Article Text

Abstract
Objectives The aim was to determine the prevalence of different degrees of kidney dysfunction and to examine their association with short-term and long-term outcomes in a large unselected contemporary heart failure population and some of its subgroups. We examined to what extent the different cardiac conditions and their severity contribute to the prognostic value of kidney dysfunction in heart failure.
Design We studied 47 716 patients in the Swedish Heart Failure Registry. Patients were divided into five renal function strata based on estimated glomerular filtration rate (eGFR) using the Chronic Kidney Disease Epidemiology Collaboration equation. The adjusted association between kidney function and outcome was examined by Cox regression.
Results 51% of the patients had eGFR <60 mL/min/1.73 m2 and 11% had eGFR <30. There was increasing mortality with decreasing kidney function regardless of age, presence of diabetes, New York Heart Association NYHA class, duration of heart failure and haemoglobin levels. The risk HR (95% CI) persisted after adjusting for differences in baseline characteristics, severity of heart disease, and medical treatment: eGFR 60–89: 0.86 (0.79 to 0.95); eGFR 30–59: 1.13 (1.03 to 1.24); eGFR 15–29: 1.85 (1.67 to 2.07); and eGFR <15: 2.96 ([2.53 to –3.47)], compared with eGFR ≥90.
Conclusions Kidney dysfunction is common and strongly associated with short-term and long-term outcomes in patients with heart failure. This strong association was evident in all age groups, regardless of NYHA class, duration of heart failure, haemoglobin level, and presence/absence of diabetes mellitus. After adjusting for differences in baseline data, aetiology and severity of heart disease and treatment, the strong association remained.
- HEART FAILURE
- KIDNEY DISEASE
- PROGNOSIS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Kidney failure, a known comorbidity in heart failure, is a part of the cardiorenal syndrome and associated with reduced survival.
What this study adds?
In the study of the whole spectrum of reduced kidney function in a large unselected heart failure population and examination of the prognostic value of kidney dysfunction in important subgroups, we found that there is strong association between kidney dysfunction and outcomes in all age groups, regardless of New York Heart Association (NYHA) class, duration of heart failure, haemoglobin level and presence or absence of diabetes mellitus. This strong association remains even after adjustment for confounders, aetiology, and severity of heart disease and its treatment.
How this might impact on clinical practice?
A simple measure of renal function in patients with heart failure will, adjusted or unadjusted, regardless of age group, presence of diabetes, NYHA class or anaemia, be an indicator of a patient's short and long-term prognosis. Our findings emphasise the importance of close follow-up and kidney preservation in patients with heart failure and kidney disease.
Introduction
Heart failure is a serious condition with high mortality despite all modern treatment.1 Many factors contribute to the poor outcome in heart failure.2 Kidney dysfunction occurs in acute and chronic heart failure, and is associated with reduced survival.3 Over the years, our knowledge of the interaction between the heart and the kidney has increased, and parts of the pathophysiological background for the cardiorenal syndrome have been established.4 The heart and kidney function are closely linked together by haemodynamics, neurohormones and the sympathetic nervous system.5
The cardiorenal syndrome is complex as heart failure and kidney disease share common risk factors and potentiate each other and other cardiovascular diseases.6 Most of the previous studies examining the prognostic value of kidney function in heart failure patients have been hampered mainly by inclusion of highly selected randomised controlled trial patients or small sample sizes, and have not been able to examine the whole spectrum of kidney dysfunction.7 ,8 In earlier large studies, the diagnoses of kidney disease have mainly been based on diagnostic codes,9 ,10 or defined only by a certain level of creatinine.11 Most previous studies have examined short-term prognosis, whereas long-term follow-up has been uncommon.12 ,13 Moreover, descriptions of the prognostic value of kidney dysfunction in important subgroups have been lacking.
The aim of this study was to determine the prevalence of different degrees of kidney dysfunction and to examine their association with short-term and long-term outcome in a large unselected contemporary heart failure population and some of its subgroups. We also wanted to examine to what extent different cardiac conditions and their severity contribute to the prognostic value of kidney dysfunction in heart failure patients.
Methods
The Swedish heart failure register (SwedeHF) has been described in detail elsewhere.14 SwedeHF has since 2000 included patients with chronic heart failure and offers a unique possibility to study a large cohort of unselected heart failure patients.
