Article Text

Abstract
Introduction Many patients deemed inoperable for surgical aortic valve replacement (SAVR) have been treated successfully by transcatheter aortic-valve replacement (TAVR). This meta-analysis is designed to evaluate the performance of TAVR in comparison with SAVR.
Methods A systematic search was conducted using MEDLINE, PubMed, EMBASE, Current Contents Connect, the Cochrane library, Google Scholar, Science Direct and Web of Science. Original data were abstracted from each study and used to calculate a pooled OR and 95% CI.
Results Among three randomised controlled trials (RCTs), differences between the two cohorts were not statistically significant for the frequency of stroke (OR=1.94, 95% CI=0.813 to 4.633), incidence of myocardial infarction (MI), (OR=0.765, 95% CI=0.05 to 11.76) 30-day mortality rate, 1-year mortality rate (0.82, 95% CI=0.62 to 1.09) and acute kidney injury incidence rate. The non-RCTs demonstrated that the TAVR group had an amplified frequency aortic regurgitation at discharge (OR=5.465, 95% CI=3.441 to 8.680). While differences between the two cohorts were not statistically significant for the incidence of MI (OR=0.697, 95% CI=0.22 to 2.21), stroke (OR=0.575, 95% CI=0.263 to 1.259), acute renal failure requiring haemodialysis (OR=0.943, 95% CI=0.276 to 3.222), 30-day mortality (OR=0.869, 95% CI=0.621 to 1.216) and the need for a pacemaker (OR=1.832, 95% CI=0.869 to 3.862), a lower incidence of patients needing transfusion (OR=0.349, 95% CI=0.121 to 1.005) and new-onset atrial fibrillation (OR=0.296, 95% CI=0.124 to 0.706) was seen in the TAVR group.
Conclusions Randomised and observational evidence adjusted on the baseline patient’s characteristics finds a similar risk for 30 days mortality, 1-year mortality, stroke, MI and acute kidney injury in TAVR and SAVR.
- VALVULAR DISEASE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
-
What is already known about this subject?
-
Severe symptomatic aortic stenosis carries a poor prognosis and aortic valve replacement is the mainstay of treatment.
-
What does this study add?
-
This study is a comprehensive review of the evidence published so far and concludes TAVR was noninferior to surgical therapy at 30 days and 1 year.
-
How might this impact on clinical practice?
-
In properly selected patients, TAVR offers substantial improvements in symptoms and life expectancy.
Introduction
Surgical aortic valve replacement (SAVR) is the gold standard for treating aortic valve stenosis in operable patients.1 Even though SAVR improves symptoms and survival,2–4 subgroups of patients are at increased risk for mortality and morbidity and it would be desirable for this cohort to undergo a less invasive procedure. Transcatheter AVR (TAVR) can be performed by the transfemoral (TF) or transapical route.5–7 Results of recent randomised prospective trials demonstrate both the future promise and current problems of the TAVR approach. The PARTNER Trial Investigators8–12 have shown that patients with aortic stenosis (AS) who are high risk developed complications with conventional surgery, SAVR and TAVR have similar mortality at 30 days and 1 year and lead to comparable improvements in symptoms. Transcatheter replacement could be a substitute for surgical replacement in the high-risk subgroup of patients with AS. The purpose of the study was to compare the efficacy and safety end points of TAVR with SAVR through a meta-analysis and review the evidence published so far.
Methods
Study protocol
We followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines where possible in performing our systematic review.13 We performed a systematic search through MEDLINE (from 1950), PubMed (from 1946), EMBASE (from 1949), Current Contents Connect (from 1998), the Cochrane library, Google scholar, Science Direct and Web of Science until May 2014. The search terms included “trans-catheter aortic valve implantation, percutaneous aortic valve implantation, percutaneous aortic valve replacement, transfemoral aortic valve implantation, transapical aortic valve implantation, transarterial aortic valve implantation, direct aortic valve implantation, transcatheter aortic-valve replacement (TAVR)”, safety end points (stroke, myocardial infarction, atrial fibrillation, major vascular complications, acute kidney injury, blood transfusion), aortic valve stenosis (AS) AND “surgical aortic valve replacement (SAVR)”, which were searched as text word and as exploded medical subject headings where possible. No language restrictions were used in either the search or study selection. The reference lists of relevant articles were also searched for appropriate studies. A search for unpublished literature was not performed. The search was conducted by two researchers (VN and JR).
