Article Text

Abstract
Background Due to improved care, the numbers of patients with tetralogy of Fallot (ToF) are increasing. However, long-term morbidity and need for reinterventions are concerns and also address issues of quality of life (QoL).
Methods Patients with ToF and valid EuroQol-5 dimensions questionnaire (EQ-5D) were identified in the national Swedish register on congenital heart disease. EQ-5Dindex was calculated and dichotomised into best possible health-related QoL (EQ-5Dindex=1) or differed from 1.
Results 288 patients met the criteria and were analysed. Univariate logistic regression showed a positive association between New York Heart Association (NYHA) class I (OR 8.32, 95% CI 3.80 to 18.21), physical activity >3 h/week (OR 3.34, 95% CI 1.67 to 6.66) and a better right ventricular function (OR 2.56, 95% CI 1.09 to 6.02). A negative association between symptoms (OR 0.23, 95% CI 0.13 to 0.42), cardiovascular medication (OR 0.31, 95% CI 0.18 to 0.53), age (OR 0.97, 95% CI 0.96 to 0.99) and EQ-5Dindex was observed. In multivariate logistic regression, NYHA I (OR 7.28, 95% CI 3.29 to 16.12) and physical activity >3 h/week (OR 2.27, 95% CI 1.07 to 4.84) remained associated with best possible health-related QoL. Replacing NYHA with symptoms in the model yielded similar results.
Conclusion In this registry study, self-reported physical activity, staff-reported NYHA class and absence of symptoms were strongly associated with best possible health-related QoL measured by EQ-5D. Physical activity level is a potential target for intervention to improve QoL in this population but randomised trials are needed to test such a hypothesis.
- tetralogy of fallot
- quality of life
- congenital heart disease
- register
- physical activity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Patients with congenital heart disease have been reported to have a good quality of life, but there are inconsistent findings regarding the impact of disease severity on quality of life.
Studies focusing on tetralogy of Fallot are scarce and has been performed at highly specialised centres.
What does this study add?
Self-reported physical activity was associated with best possible health-related quality of life, an association never reported before.
Medical factors such as New York Heart Association (NYHA) functional class, symptoms and cardiovascular medication were associated with health-related quality of life, and this applies even in a setting of national multicentre-derived patients.
How might this impact on clinical practice?
The result stresses the importance of evaluating physical activity, NYHA functional class, symptoms and medication thoroughly during regular follow-up.
Encouraging patients to a more active lifestyle may have a positive effect on health-related quality of life.
Introduction
Tetralogy of Fallot (ToF) is the most common cyanotic congenital heart defect.1 Due to continuous improvements in intervention techniques and care during childhood, the numbers of adults with ToF are increasing.2 Although reintervention rates in children with ToF are low and quality of life (QoL) is good or even better than healthy counterparts,3 4 living longer raises questions concerning long-term morbidity and mortality.5 It is well known that physical capacity in patients with ToF is impaired6 and long-term follow-up has shown that only a quarter of patients with corrected ToF are free from events after 40 years and nearly half need future reintervention.7 With this in mind, it becomes important to address QoL issues.
Many previous studies report that overall QoL in adults with congenital heart disease is good,8–10 but there are inconsistent findings especially regarding differences between diagnosis groups. Furthermore, such inconsistent findings are also valid regarding the impact of impaired physical capacity on QoL.11–14
Identifying factors associated with impaired QoL is important as this may lead to changes in routines for follow-up and counselling. Former studies have for example implicated that sense of coherence15 and level of physical activity are associated with QoL.16
Since former studies addressing QoL mainly have been performed at highly specialised tertiary centres, it is not evident that these results are applicable to a population with national multicentre-derived patients. Therefore, we conducted a cross-sectional registry study based on the Swedish national registry on congenital heart disease (SWEDCON).
In the present study, the aim was to identify factors associated with best possible self-reported health status measured by EuroQol 5-dimensions (EQ-5D) in adult patients with previously repaired ToF.
Materials and methods
SWEDCON register
The register was started in 1992 and since 1998 it has covered all seven healthcare regions in Sweden. Since 2009, the register also includes paediatric cardiology and congenital heart surgery. In the end of 2012, the registry contained almost 10 000 adults. Data are collected by each centre and contains information about diagnosis, interventions, demographics, medication, symptoms, New York Heart Association (NYHA) functional class, ECG, exercise tests, self-reported level of physical activity, echocardiography pacemaker/implantable cardioverter defibrillators and QoL assessed by EQ-5D.