It is a web-based national quality register including unselected heart failure patients, of whom 55% are registered during hospitalisation, while the remaining are registered in an outpatient setting at the hospital or in primary care. Inclusion criteria are clinician-judged heart failure and approximately 80 variables are recorded at discharge or during visit to a physician or healthcare team. The patients are informed of their participation in the SwedeHF and are allowed to opt out, but individual patient consent is not required. Uppsala Clinical Research Center (Uppsala, Sweden) is managing the database. Variables in the registry include baseline description of the patients, risk factors, history of heart disease, cardiac interventions, cardiac evaluation (ECG and echocardiogram), medication, and laboratory tests at discharge or at the outpatient visit. The protocol, registration form and annual report are available at http://www.rikssvikt.se
Only centres using creatinine measurements from methods that are traceable to isotope dilution mass spectroscopy standards were included. Glomerular filtration rate (eGFR) was estimated with the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.15 All patients were divided according to the current National Kidney Foundation Kidney Disease Outcomes Quality Initiative (KDIGO) recommendations into five renal function categories with eGFR (mL/min/1.73 m2): higher or equal to 90 (eGFR ≥90, normal function), eGFR higher or equal to 60 but below 90 (eGFR 60–89, mild dysfunction), eGFR higher or equal to 30 but below 60 (eGFR 30–59, moderate dysfunction), eGFR higher or equal to 15 but below 30 (eGFR 15–29, severe dysfunction) and eGFR less than 15 (eGFR <15, end stage renal disease (ESRD)).16 Owing to lack of data on albuminuria, these categories can only be considered as renal function strata and not chronic kidney disease (CKD) stages.
Information about mortality was obtained by linkage with the Swedish population registry, which includes the vital status of all Swedish citizens. The registry and the study conform to the declaration of Helsinki and the study was approved by the local ethical authority.
Statistics
Continuous variables are presented as median and IQR, and categorical variables are presented as counts and proportions (%). p Values for trends were assessed by Pearson χ2 for proportions and Kruskal-Wallis test for continuous variables. The index date was date of admission to hospital or date of outpatient visit, respectively. Crude survival was assessed and illustrated by Kaplan-Meier analyses. After graphically checking the model assumption of proportional hazard, univariable and multivariable Cox proportional hazard regression was used to examine the association between kidney function and outcome. In the first model, we adjusted for baseline variables possibly influencing both kidney dysfunction and outcome (age, gender, smoking, hypertension and diabetes). In the second model, we added variables related to the aetiology and severity of heart failure (heart failure >6 months, ischaemic heart disease, atrial fibrillation, valvular heart disease, dilated cardiomyopathy, previous revascularisation, previous valvular intervention, non-sinus rhythm in the electrocardiogram, heart rate, left ventricular ejection fraction (LVEF), New York Heart Association (NYHA) class, systolic blood pressure and haemoglobin level). In the third model, we also adjusted for the given treatment (ACE inhibitors, angiotensin-receptor blocker (ARB), β-blockers, aldosterone antagonists, statins and cardiac resynchronisation therapy (CRT)). To ensure linearity, the univariable association of different categorisations of the continuous variables and outcome was examined. Body mass index and heart rate were divided into quartiles before entry into the models, and age was divided into age/10 years. Haemoglobin (Hb) and systolic blood pressure were divided in to four clinically-based categories: Hb >150 g/L (as reference), Hb 120–149 g/L, Hb 90–119 g/L, and Hb <90 g/L; systolic blood pressure >140 mm Hg (as reference), 110–139 mm Hg, 90–109 mm Hg, and <90 mm Hg.
Results
From 11 May 2000 to 3 October 2013, a total of 88 317 registrations occurred in SwedeHF. Only the first registration in the registry were included, and patients who lacked information on age, creatinine and confirmation that creatinine had been measured by a standardised method were excluded. Thus, 47 716 patients were included in the analyses (figure 1).
