.0±15.0 years; 322 (68%) were men. At a median of 4.3 years (IQR 0.1–7.8) follow-up, 21 (4.4%) patients experienced cardiovascular death: 6 (1.3%) died from HF, 13 (2.7%) had sudden cardiac death and 2 (0.4%) died secondary to stroke. Four (0.8%) patients experienced appropriate defibrillator shock, and 13 (2.7%) were admitted for HF. On multivariate Fine–Gray proportional hazard analyses, GLS was significantly associated with the primary end-point (HR=0.90, 95% CI 0.83 to 0.98, p=0.018) independently of age, maximal provoked LV outflow-tract gradient and LV end-systolic volume. Moreover, GLS was particularly associated with the secondary end-point (HR=0.82, 95% CI 0.75 to 0.90, p<0.0001) independently of age, previous atrial fibrillation, New York Heart Association (NYHA) class III–IV, LV end-systolic volume, E/E′, and outflow-tract gradient. Survival curves confirmed that GLS was associated with HF events (GLS <15.6%, p=0.0035).
Conclusions In patients with HCM, reduced GLS is an independent factor associated with poor cardiac outcomes, and particularly HF outcomes.
Statistics from Altmetric.com
Introduction
Early outcome studies indicated that sudden cardiac death is a major part of the natural history of hypertrophic cardiomyopathy (HCM), and that fatal ventricular arrhythmia may occur at any age.1–3 Recognition that HCM is an important cause of sudden cardiac death, particularly in the young, coupled with improved diagnostic skills and treatments, appears to have altered the previous ‘natural history’; adverse outcomes are increasingly associated with heart failure (HF) related complications.4 Individuals with severe left ventricular (LV) systolic impairment are readily identified with conventional imaging evaluation. They, however, are in a minority of those who suffer disease-related complications.4 More sensitive earlier markers of impaired LV function may be clinically useful to identify those at risk of HF complications and fatal ventricular arrhythmia.
Late gadolinium enhancement on cardiovascular MRI5–7 and elevated N-terminal pro-brain natriuretic peptide level8 have been evaluated as early biomarkers of poor outcomes in HCM. Diagnostic two-dimensional echocardiography is performed in all patients with HCM. The evaluation of global longitudinal strain (GLS) is readily available in addition to classic measurements such as maximum wall thickness and LV outflow-tract obstruction. Percentage of LV longitudinal systolic deformation can be quantified by the speckle-tracking method in the three apical views in less than 1 min.9 The software is readily available among all vendors and the results can be used as routine in most echocardiography laboratories in more than 80% of the patients. In a preliminary study, impaired LV longitudinal myocardial strain was an early indicator of systolic dysfunction in patients with HCM and preserved LV ejection fraction.9 In other cardiomyopathies (eg, dilated cardiomyopathy, cardiac amyloidosis), GLS analysed by speckle-tracking echocardiography has proven to be a stronger predictor than LV ejection fraction of patient outcomes.10 ,11 A few small studies have evaluated GLS and outcomes in HCM,12–15 but the predictive value of GLS (used into small populations) has not been thoroughly assessed. We hypothesised that abnormal GLS would predict outcomes in HCM better than current echocardiographic measures. The current study was undertaken to evaluate reduced GLS as an early marker of disease-related outcomes in a large cohort of patients with HCM.
Methods
Study protocol
This was an observational, single-centre cohort study performed in the specialist inherited heart muscle disease unit at The Heart Hospital, London, UK. The HCM cohort was evaluated to identify patients seen between July 2006 and December 2012 who had undergone echocardiography with data storage in a format suitable for offline evaluation.
Inclusion criteria for the study were (1) a diagnosis of HCM based on LV hypertrophy on echocardiography (≥15 mm), that was unexplained by abnormal loading conditions, (2) age ≥16 years, (3) at least two visits to The Heart Hospital during the study period in which there were echocardiographic studies of adequate quality (at the first visit) to enable measurement of GLS.
The exclusion criteria were (1) other cardiac or systemic diseases that may produce LV hypertrophy, (2) long-standing uncontrolled hypertension, (3) persistent atrial fibrillation, (4) prosthetic valves and moderate-to-severe aortic stenosis defined by aortic valve area <1.5 cm2, (5) unsuitable echocardiograms for strain analysis (ie, low frame rate <45 ips or on a vendor other than General Electrics.