Study selection
We included studies that met the following inclusion criteria:
-
Studies identifying the population of patients with AS.
-
Randomised and non-randomised trials comparing TAVR and SAVR.
-
Original data (or ORs) reporting on the number of patients who underwent TAVR/SAVR stratified by various patient characteristics/outcomes/safety end points (stroke, myocardial infarction (MI), atrial fibrillation (AF), major vascular complications, acute kidney injury, blood transfusion).
Quality of the studies
Two independent reviewers screened the studies for inclusion, extracted data and evaluated quality (VN and JR). Quality assessment of randomised controlled trials (RCTs) was performed by the two reviewers according to the Cochrane Handbook for Systematic Reviews of Interventions V.5.1.0 based on the following aspects: random sequence generation, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other sources of bias. Three bias levels including low risk, high risk and unclear were assigned to every study aspect. Studies with more ‘low-risk’ bias assignations were recognised as superior. For non-random controlled studies, a modification of the Newcastle-Ottawa Scale (NOS) was used as an assessment tool for selection, comparability and outcome assessment.14 Study quality was rated on a scale from 1 (very poor) to 9 (high). Disagreements were resolved by consensus. This has been summarised in online supplementary table S1 and table 1.
Quality assessment
Data extraction
The full texts of the studies were read and data extraction was conducted by two independent reviewers (VN and JR). We performed data extraction using a standardised data extraction form, collecting information on the publication year, study design, number of cases, total sample size, population type, country, continent, mean age and clinical data. The event rate and CIs were calculated.
Data synthesis and analysis
Among non-randomised trials, a subgroup analysis was performed for the statistically sound studies (propensity score matched studies, case matched studies and adjusted analysis) to attain robust results. In order to assess the performance of the transapical approach with SAVR, a subgroup analysis was also performed. A subgroup analysis for the TF group and other approaches for TAVR were not possible due to the lack of extractable information from the studies.
Statistical analysis
Pooled event rate and 95% CIs were calculated using a random effects model (DerSimonian and Laird).15 We tested heterogeneity with Cochran's Q statistic, with p<0.10 indicating heterogeneity, and quantified the degree of heterogeneity using the I2 statistic, which represents the percentage of the total variability across studies which is due to heterogeneity. I2 values of 25%, 50% and 75% corresponded to low, moderate and high degrees of heterogeneity, respectively.16 Publication bias was quantified using Egger's regression model,17 with the effect of bias assessed using the fail-safe number method. The fail-safe number was the number of studies that we would need to have missed for our observed result to be nullified to statistical non-significance at the p<0.05 level. Publication bias is generally regarded as a matter of concern if the fail-safe number is less than 5n+10, with n being the number of studies included in the meta-analysis.18 All analyses were performed with a Comprehensive Meta-analysis (V.2.0).
Results
The search strategy retrieved 447 studies (figure 1). The abstracts were reviewed and after applying the inclusion and exclusion criteria, articles were selected for full-text evaluation. Systematic review19 and meta-analyses20 ,21 were excluded. Of the articles selected, only 39 studies (13 130 patients) met the full criteria for analysis and are summarised in online supplementary table S1. Of these, we found 3 RCTs,9 ,22 ,23 10 propensity score matched studies,24–32 5 case matched studies33–37 and 2 studies that provided adjusted analysis.38 ,39 The years of publication ranged from 2002 to 2014.

Flow of included studies.