Symptoms refer to cardiovascular symptoms (palpitations, syncope, dyspnoea, fatigue, oedema and chest pain). NYHA functional class is reported by the staff.
The register does not contain information about hospitalisations other than for surgical interventions.
Patient selection
This registry study obtained data from SWEDCON. Inclusion criteria were patients with ToF ≥18 years and valid EQ-5D questionnaire. All data available until 19 February 2013 were searched. The data from the last available clinical visit/test were used.
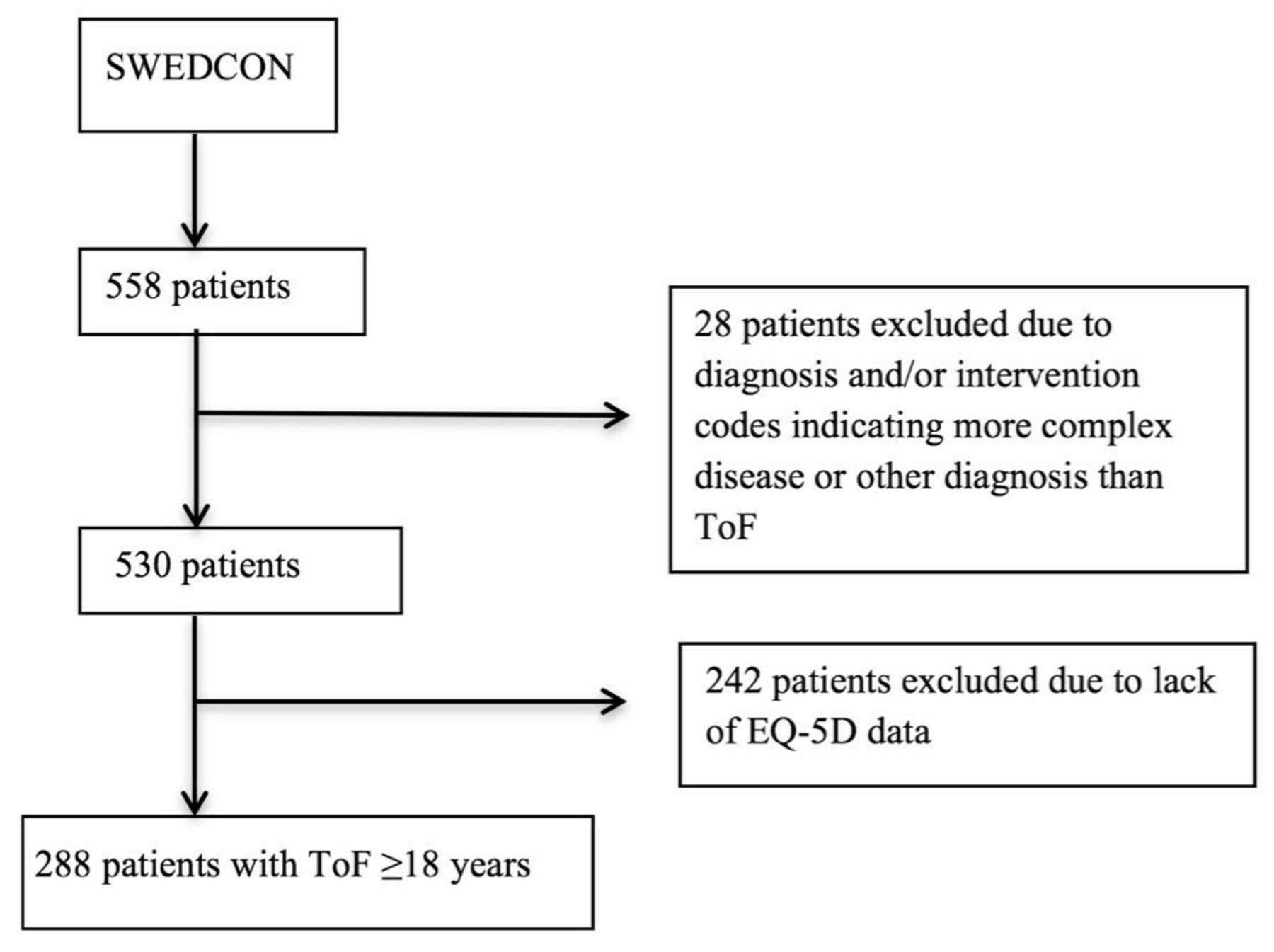
Data on patients with ToF were extracted and the file was manually validated case by case to verify that only patients with complete repair of ToF were included. Initially, 558 patients were identified. Based on intervention codes and concomitant diagnoses, 28 patients were excluded considered having more complex lesions or other diagnosis than ToF (figure 1).