Data collection
Demographic characteristics including age at evaluation, family history of HCM, of unexplained sudden cardiac death (in a relative ≤40-year old or at any age if confirmed HCM), clinical symptoms, New York Heart Association (NYHA) functional class, current medication, heart rate and resting blood pressure were collected from the hospital records at the time of the echo assessment. Previous episode of atrial fibrillation, unexplained syncope ≤2 years, aborted sudden cardiac death, non-sustained (≥3 consecutive ventricular extrasystoles at a rate of ≥120 bpm and lasting <30 s) or sustained ventricular tachycardia on 24–48 h ambulatory electrocardiogram at or prior to evaluation,16 pacemaker or cardioverter defibrillator implantation, myectomy and septal alcohol ablation were also recorded.
The transthoracic echocardiography protocol was based on a standardised acquisition in all patients attending the clinic.17 Resting two-dimensional echocardiography was performed according to ASE guidelines,17 ,18 with either a Vivid 7 or E9 system (M3S probe, General Electric Medical System, Horten, Norway). Recordings in standardised views (three consecutive cardiac cycles) were acquired in two-dimensional, M-mode, pulsed Doppler, continuous Doppler, colour flow Doppler and pulsed tissue Doppler modalities, and stored for subsequent analysis. One independent and experienced observer (PR), blinded to the patient's history, analysed all the echocardiograms offline, applying standard measurements according to European Association of Echocardiography (EAE)/American Society of Echocardiography (ASE) guidelines17 ,18 and using the Echopac software version BT11.2 (General Electric Medical System, Horten, Norway). Maximum LV wall thickness was defined as the greatest thickness in any single segment. LV volumes and ejection fraction were calculated using biplane Simpson's rule.17 Biplane maximal left atrial volume was calculated using the area–length method and indexed to body surface area.19 LV filling pressures were estimated using Doppler mitral inflow and the ratio of peak E wave over E/E′ on tissue Doppler imaging at the lateral side of the mitral annulus. Mitral regurgitation was graded (none or trivial, mild, moderate or severe) according to current guidelines.20 Outflow gradients were measured and automatically calculated from the flow velocities using the modified Bernoulli equation.21 LV outflow-tract obstruction at rest was defined as a gradient ≥30 mm Hg.22 Maximal LV outflow-tract gradient during Valsalva provocation manoeuvre was also recorded. Peak systolic (transmural) longitudinal LV strain was quantified in the three apical views using the two-dimensional speckle-tracking method on a 17-segments model (figure 1).9 ,23 The frame rate of the recordings was between 45 and 75 ips. End systole was determined as aortic valve closure. GLS is usually expressed using negative numbers, as longitudinal shortening leads to a smaller segment length in systole compared with baseline, but, to avoid any confusion induced by the ‘minus’ sign and the cut-off values, we presented GLS in term of magnitude (absolute value) in all this manuscript.

Longitudinal strain evaluation by speckle-tracking echocardiography in the apical views: example of analysis in apical four-chamber view in a patient with hypertrophic cardiomyopathy (A) and global bull eye representation (B).
Imaging and record quality to perform strain analysis was considered correct and accurate: (1) when visualisation of the wall speckles was present transmurally (from endocardium to epicardium) during the whole cardiac cycle in at least 15/17 segments (inaccurate segments were excluded from the analysis), (2) if strain curves were of good quality (ie, not square), (3) where there was in front of good visual wall tracking quality of the region of interest.
End-points
The duration of follow-up was determined using the initial visit to the last visit and/or communication with the patient or event. Implantable cardioverter defibrillators were evaluated at The Heart Hospital pacing clinic every 6 months, as recommended. The primary end-point included: (1) cardiovascular death (sudden cardiac death, death related to HF, death secondary to stroke); (2) appropriate implantable cardioverter defibrillator shock; (3) HF admission. The secondary end-point included death related to HF and admissions related to HF.
Sudden cardiac death was defined as witnessed sudden and unexpected collapse or nocturnal death with no previous deterioration. Aborted sudden cardiac death or appropriate cardioverter defibrillator shock were also considered as events.