Randomised controlled trials
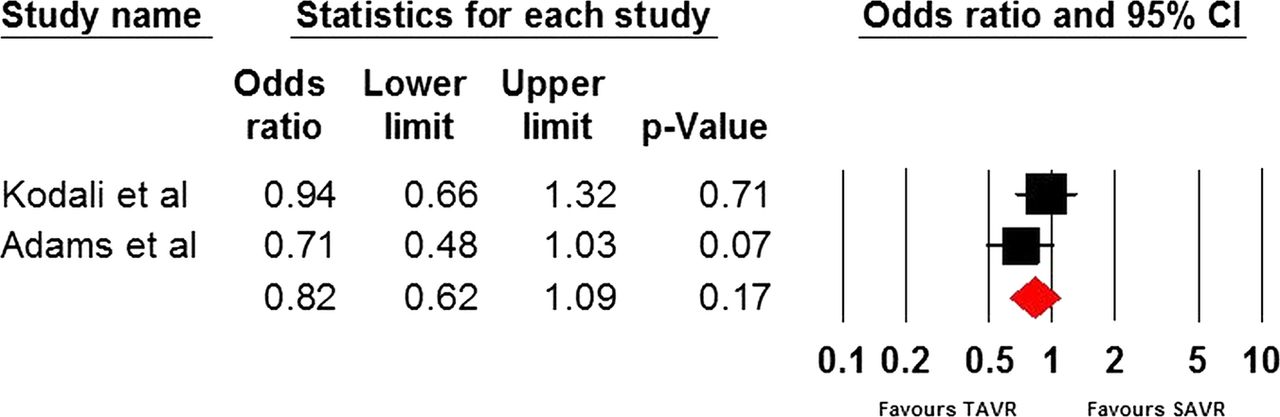
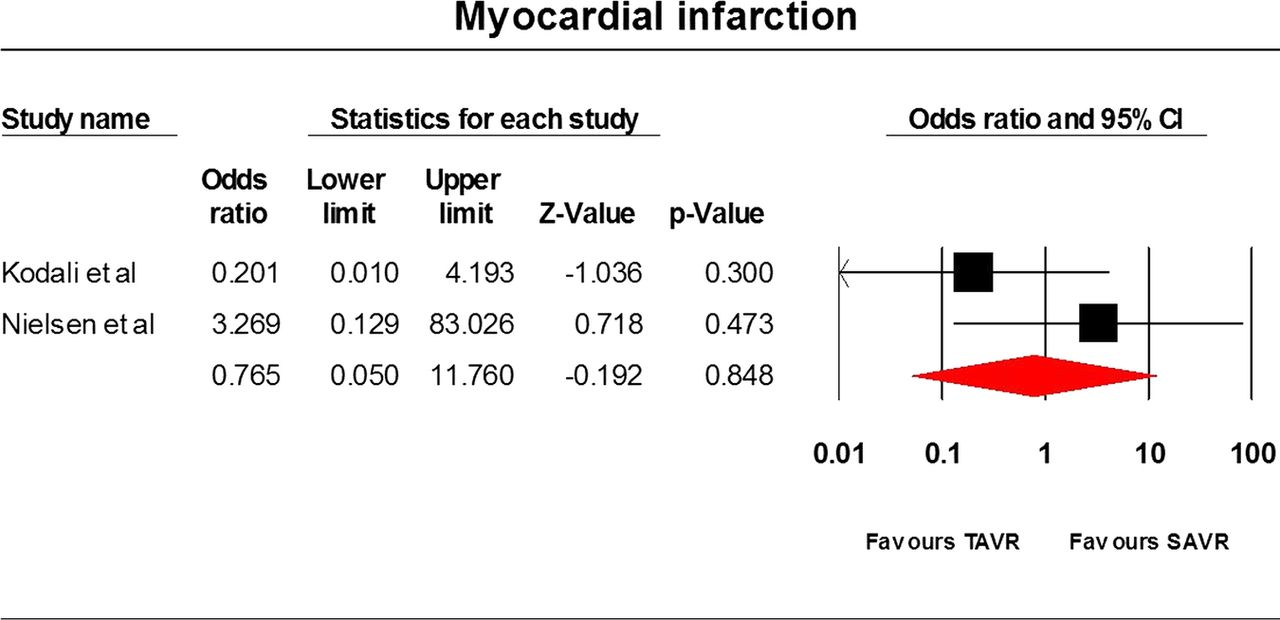
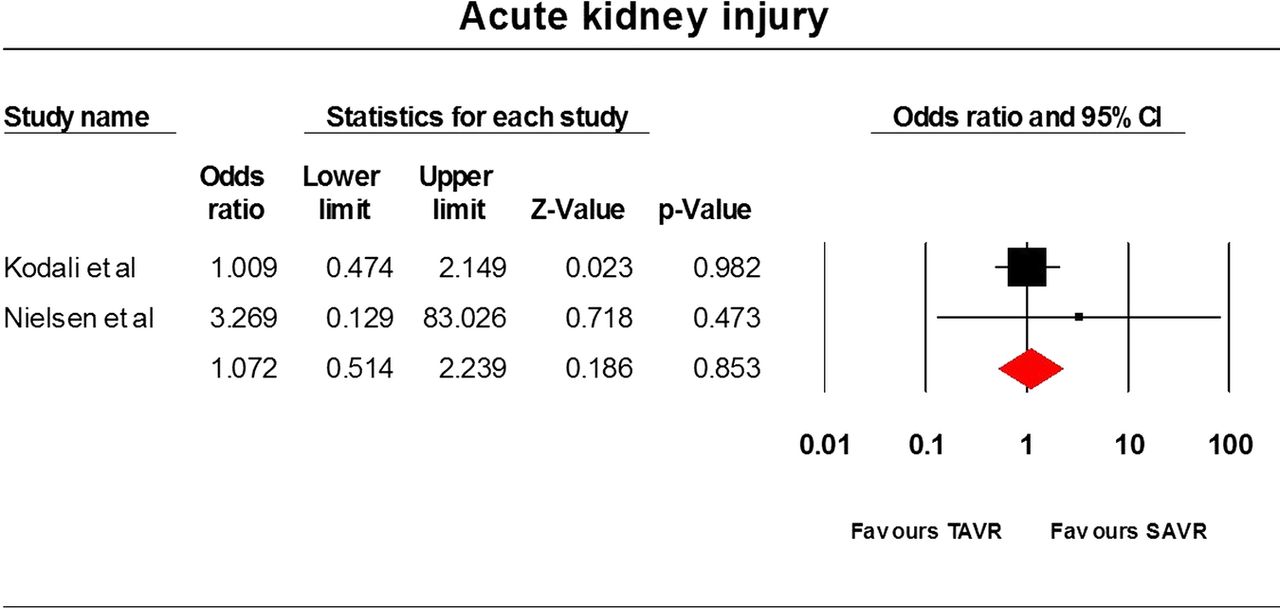
Only three RCTs9 ,22 ,23 have been conducted so far and they comprised 1564 patients. The STACCATO trial22 compared transapical TAVR with SAVR, whereas the PARTNER trial9 and Adams et al23 compared TF and transapical TAVR with SAVR. Data analysis was based on an intention-to-treat approach. Differences between the two cohorts were not statistically significant for the frequency of stroke (OR=1.94, 95% CI=0.813 to 4.633), incidence of MI (OR=0.765, 95% CI=0.05 to 11.76), 30 day mortality rate (OR=1.057, 95% CI=0.13 to 8.568), 1-year mortality rate (OR=0.82, 95% CI=0.62 to 1.09) and acute kidney injury (OR=1.072, 95% CI=0.514 to 2.239) incidence rate. The average overall hospitalisation time was 9.5(SD=0.99) and 12 days (SD=6.223) in the TAVR and SAVR cohorts, respectively (p value=0.6217). The results have been tabulated in table 2 and illustrated in figures 2⇓⇓⇓–6.