{kind=link}
Overview of the inclusion of patients. ToF, tetralogy of Fallot.
In the remaining 530 patients, EQ-5D data were available in 288 who met the inclusion criteria and were included in the analysis.
The patients excluded due to lack of EQ-5D data did not differ regarding age, sex, body mass index (BMI), NYHA class, symptoms or level of physical activity (table 1).
Comparison between patients with and without available EQ-5D data
EQ-5D
The EQ-5D questionnaire was developed by the EuroQoL Group and enables the respondent to classify their health according to five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression.
Each dimension has three levels describing no problems, some problems or severe problems.
Thus, 243 different health states can be described. The information derived from the questionnaire can be converted in to a single summary index (EQ-5Dindex) by applying a formula weighting all levels in each dimension using an index tariff. Since there is no Swedish EQ-5Dindex value set, the British index was adopted as reference.17 EQ-5Dindex equal to 1 represents perfect health and 0 worst possible health status or even death.18 Using these calculations, it is possible to generate values below zero, often replaced by zero, but this does not apply in the present study since minimum score here was zero.
Self-reported level of physical activity
In the SWEDCON registry, self-reported level of physical activity is defined as sports/exercise performed more or less for its own sake. There are three levels: none, <3 h/week or >3 h/week.
Statistical analysis
The data were assessed for normality. Data are presented as ratios (percentage), means with SD and ORs with 95% CIs. For comparison between groups, χ2 test was used for categorical variables and independent samples t-test for continuous variables. The outcome variable EQ-5Dindex was dichotomised into EQ-5Dindex=1 or EQ-5Dindex<1.
Independent variables were assessed using logistic regression. The independent variables were reviewed and considered for associations. Univariate logistic regression was used to select variables for multivariate regression. Variables with a significant p value in univariate analysis were entered in multivariate analysis. In addition, smoking was entered in the model due to clinical relevance and borderline significance in univariate mode. The statistical analysis was performed using IBM SPSS statistics V.23.0. A p value <0.05 was considered significant.
Results
A total of 288 patients met the inclusion criteria and were analysed. The majority, 57%, of the patients reported their health status as the best possible (EQ-5D=1).
Patients experiencing best possible health-related QoL (HRQoL) (EQ-5D=1) were younger and reported a higher degree of physical activity than patients with worse self-reported health status (EQ-5D<1). Cardiovascular medication and symptoms were more common in the latter group, but there was no difference regarding sex, BMI or smoking frequency between the groups (table 2).
Patient characteristics
Univariate logistic regression analysis showed an association between best possible HRQoL (EQ-5Dindex=1) and NYHA I (OR 8.32, 95% CI 3.80 to 18.21), physical activity >3 h/week (OR 3.34, 95% CI 1.67 to 6.66), symptoms (OR 0.23, 95% CI 0.13 to 0.42), cardiovascular medication (OR 0.31, 95% CI 0.18 to 0.53) and age (OR 0.97, 95% CI 0.96 to 0.99). In addition, there was an association between preserved or slightly reduced right ventricular function, in contrast to ≥moderately impaired right ventricular function (OR 2.56, 95% CI 1.09 to 6.02) and best possible HRQoL but no association with left ventricular function (table 3). Since NYHA and symptoms were associated with each other, we constructed two models, one containing NYHA and the other symptoms.
Association between demographics, medical factors and health-related quality of life in univariate logistic regression
In the multivariate model including NYHA, physical activity >3 h/week (OR 2.27, 95% CI 1.07 to 4.84) and NYHA class I (OR 7.28, 95% CI 3.29 to 16.12) were associated with best possible HRQoL (table 4).
Association between demographics, medical factors and health-related quality of life in multivariate a logistic regression model containing NYHA instead of symptoms
When replacing NYHA with symptoms in the model, physical activity >3 h/week (OR 3.47, 95% CI 1.64 to 7.35) remained associated with best possible HRQoL, symptoms (OR 0.24, 95% CI 0.13 to 0.46) and cardiovascular medication (OR 0.55, 95% CI 0.30 to 0.99) (table 5) were negatively associated with best possible HRQoL, the latter borderline associated in the first model but with similar point estimates.