Statistical analysis
Descriptive data were analysed for normality using visual histograms and the Shapiro–Wilks test. Continuous variable were expressed as mean±SD or median (IQR), and categorical variables as frequencies and percentages. Linear correlations were evaluated between GLS and some relevant echocardiographic variables using Pearson test. Specific survival as defined for primary and secondary end-points, measured from inclusion until the first end-point occurring or last follow-up, was estimated using Kaplan–Meier method, and survival curves were compared using log-rank test. We used Fine–Gray proportional hazard regression analyses to integrate the competing risk of other causes of death for univariate and multivariate analyses for each end-point.24 The significant level α=0.25 in the univariate analysis was used to select variables for the multivariate models. According to its weight, age was forced into the multivariate models. Estimated HRs and their 95% CIs were calculated.
For the primary end-point, multivariate models were performed using backward stepwise elimination in separate blocks (clinical variables and echocardiographic variables). For the secondary end-point, given the relatively low number of events, sequential multivariate analyses tested the variables with GLS in separate models by blocks (clinical variables, echocardiographic variables).
A p value <0.05 was considered as statistically significant. Our methods comply with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement.25 All statistical analyses were performed using the Stata software V.11.0 (StataCorp LP, College Station, Texas, USA).
Ethics
Our study complies with the Declaration of Helsinki. The National Research Ethics Service (NRES)/Ethics Committee London Harrow approval for data collection at The Heart Hospital was obtained which included waiving patients’ consent given the retrospective observational nature of the work.
Results
Study population
Four hundred and seventy-two out of a cohort of 714 patients with HCM fulfilled the study inclusion criteria. The clinical reasons for exclusion were: 71 for having no second visit during the study period (lost to follow-up), 59 for permanent atrial fibrillation, 3 for prosthetic valve and 2 patients for known severe untreated coronary artery disease. Technical echocardiographic reasons for exclusions were: 36 for poor acoustic window, and 71 for GLS analysis not feasible from the recordings (figure 2). The mean age at initial evaluation was 50.0±15.0 years, and 322 (68%) were men. Demographic, clinical and echocardiographic characteristics of the population (n=472) at the time of the first available echocardiographic strain analysis are presented in table 1. Sixty-four patients had implantable cardioverter defibrillator implantation prior to inclusion: 3 for secondary prevention and 61 for primary prevention. All the patients included had suitable frame rate and image quality for GLS measurement. GLS values were normally distributed.
Baseline clinical, demographic and main echocardiographic characteristics of patients

Flow chart. Study selection process: over 714 patients HCM reviewed with echocardiography from July 2006 to December 2012, 71 did not have available follow-up data, 64 were excluded for permanent AF or associated disease which could modify strain analysis interpretation and 107 were excluded for echo technical reasons. AF, atrial fibrillation; GLS, global longitudinal strain; HCM, hypertrophic cardiomyopathy.
Study end-points
Patients were followed for a median duration of 4.3 years (IQR 0.1–7.8 years). Twenty-one (4.4%) patients experienced cardiovascular death: 6 (1.3%) patients died from HF, 13 (2.7%) patients had sudden cardiac death and 2 (0.4%) died of stroke related to HCM. Four (0.8%) patients had appropriate implantable cardioverter defibrillator shock, and 13 (2.7%) patients were admitted for HF. Eleven (2.3%) patients died of non-cardiac causes: cancer (n=7), sepsis (n=3) and haemorrhage (n=1).
There were no relevant correlations between GLS and left atrial volume index, between GLS and E/E′. There was a small correlation between GLS and maximal wall thickness (r=−0.36), and between GLS and LV ejection fraction (r=0.42).
Survival analysis
Univariate Fine–Gray proportional hazard regression analyses to predict the primary and the secondary end-points are displayed in table 2.
Univariate Fine–Gray proportional hazard analyses according to the primary and the secondary end-points, integrating the competing risk of other causes of death
After sequential multivariate analyses (table 3), GLS was significantly associated with the primary composite end-point (HR=0.90, 95% CI 0.83 to 0.98, p=0.018) adjusted to age, independently of maximal provoked LV outflow-tract gradient (HR=1.01, 95% CI 1.00 to 1.02, p=0.047) and LV end-systolic volume (HR=0.95, 95% CI 0.92 to 0.98, p=0.001). Concerning the secondary end-point (table 4), after sequential analyses, GLS was particularly associated with HF death or admission related to HF (HR=0.82, 95% CI 0.75 to 0.90, p<0.0001), adjusted to age, and independently of previous atrial fibrillation (HR=2.84, 95% CI 1.03 to 7.81, p=0.043), NYHA class III–IV (HR=4.84, 95% CI 1.67 to 14.00, p=0.004), LV end-systolic volume (HR=0.98, 95% CI 0.92 to 0.99, p=0.036), lateral E/E′ ratio and resting maximal LV outflow-tract gradient (HR=1.01, 95% CI 1.00 to 1.02, p=0.040).
