Article Text

Abstract
Objective The impact of the severity of secondary mitral regurgitation (MR) on the risk of death and heart failure (HF) hospitalisations in patients with reduced left ventricular (LV) systolic function is poorly defined. The study sought to identify the incremental risk of secondary MR in patients with reduced LV systolic function.
Methods We studied 615 consecutive patients with LV ejection fraction ≤35% by transthoracic echocardiography at a single medical centre. Patients were divided into three groups of no MR, mild, or moderate to severe MR. The median follow-up was 2.9 years. The primary endpoint was a composite of death or HF hospitalisations.
Results Compared with patients with no MR, the risk of death or HF hospitalisations was higher for mild MR (HR 1.7, P=0.003) and moderate to severe MR (HR 2.7, P<0.001). The risk was also higher for the component endpoints of HF hospitalisations (mild MR: HR 2.3, P=0.001; moderate to severe MR: HR 3.5, P<0.001) and death (mild MR: HR 1.6, P=0.033; moderate to severe MR: HR 2.6, P<0.001). After adjustment for other covariates, MR was no longer significantly associated with death or HF hospitalisations, or death alone, but remained significantly associated with HF hospitalisations (mild MR: HR 1.7, P=0.028; moderate to severe MR: HR 2.2, P=0.002).
Conclusions In patients with reduced LV systolic function, secondary MR is associated with an increased risk of HF hospitalisations but not death.
- secondary mitral regurgitation
- death
- heart failure hospitalization
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
A strong association between the severity of secondary mitral regurgitation (MR) and all-cause mortality as well as hospitalisation for heart failure has been reported. However, the existing data from multiple studies is discordant. It can be debated if secondary MR is independently associated with all-cause mortality beyond that rendered by the underlying cardiomyopathy and other associated comorbidities.
What does this study add?
Secondary MR is associated with an adverse prognosis in patients with left ventricular systolic dysfunction. However, its impact independent of the underlying cardiomyopathy and other covariates may be on overall morbidity but not on mortality.
How might this impact on clinical practice?
Based on these findings, we believe that interventions to reduce secondary MR in this patient population may improve the quality—but not the quantity—of life. This has clinical implications in the selection of patients undergoing therapies targeted towards mitral valve repair or replacement.
Introduction
Patients with reduced left ventricular (LV) systolic function commonly develop malcoaptation of structurally normal leaflets secondary to altered LV geometry, a condition termed secondary mitral regurgitation (MR). Secondary MR is thought to arise from a combination of factors including altered mitral leaflet tethering due to focal or global LV remodelling, decreased LV closing forces1 and mitral annular dilatation.2 3 The resultant, chronic volume overload imposes additional diastolic wall stress and triggers further LV remodelling and dysfunction thereby perpetuating a vicious cycle.4–6 At the cellular and molecular levels, this pathological process is mediated by excess neurohormonal and cytokine activation, loss of cardiomyocytes and inadequate hypertrophic compensation of the left ventricle.
Despite these deleterious effects, it remains unclear if secondary MR confers an incremental risk beyond that rendered by the underlying cardiomyopathy. While some studies have identified secondary MR as an independent risk factor for increased mortality,7–11 others suggest that the underlying cardiomyopathy primarily drives mortality risk.12–15 The controversy may impact the decision to pursue aggressive management of secondary MR via surgical or transcatheter repair or replacement of the mitral valve.16
The primary objective of our study was to examine the incremental prognostic impact of secondary MR on all-cause mortality and hospitalisations for heart failure (HF) in patients with reduced LV systolic function.
Methods
Patient selection
We reviewed the medical records of patients from the Veterans Affairs (VA) Boston Healthcare System database. Using the Crystal Reports analysis software programme, we included consecutive patients with a left ventricular ejection fraction (LVEF) ≤35% who received a transthoracic echocardiographic (TTE) study for clinically indicated purposes between 1 April 2009 and 31 December 2011. We excluded patients with (1) structural mitral valve disease (more than mild mitral stenosis or prolapse as well as rheumatic or degenerative mitral valve regurgitation), (2) more than mild aortic stenosis or regurgitation and (3) history of mitral valve repair or replacement.
Patient demographics, comorbid conditions and clinical outcomes data—including all-cause mortality and hospitalisations for HF—were collected through retrospective chart review. All charts were reviewed for outcomes data through February 2013. Blood pressure, body surface area, inpatient versus outpatient status and echocardiographic variables were collected from the TTE reports at the time of the index study. Renal function was assessed by the glomerular filtration rate estimated from the Cockroft-Gault equation. Causes of reduced LV systolic function were determined from the medical chart and categorised as ischaemic, non-ischaemic, mixed (ischaemic and non-ischaemic) and unknown. TTE studies were interpreted by board-certified echocardiographers with substantial clinical experience in echocardiography. Given the retrospective nature of the study, no informed consent was required.