Overall OR and 95% CI for randomised controlled trials

Thirty-day mortality.

Stroke.
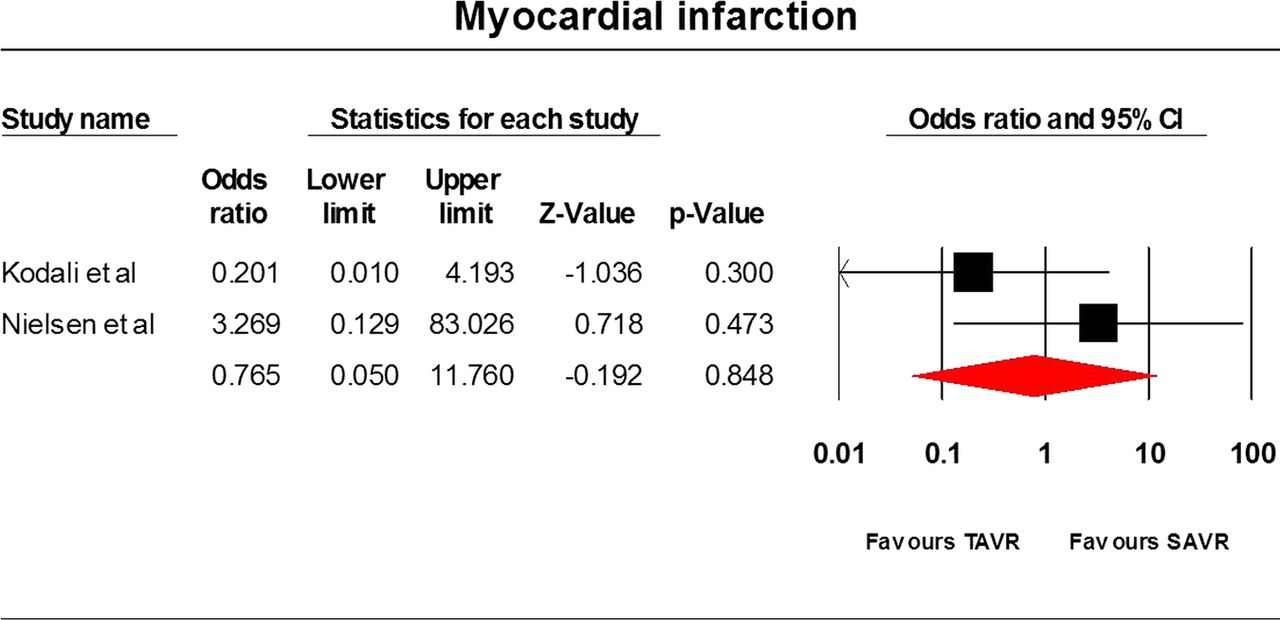
Myocardial infarction.

Acute kidney injury.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
One-year mortality.
Non-randomised controlled trials
Crude analysis
A total of 36 studies with 11 566 patients were included in the study. The TAVR group had an amplified frequency of pacemaker insertion (OR=3.169, 95% CI=2.338 to 4.294), a major vascular complication (OR=7.117, 95% CI=2.287 to 22.149) and aortic regurgitation at discharge (OR=7.412, 95% CI=3.695 to 14.868). While differences between the two cohorts were not statistically significant for the incidence of MI (OR=0.774, 95% CI=0.338 to 1.770) and 30-day mortality (OR=1.332, 95% CI=0.953 to 1.861), a lower incidence of new-onset AF (OR=0.353, 95% CI=0.148 to 0.842), patients needing transfusion (OR=0.392, 95% CI=0.189 to 0.812) and patients requiring haemodialysis (OR=0.863, 95% CI=0.361 to 2.063) was observed in the TAVR cohort. The average overall hospitalisation time was 10.33 and 12.21 days in the TAVR and SAVR cohorts, respectively (p value= 0.0473). The mean duration of stay in intensive care was 2.79 and 3.95 days (p value=0.0281) and the operative times were 150 and 215 min in the TAVR and SAVR groups, respectively (p value=0.0114). The results have been tabulated in online supplementary table S2.