Multivariate Fine–Gray proportional hazard analyses integrating competing risk (other causes of death) according to the primary end-point: final steps of sequential analyses per blocks
Multivariate Fine–Gray proportional hazard analyses integrating competing risk (other causes of death) according to occurrence of HF death or HF admission (secondary end-point): sequential analyses per blocks
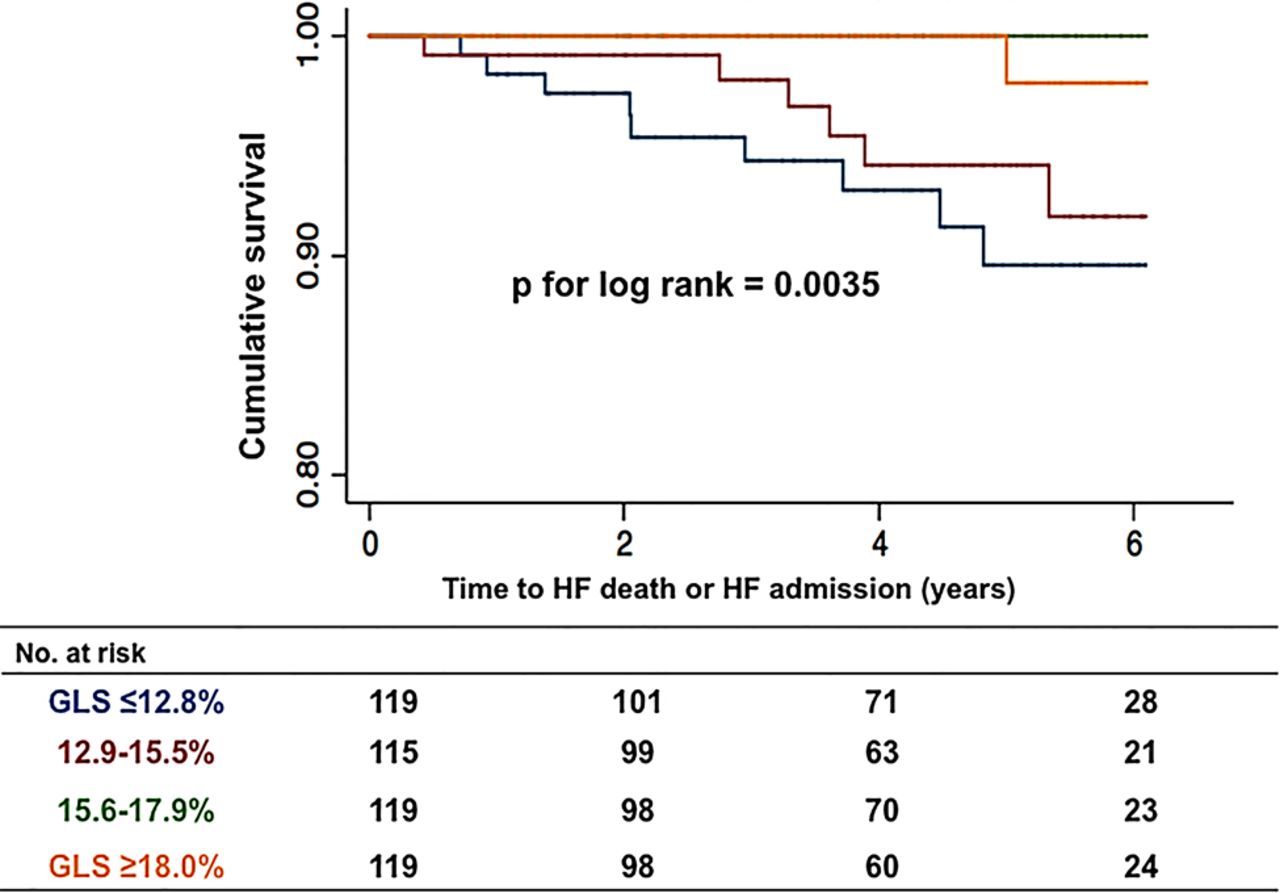
Survival rates evaluated by Kaplan–Meier lifetime analysis (also integrating the competing risk) were lower in patients of the two lower quartiles (GLS ≤12.8% and <15.6%, respectively) compared with patients with GLS ≥15.6% for HF events occurrence (p for log-rank=0.0035 (figure 3)).