Grading MR severity
As any single parameter should not be relied on while grading severity of MR,17 a systematic analysis of the MR severity was performed integrating the following elements as recommended by American Society of Echocardiography17: Vena contracta width (mild when <0.3 cm, moderate when 0.3–0.6 cm and severe when ≥0.7 cm), effective regurgitant orifice area (mild when <20 mm2, moderate when 20–39 mm2 and severe when ≥40 mm2) and regurgitant volume (mild when <30 mL, moderate when 30–59 mL and severe when ≥60 mL), pulmonary venous flow pattern, mitral inflow velocity, density of the MR continuous wave Doppler profile, as well as the MR jet area. Although these parameters were performed in all patients, except for a few with poor image quality, their respective values were not solely relied on in the final determination of MR severity, but rather integrated together for the final interpretation. Evaluation of left atrial (LA) size was used as additional data for grading MR severity.17 LA size was determined by volume assessments as calculated by the biplane area-length formula.18 LA size was graded based on the LA volume indexed to body surface area (normal when LA volume index <29 mL/m2, mildly dilated when LA volume index 29–33 mL/m2, moderately dilated when LA volume index 34–39 mL/m2 and severely dilated when LA volume index ≥40 mL/m2).18
Based on this grading method, patients enrolled in the study were further categorised into three main groups according to MR severity (no MR, mild MR, and moderate to severe MR). For purposes of analysis in our study, patients with moderate MR were combined with patients with severe MR in one group to increase the sample size.
Severity of tricuspid valve regurgitation was assessed by using colour flow and spectral Doppler imaging according to the guidelines proposed by the American Society of Echocardiography.17
Endpoints
The primary endpoint was a composite of all-cause death and hospitalisations for HF. A hospitalisation for HF was defined as any hospital admission during which the patient was identified to have symptoms of acute HF exacerbation (eg, breathlessness, fatigue or ankle swelling) with consistent physical exam findings as documented in the chart (eg, rales on lung exam, elevated jugular venous pressure or peripheral oedema) that required intravenous diuretic therapy. Secondary endpoints included the individual component outcomes of all-cause death and hospitalisation for HF.
Statistical analysis
Continuous variables were expressed as mean and SD or median and IQR. Associations between MR category and continuous and categorical variables were studied using analysis of variance and Χ2 tests, respectively. Survival curves for death or hospitalisation for HF were assessed by the Kaplan-Meier method and the differences between event rates were tested for significance using the log-rank test. The time to primary and secondary endpoints was analysed using univariable and multivariable Cox proportional hazards models. Patients were censored at their last documented encounter in the electronic record. Clinically relevant variables were included in a backward stepwise multivariate model (P for removal >0.05) to determine the variables independently associated with the primary endpoint. A P value <0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 815 patients were reviewed, of which 200 patients did not meet inclusion criteria and the remaining 615 patients (mean age 69±11) were analysed. The median follow-up duration for the study was 2.9 years (IQR 0.8–3.7 years). There were 179 patients (29%) with no MR, 192 patients (31%) with mild MR and 244 patients (40%) with moderate to severe MR.