Subgroup analysis of statistically sound studies
We performed a subgroup analysis for propensity score matched studies,24–32 case matched studies33–37 and studies that provided adjusted analysis.38 ,39 The TAVR group had an amplified frequency aortic regurgitation at discharge (OR=5.465, 95% CI=3.441 to 8.680). While differences between the two cohorts were not statistically significant for the incidence of MI (OR=0.697, 95% CI=0.22 to 2.21), stroke (OR=0.575, 95% CI=0.263 to 1.259), acute renal failure requiring haemodialysis (OR=0.943, 95% CI=0.276 to 3.222), 30-day mortality (OR=0.869, 95% CI=0.621 to 1.216) and the need for a pacemaker (OR=1.832, 95% CI=0.869 to 3.862), a lower incidence of patients needing transfusion (OR=0.349, 95% CI=0.121 to 1.005) and new-onset AF (OR=0.296, 95% CI=0.124 to 0.706) was seen in the TAVR group.
Among these studies, we also performed a subgroup analysis for three statistically sound transapical TAVR versus SAVR studies,27 ,29 ,40 which demonstrated that the differences between the two cohorts were not statistically significant for the incidence of stroke (OR=0.196, 95% CI=0.023 to 1.698) and 30-day mortality (OR=0.7, 95% CI=0.382 to 1.282). A subgroup analysis for the TF group and other approaches for TAVR were not possible due to the lack of extractable information from the studies.
Heterogeneity and publication bias
The heterogeneity of outcomes has been summarised in table 2 and online supplementary table S2. No publication bias was detected using Egger's regression model.
Discussion
In the past 10 years, TAVR has gained popularity in higher risk populations. Many patients deemed inoperable for AVR have been treated successfully by TAVR. According to our meta-analysis, both randomised and observational evidence adjusted on the baseline patient’s characteristics find a similar risk for 30-day mortality, stroke, MI and acute kidney injury (AKI) in TAVR and SAVR. TAVR is associated with a lower incidence of patients needing transfusion and new-onset AF.
Stroke
Stroke accounts for a major proportion of mortality post SAVR. This equates to approximately eight times the risk of mortality due to stroke compared to other reasons.41 According to the Society of Thoracic Surgeons (STS) database, the overall stroke rate is about 1.5%.3 ,42 After SAVR, stroke with an enduring disability was an imperative predictor of 30-day mortality in geriatric patients.43
Most of the participants in these studies were over 80 years and had numerous medical comorbidities accounting for increased risk. The average stroke incidence described in these publications was approximately 4%.44 However, the description of cerebrovascular complications associated with TAVR was inconsistent, which could possibly explain the heterogeneity among the studies. However, the incidence of a cerebrovascular event was more common after TAVR than SAVR in the PARTNER trial equating TAVR and SAVR in high-risk patients.45
In our meta-analysis, differences between the two cohorts were not statistically significant for the frequency of stroke (OR=1.94, 95% CI=0.813 to 4.633) in the TAVR and SAVR cohorts and no heterogeneity was observed among the two studies.