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier event-free survival curves from heart failure (HF) death or HF admission (log-rank test) in patients with hypertrophic cardiomyopathy (n=472) according to left ventricular global longitudinal strain (GLS): analysis by quartiles.
None of the 14 patients with LV ejection fraction ≤50% had any death or other event during the study period. All six patients who presented with death related to HF had a GLS ≤14.0% and an LV ejection fraction >50%.
Discussion
This study contributes to the profile of patients with HCM at risk of major-disease-related cardiovascular events. This cohort study particularly highlights in a large HCM population the potential of reduced GLS as an additional independent predictor of severe cardiac outcomes and particularly of HF death or HF admission, regardless of LV ejection fraction.
Predictors of outcomes in HCM
Previous history of atrial fibrillation, NYHA III–IV, small LV end-systolic volume, resting or maximal provoked LV outflow-tract gradient and GLS were independent factors associated with occurrence of our primary and secondary end-points. These results are in keeping with previously published data in terms of NYHA III–IV, LV outflow-tract obstruction,3 ,4 LV end-systolic volume and GLS.15 Other echocardiographic parameters expected to be associated with HF events were less predictive of HF evolution than GLS (eg, left atrial dilatation, E/E′, LV ejection fraction and mitral regurgitation) as most of them (excepted LV ejection fraction) had p<0.25 on univariate analysis but were not significantly associated with the end-points on multivariate analysis. This could be partly explained by the population sample size.
However, this study, targeting a composite end-point, did not confirm other recognised predictors of sudden cardiac death such as family history of sudden cardiac death, severe LV hypertrophy or unexplained syncope.3 The recent guidelines of the European Society of Cardiology highlight the use of an algorithm to stratify patients according to their risk of sudden cardiac death.26 There is however no recommendation in terms of prevention of other cardiovascular events related to the condition, particularly HF. Moreover, more recent studies suggest that maximum wall thickness is not related to sudden cardiac death risk in a linear fashion3 and this may partly explain why it was not associated with our end-points. Progression towards thinning of the myocardium in late-stage HCM, with nevertheless preserved LV ejection fraction, may also explain our findings.27 Unlike LV ejection fraction, GLS seems to be of particular prognostic interest. However, it is all the time debated how to define the best cut-off value to use in practice. A cut-off of 14%,13 15%15 or 16%28 should be more sensitive than 10% but less specific. However, according to our Kaplan–Meier survival analyses, we think that patients with HCM with GLS below 15.6% have higher risk or cardiac events than patients with GLS ≥15.6%.
Data on the prognostic value of GLS are scarce. Our results are consistent with the few studies published to this date in the field, which have the limitations of small sample size and small number of cardiovascular events.12–15 ,28 One study showed that GLS ≤12.9% was a predictor of cardiac events and that it was correlated to the amount of late gadolinium enhancement on cardiac magnetic resonance.12 However, the cardiac events were few: one sudden cardiac death, three non-sustained ventricular tachycardia and the other events were HF hospitalisation or NYHA functional class worsening. Similarly, Reant et al15 found GLS with a cut-off of 15% to be predictive of such events, and Hartlage et al28 used a cut-off of 16%. Our feeling is that more GLS is altered (<16%), more we should considered the patient at risk of poor outcomes, particularly HF but equally ventricular arrhythmia. Another study by Debonnaire et al13 underscored the potential interest of GLS (using a cut-off value of 14%) as a predictive marker for appropriate implantable cardioverter defibrillator therapy in 21 out of 92 high-risk patients with HCM. In another study, reduced longitudinal septal strain and increased extent of interstitial fibrosis were predictors of ventricular arrhythmias.14 Patients with ventricular arrhythmias had lower septal longitudinal strain and increased extent of fibrosis in myectomy specimens, but no differences were demonstrated in terms of late gadolinium enhancement on magnetic resonance.14 The prognostic significance of late gadolinium enhancement remains controversial.5–7 GLS impairment in HCM is associated with greater myocardial fibrosis, contractility abnormalities and more severe hypertrophy.14 This could be the potential mechanisms by which GLS is related to severe ventricular arrhythmia, and HF but needs to be explored further.