Clinical and echocardiographic characteristics of patients in the different groups are shown in table 1. As patients were enrolled from a VA medical centre, most patients were male (97.7%). Patients with increasing severity of MR were more likely to be older (P<0.0001), have a history of atrial fibrillation (P=0.035) and coronary artery bypass graft (CABG) surgery (P=0.04) as well as a significantly lower glomerular filtration rate (P<0.0001). MR severity was not associated with the underlying cause of cardiomyopathy (ischaemic vs non-ischaemic) (P=0.73). Severity of MR directly correlated with left ventricle internal dimensions at end diastole (LVIDd) and end systole (LVIDs), with LA dimensions and indexed LA volumes, but was inversely related to the LVEF (P<0.0001). Additionally, patients with more severe MR had significantly higher pulmonary artery systolic pressures (P<0.0001) and more severe tricuspid regurgitation (P=0.001), consistent with the results of prior studies (table 1).9
Baseline characteristics by severity of mitral regurgitation (MR)
Outcomes
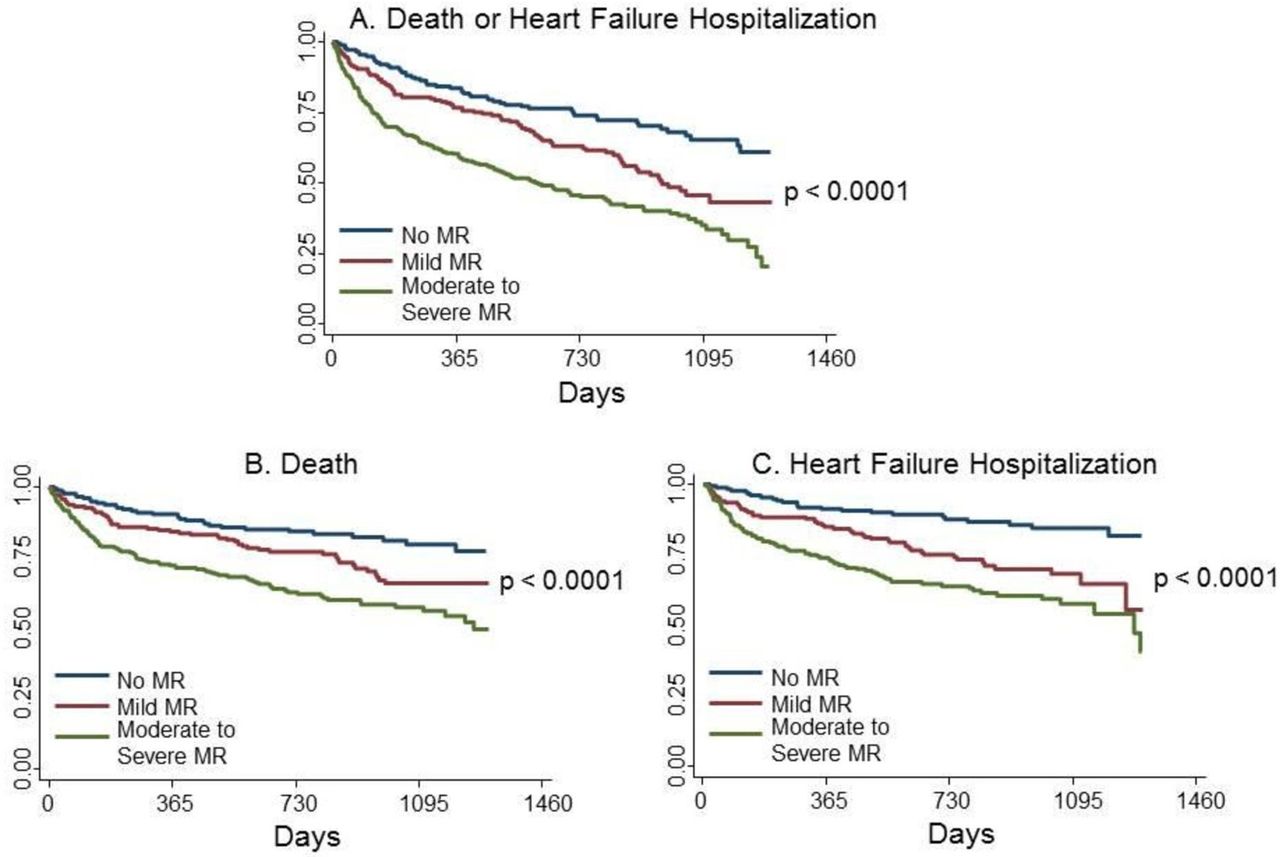
A total of 287 patients (47%) reached the primary composite endpoint of death or HF hospitalisation during the follow-up period. Death occurred in 184 patients (30%), while a hospitalisation for HF occurred in 160 patients (26%). Survival curves for the combined and component endpoints are shown in figure 1, and outcomes were worse with more severe MR.
{kind=link}
Survival curves by severity of mitral regurgitation (MR) for (A) death or heart failure hospitalisation, (B) death and (C) heart failure hospitalisation.
Survival analysis
In univariable analyses, death or HF hospitalisation was significantly related to mild MR (HR 1.7; 95% CI 1.2 to 2.4, P=0.003) and moderate to severe MR (HR 2.7; 95% CI 2.0 to 3.7, P<0.001) (table 2). MR severity was also associated with the component endpoints of hospitalisation for HF (table 3) and death alone (table 4).