Need for a permanent pacemaker and post procedural atrial fibrillation
Owing to the proximity of the infranodal conduction system to the aortic valvular apparatus, patients with AS frequently present with atrioventricular conduction abnormalities (AVCA). In addition, the procedure itself may lead to temporary or permanent injury resulting in AVCA with the need for prolonged monitoring and/or a high rate of permanent pacemaker (PPM) implantation after TAVR.46–50 The rates of AVCA reported after SAVR are lower and a PPM is implanted in only 3–4% of patients undergoing SAVR.51–53 Cao et al54 found a 3.5-fold increased risk (13.2% vs 3.0%; p=0.0003) of pacemaker need in patients undergoing TAVR compared to SAVR. Our study presents similar findings;however, the significance was lost on performing a subgroup analysis for statistically sound studies, which was not done by Cao et al.54
Postprocedural AF is a predictor of long-term mortality in patients undergoing cardiac surgery.55 ,56 Earlier studies revealed a significant reduction of left atrial pressure in the first postoperative days after aortic valve replacement for aortic stenosis.57 ,58 TAVR allows one to avoid most of the factors causing AF after standard open AVR, such as the inflammatory effect of cardiopulmonary bypass and cardioplegic arrest, part of the postoperative increase of adrenergic tone and pericarditis.59 The fact that patients with TAVR experience less periprocedural AF than those receiving AVR is not unexpected. Motloch et al60 reported that the prevalence of post procedural AF was significantly lower in the TAVR group (6.0%, vs 33.7% after SAVR, p<0.05). A lower incidence of new-onset AF was observed in the TAVR cohort (OR=0.353, 95% CI=0.148 to 0.842) in our analysis, which is consistent with the aforementioned hypothesis.
Acute renal failure and aortic regurgitation
AKI after cardiac surgery is an autonomous predictor of mortality.61–64 Contrast to cholesterol embolisation, hypotension (rapid pacing, balloon valvuloplasty and valve deployment) are risk factors for acute renal failure. In our study, however, the incidence of AKI was similar in both clusters. Patients who underwent TAVR had a higher risk of developing moderate or severe aortic regurgitation, which is inversely related to survival.9
Limitations
Causes for heterogeneity
Heterogeneity was identified in many of the perioperative results. The classifications of ‘high surgical risk’ and the risk score models utilised varied between publications. The patient selection criteria for TAVR was diverse between institutes and had mean pressure gradient ≥40 mm Hg,36 ,38 logistic Euroscore >20%25 ,36 ,65 or >15%,38 age >7522 ,25 ,40 ,65 ,66 or >80,38 aortic valve area of <1.038 ,67 ,68 or <0.8 cm2,9 ,45 ,69 additive Euroscore ≥9,27 ,40 or STS score >15%66 or >10%.9 ,45 In a few studies, participants who were thought to be ‘too high risk’ were not offered TAVR, which comprised individuals with EF <20%9 ,45 or <15%.66 Similarly, crossover treatment was not reported consistently.
In a few studies, there was a considerable loss to follow-up,26 exclusion of patients with failed TAVR 39 and enclosure of participants who had surgical AVR with coronary artery bypass graft or mitral valve surgery.66 The follow-up period was short with only three studies providing detailed outcome data beyond 12 months.9 ,23 ,38 The evaluation of effectiveness of TAVR versus AVR in the long term remains unknown and delayed complications have not yet been estimated.
Upcoming clinical trials
The Nordic Aortic Valve Intervention (NOTION) trial,70 PARTNER II trial, MEDTRONIC COREVALVE U.S. PIVOTAL trial, COREVALVE vs SAVR-DENMARK TRIAL and SURTAVI trial are underway or are expected to start aiming to investigate the effectiveness of TAVR in younger and lower risk patients.
Conclusion
TAVR is maturing as a minimally invasive approach for treating patients with severe AS. It is quite agreeable that TAVR today is already preferable in a growing proportion of elderly and fragile patients; however, this procedure has the potential for serious complications. New technology will probably make it worthwhile in a larger proportion of clinical situations. The current evidence and results from this meta-analysis has demonstrated its feasibility and efficacy and drawn the attention of industry and physicians. Although short-term efficacy is good, there is little evidence on long-term outcomes. Randomised and observational evidence adjusted on the baseline patient’s characteristics finds a similar risk for 30-day mortality, stroke, MI and acute renal injury in TAVR and SAVR. We know that AVR treats the disease quite consistently and is still considered the standard treatment for most patients. The future is expected to be more prosperous as new developments and data from ongoing trials will provide the background to expand TAVR applications and establish their position in a broader spectrum of patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.