In the meanwhile, GLS, available on routine echocardiography, may provide valuable prognostic information. However, determine a cut-off point is frequently debated and depends really of the target in term of sensitivity and specificity.
Clinical implications of our study
This study indicates that GLS, a readily available echocardiographic measurement, could help to predict major cardiovascular events in HCM, as previously demonstrated in various other cardiac diseases.29 Risk assessment and early intervention with implantable cardioverter defibrillators for primary prevention have been associated with reduced incidence of sudden cardiac death and may have altered the ‘natural history’ of the condition. HF is emerging as a serious complication and major determinant of outcome in HCM.4 As LV ejection fraction is generally preserved in patients with HCM, other markers of myocardial dysfunction are needed in clinical practice.9 Patients with low GLS should benefit from closer clinical management. Our results should foster further studies assessing the prognostic value of systematic GLS measurements in HCM.
Strengths and limitations
This is the largest study to this date that assesses GLS as a factor associated with outcomes in HCM. We identified a group of patients in whom evaluation of GLS was associated with major cardiovascular events. However, we acknowledge on a series of limitations. As a tertiary centre for inherited cardiomyopathy management, we cannot exclude referral bias. We did not collect mortality data from a national registry, but relied on our hospital's records and direct communication with the patients or their general practitioners. Patients with previous history of septal alcohol ablation and/or myectomy were not excluded. However, on univariate analysis, this condition was not significantly associated with poor outcome and they represent a relative minority of the HCM population. As atrial fibrillation is likely to be of prognostic significance in patients with HCM, exclusion of the patients in permanent atrial fibrillation, which is related to HF, may have influenced our results. Patients in permanent atrial fibrillation had to be excluded since GLS analysis is variable in this situation, and this might have induced a selection bias. In addition, we had to exclude patients without the possibility of strain analysis; consequently, our cohort was unfortunately reduced by 33%. Intraobserver and interobserver variability of GLS in patients with HCM in sinus rhythm is good (<10%), data were previously reported by Serri et al.9 With the version of the software we used for this study, the region of interest could not be set against segments asymmetrically thickened but the most recent one (BT11.3) can. Although GLS measurements have previously been described as concordant when compared with another vendor, the use of cut-off values has not been tested when using different vendors.30 Further studies are needed to address how GLS could tailor treatment. In the present study, we analysed only left atrial volume index as recommended by recent echocardiographic guidelines while there are actually more data to support the predictive value of left atrial diameter rather than volume in HCM.3 Late gadolinium enhancement on cardiac magnetic resonance was not evaluated in the present study. Maximal LV outflow-tract gradient was not routinely evaluated in the centre during or after exercise, and provocation by Valsalva manoeuvre is probably not the best way to do it.
Conclusions
GLS is associated with major cardiovascular events in HCM. This readily available marker of LV dysfunction may be considered to identify patients at risk or severe cardiac outcome, particularly of HF evolution.
Key messages
What is already known on this subject?
A few small studies have evaluated global longitudinal strain (GLS) and outcomes in hypertrophic cardiomyopathy (HCM), but the predictive value of GLS has not been thoroughly assessed.
What might this study add?
To date, this is the largest series in the field, and our findings suggest that GLS is an additional independent predictor of major cardiovascular events, particularly heart failure (HF) events in multivariate analysis (HR=0.82, 95% CI 0.75 to 0.90, p<0.0001), and in survival analyses (GLS<15.6%, p=0.0035).
How might this impact on clinical practice?
GLS should be used to identify patients with HCM at risk of poor cardiac outcomes, particularly HF evolution. Larger studies are needed to confirm this.
Acknowledgments
This work was undertaken at University College London Hospitals (UCLH)/University College London (UCL), which receives a proportion of funding from the Department of Health's National Institute for Health Research (NIHR) University College London Hospitals Biomedical Research Centre funding scheme. We are indebted to Charlotte Hall for her assistance.
References
Footnotes
Contributors PR, MM, JCM, SL, GL and WJM have participated in the design of the study. PR, MM, J-MLA, OG, SR, MT-E, CD, AP and SD have participated in data collection. PR, JP, GC and HB have participated in statistical analyses. All the authors listed in the title page have contributed to the manuscript redaction and improvement.
Funding PR and MM were supported for this work by the French Federation of Cardiology.
Competing interests None declared.
Ethics approval Local institutional approval.
Provenance and peer review Not commissioned; externally peer reviewed.