Severity of mitral regurgitation and the risk of death or heart failure hospitalisation
Severity of mitral regurgitation and the risk of heart failure hospitalisation alone
Severity of mitral regurgitation and the risk of death alone
Factors significantly associated with the composite primary endpoint included age, inpatient status, any degree of tricuspid regurgitation, history of diabetes mellitus, ACE inhibitor use, diuretic use, atrial fibrillation, LVEF, LVIDd and glomerular filtration rate. After controlling for these variables in a multivariable analysis, the relationship between MR and death or HF hospitalisation was no longer significant (table 2). Similarly, after adjustment of the covariates, there was no significant relationship between MR and death alone (table 4), but MR remained associated with hospitalisations for HF (table 3).
Discussion
Patients with reduced LV systolic function often develop secondary MR due to associated ventricular and atrial remodelling, with ultimate progression of this cyclical, pathological process to worsening clinical heart failure and death.15 19–22 Whether the presence of MR in this population contributes incremental risk beyond that conferred by the underlying cardiomyopathy is unclear. In our study of consecutive patients with reduced systolic function (LVEF ≤35%), the presence of secondary MR was associated with death and HF hospitalisation, but the relationship to this combined endpoint and to death alone was attenuated by adjustment for other covariates. However, the severity of MR was related to HF hospitalisation before and after adjustment for covariates. This suggests a more direct role for the severity of MR on HF hospitalisation, but that the risk of death is related to covariates that associate with MR. Thus, trials of surgical or catheter-based treatments of MR are more likely to reduce HF hospitalisation, but less likely to affect death.
Prior studies have produced conflicting data on the independent impact of secondary MR on morbidity and mortality in patients with LV systolic dysfunction.7–15 Fundamental differences in the cohorts and methodologies employed have likely resulted in divergent study conclusions and continued clinical uncertainty.
Among 558 consecutive patients with advanced LV systolic dysfunction and HF due to ischaemic and non-ischaemic cardiomyopathy, Patel and colleagues found that secondary MR was not independently associated with mortality, although the authors did not examine the risk of recurrent hospitalisations.14 In a prospective multicenter study of 336 patients with New York Heart Association functional class III–IV HF and LVEF of ≤35%, the severity of secondary MR did not predict death, but independently predicted the composite endpoint of death, HF hospitalisations or transplant.13
In contrast, in a more recent study of 1256 patients with ischaemic and non-ischaemic cardiomyopathy and severe LV dysfunction, quantitatively determined secondary MR was an independent predictor of death or HF hospitalisation at a median follow-up of 2.5 years.10 Multivariable analysis in this study did not include clinical factors such as diabetes mellitus, renal function or medication use—covariates that, when employed in our multivariable model, rendered the association between MR and death or HF hospitalisation no longer statistically significant.
A separate study of 303 patients with previous myocardial infarction (>16 days) followed for 5 years demonstrated an association between secondary MR and excess mortality.8 In a subsequent analysis of 173 patients with prior myocardial infarction (>16 days), secondary MR was associated with a threefold increase in risk of congestive heart failure and a higher incidence of the combined endpoint of death or HF after approximately 4 years of follow-up.23
Several reasons have been posited for the variability in these study results but most relate to the complex interplay between secondary MR, LV dysfunction and remodelling. In particular, while possible to adjust for LVEF, it is difficult to control for variations in ventricular remodelling, which may contribute more to long-term risk than associated secondary MR. In fact, of the above studies that reported excess mortality with secondary MR, most were composed of patients with a greater burden of myocardial ischaemia and/or prior infarction—a distinct clinical profile that may be predisposed to poorer outcomes.