Association between demographics, medical factors and health-related quality of life. Multivariate logistic regression—model containing symptoms instead of NYHA
Discussion
Here, we report that HRQoL was associated with NYHA class, physical activity level, presence of symptoms and cardiovascular medication in a large, register-based population of patients with ToF. This stresses the importance to carefully assess these variables during periodic outpatient follow-up. Furthermore, this is the first time an association between a high physical activity level and best possible HRQoL is reported in adult patients with ToF.
Physical activity level was associated with HRQoL, which is in line with our previous report on adult patients with aortic valve disease.16 Associations between exercise test performance and general health has also been reported, and it may be that physical activity level is a marker of high HRQoL.19 Earlier studies20 21 have reported improvement in QoL after exercise intervention, and it is tempting to speculate that interventions targeting physical activity level would improve HRQoL in patients with ToF as well. Randomised clinical trials to test such a hypothesis are therefore warranted.
The NYHA class was strongly associated with HRQoL. In this study, we analysed staff-reported NYHA. Earlier findings suggest that there is a strong association between self-reported NYHA and HRQoL.8 22 This underscores the importance of correctly assessing this variable during follow-ups and that staff-reported NYHA here seems to be as valid as self-reported NYHA in that aspect.
Presence of symptoms were associated with HRQoL but not as strongly as NYHA. There are multiple reasons for this: first of all, many of the patients (60%) with worse self-reported health status (EQ-5D<1) were reported as asymptomatic. Whether this reflects the truth or is a consequence of deficient evaluation of symptoms during follow-up is not possible to tell.
Second, NYHA relates to limitations in physical activity whereas symptoms may occur unrelated to physical exercise.
Ongoing cardiovascular medication was associated with HRQoL in one of the multivariate models and borderline in the other, but with similar point estimates. Medication is probably an indicator of more severe disease but may also itself affect HRQoL through side effects, both physical and psychological. Furthermore, daily intake of drugs reminds the person of the chronic cardiac disease that not necessarily causes daily symptoms or experience of limitations.23 24
We found no association between age and HRQoL in the multivariate analysis. Since it is well known that morbidity increases with age in the ToF population,7 one could have expected an association. The lack of association in multivariate mode may be due to the strong associations between NYHA, physical activity and HRQoL outweighing the weaker variable age.
Study limitations
In registry studies, there are certain factors that can influence the results. Data are delivered from several sites and by many individuals, which potentially may reduce the validity of data. On the other hand, the large population likely compensates for such possible variations.25 Missing data pose a potential problem. In the current study, 242 patients were excluded due to missing data on EQ-5D. This is, however, most likely explained by changes in routines regarding registration of this variable. Comparison between the groups with and without available EQ-5D data did not show any differences with regard to demographics or medical factors. However, NYHA class and presence of symptoms was borderline significant with a slightly higher proportion of symptoms and a lower proportion of NYHA class I in those lacking EQ-5D data (table 1). Therefore, inclusion of the 242 patients without EQ-5D data would likely have strengthened the OR for these variables. We find it unlikely that this effect would have been strong enough to expel the physical activity variable from the model. The register does not contain information on hospitalisations other than for cardiac interventions. Therefore, the present study potentially underestimates factors that may influence on HRQoL.
Conclusion
In the present study, based on register data, we found an association between NYHA class, symptoms and best possible self-reported HRQoL. This suggests that earlier findings regarding importance of medical factors in association with QoL applies also in a setting with a broad recruitment of patients with ToF. Furthermore, self-reported physical activity >3 h/week was associated with best possible HRQoL, an association never reported before in patients with ToF. A better understanding of factors related to QoL can lead to improvements in the periodic outpatient follow-up programme. Encouraging physical active lifestyle may lead to better HRQoL in patients with ToF; however, prospective interventional studies are warranted.
Acknowledgments
The Swedish Heart-Lung Foundation, Riksförbundet HjärtLung, Umeå University and The County of Västerbotten.
References
Footnotes
Contributors All authors have contributed to data collection, draft, critically reviewed the draft and finally approved the manuscript. ASS, CS, DR and BJ have performed database work and performed the statistical analysis.
Funding This study was funded by Västerbotten Läns Landsting, Norrländska Hjärtfonden, Riksförbundet HjärtLung and Hjärt-Lungfonden.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The investigation was approved by the Regional Ethical Review Board in Umeå, Sweden (Dnr 08-218 M, Dnr 2012 445-32 M and Dnr 2015-212-32 M).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The study is based on the national register SWEDCON where all data are stored.