Despite discrepant data on clinical outcomes, the consensus remains that secondary MR is associated with an adverse prognosis and therefore warrants targeted therapy.24 While a causal link between secondary MR and mortality would imply that repair of the mitral valve might improve long-term survival, this hypothesis is relatively unsupported by contemporary surgical literature.25–32 In a retrospective study of 390 propensity-matched patients with 3–4+ secondary MR and LVEF <45% undergoing CABG, concurrent mitral valve repair was associated with reduced postoperative MR and improved symptoms, but not with improved long-term functional status or survival.27 Similarly, in a study of 107 patients with severe LV dysfunction (mean LVEF 35%±9%) and moderate to severe secondary MR, mitral valve repair in addition to CABG was effective in eliminating MR, but did not differ from CABG alone in 5 year actuarial survival rates (88 vs 87%).26
More recently, a large retrospective study of 4989 patients with significant CAD, moderate LV dysfunction (mean LVEF=40%–50%) and moderate to severe secondary MR assessed the relative survival advantages associated with medical therapy (n=1800), percutaneous coronary intervention (n=1295), CABG alone (n=1651) and CABG with mitral valve repair or replacement (n=243) over a 20-year period. At a median follow-up of 5.3 years, isolated CABG was associated with the highest adjusted survival (adjusted HR 0.56; 95% CI 0.51 to 0.62, P<0.0001) when compared with medical therapy, and no additional survival benefit was conferred by concomitant mitral valve repair or replacement irrespective of secondary MR severity. The study highlights that long-term survival may be more dependent on relief of ischaemia than on correction of secondary MR, suggesting that both MR and its associated mortality may be driven by pathological remodelling—particularly in the setting of ischaemic heart disease—and a poor ventricular substrate.29
Notably, in the Surgical Treatment for Ischaemic Heart Failure trial assessing medical therapy versus CABG among patients with ischaemic cardiomyopathy and LVEF <35%, the addition of mitral valve repair to CABG (n=49) in patients with moderate to severe MR was associated with improved survival. However, apart from the small sample size and a low median LVEF (25%), mitral valve repair in this study was pursued in a non-randomised fashion at the surgeon’s discretion inducing a possible selection bias wherein surgery was avoided for the relatively sicker study patients.33
The largest and most recent prospective randomised trial included 301 patients with moderate ischaemic MR randomly assigned at 26 sites to CABG alone (n=151) or CABG and mitral valve repair (n=150). The primary endpoint assessed was LV remodelling as measured by end systolic volume index at the end of 1 year and secondary endpoints included a composite of major adverse cardiac or cerebrovascular events and individual endpoints such as mortality, functional status and quality of life. The study did not reveal a difference in LV remodelling. MR was decreased in the group that underwent mitral valve repair and CABG but there was no significant difference between the two groups in major adverse cardiac or cerebrovascular events or in survival at 12 months.32 Two earlier randomised trials of CABG±mitral valve repair demonstrated reduced secondary MR and improved symptoms with mitral valve repair but were underpowered to determine an effect on mortality.30 31
Clinical implications and future directions
Our study supports the hypothesis that secondary MR in the setting of LV dysfunction influences morbidity reflected by HF hospitalisation, but not mortality. Current guidelines recommend aggressive medical therapy as the cornerstone of secondary MR management in patients with severe cardiomyopathy, followed by CRT and revascularisation in those who meet clinical indications.34 Mitral valve repair or replacement may play a role in patients who are refractory to the above therapies. As the goals of therapy often shift in patients with advanced heart failure, mitral valve repair or replacement in the appropriate context may promote improved quality over quantity of life. The ongoing Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation trial assessing a catheter-based mitral valve therapy in patients with HF with significant secondary MR will help determine the efficacy of mitral valve repair. Our study would suggest that it will have a greater effect on HF hospitalisation than on death.
Strengths and limitations
The major strength of this study is the inclusion of a broad list of patient comorbidities as well as relevant medications and echocardiographic variables which were included in the multivariable analysis. In addition, a comprehensive integrative approach in the assessment of MR severity was carried out in all study patients, as recommended by most recent American Society of Echocardiography guidelines.17
Several limitations, however, must be acknowledged. Our study was retrospective and 97.8% of the patients in the study were men reflecting a typical VA population. In addition, complete coronary angiography data was not available in all patients; thus, we were unable to account for the extent of coronary artery disease in our analysis. Finally, specific causes of death, particularly from cardiovascular causes, were not accounted for in our analysis.
Conclusion
In a large, consecutive population of veterans with reduced LV systolic function, the severity of secondary MR was associated death or HF hospitalisation. After risk adjustment by other covariates, the relationship of MR to death was no longer significant. However, MR remained significantly associated with the risk of HF hospitalisation in multivariable models. Thus, interventions to reduce secondary MR in patients with reduced LV systolic function may have a greater effect on HF hospitalisation than death.
References
Footnotes
This study was conducted in the Veterans Administration Boston Healthcare System in West Roxbury, Massachusetts, USA. The findings of this study were presented in poster format at the American Society of Echocardiography Scientific Sessions in Minneapolis, Minnesota, USA, 2013.
SM and AD contributed equally.
Contributors SM and AD: study design and interpretation of data; drafting of manuscript. JRG, KGA and SE: interpretation of data and revision of manuscript. GP: study design and revision of manuscript. ZC: study design and interpretation of data; revision of manuscript. SK: analysis and interpretation of data; revision of manuscript. JA: study design and analysis/interpretation of data; revision of manuscript.
Competing interests None declared.
Ethics approval The VA Central Institutional Review Board.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement No additional data are available.