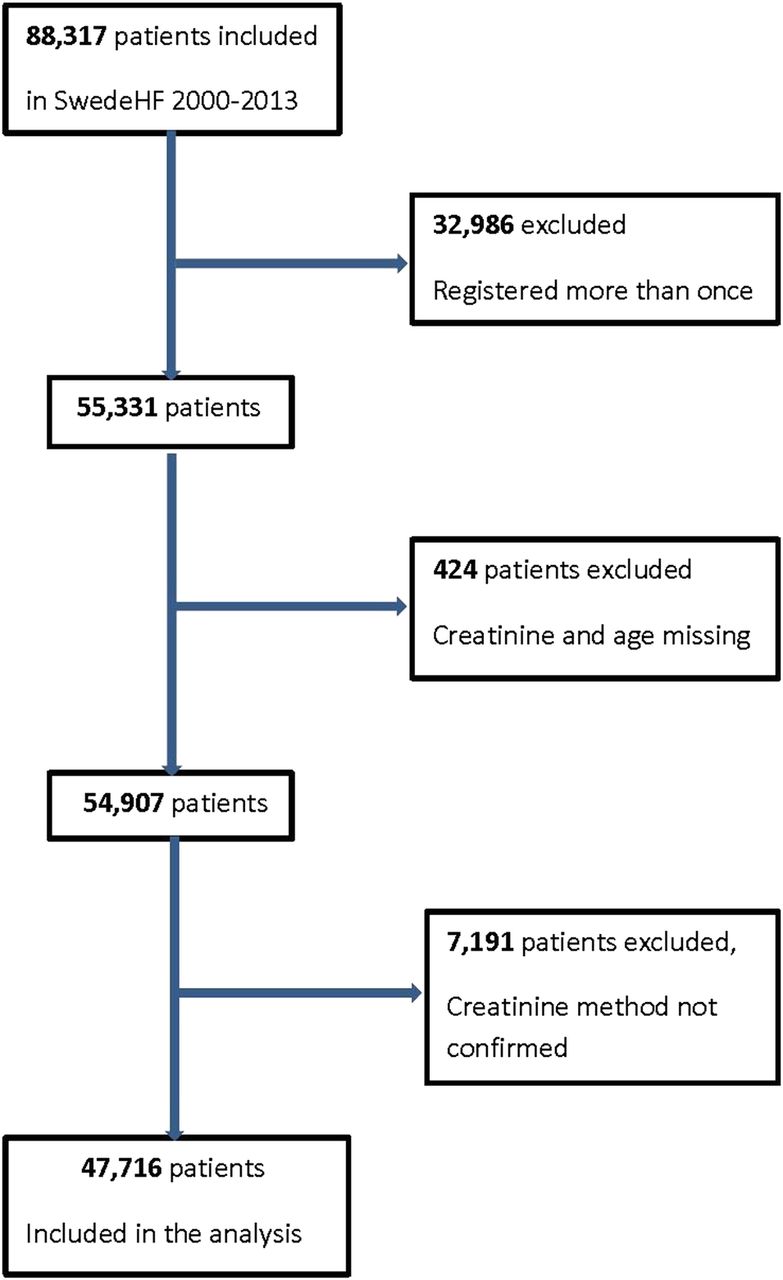
Patients included in the study. SwedeHF, Swedish heart failure register.
Kidney function and heart disease
A total of 24 225 (51%) patients had moderate kidney dysfunction (eGFR <60 mL/min/1.73 m2) and 5065 (11%) had a severe kidney dysfunction (eGFR <30 mL/min/1.73), of which 813 (2%) was classified as ESRD (eGFR <15 mL/min/1.73 m2; table 1).
Baseline characteristics
The median (IQR) age of the population was 77 (67–84) years with higher age in those with worse kidney dysfunction (table 1). Patients with lower kidney function were more often female with more hypertension and diabetes mellitus.
Also, patients with poor kidney function more often had ischaemic heart disease; however, they had a similar rate of previous revascularisation. Atrial fibrillation, stroke and valvular heart disease were more common in those with poor kidney function; however, they less often had dilated cardiomyopathy. Patients with lower kidney function more often had heart failure with a known duration of more than 6 months and were more often hospitalised at inclusion. Mildly symptomatic heart failure was more common in those with preserved kidney function and severe heart failure increased with worsened kidney function. Preserved ejection fraction was more common in those with low eGFR, whereas severe left ventricular systolic dysfunction (LVEF <30%) was more common in those with preserved kidney function.
Physical findings
Regarding heart rate, blood pressure and body mass index, there were no major differences between the eGFR strata (table 2). Presence of left bundle branch block and QRS width did not differ between eGFR strata. The laboratory data showed that patients with low eGFR more often exhibited low haemoglobin and a high potassium level, and a markedly higher level of N-terminal pro-brain natriuretic peptide (NT-proBNP).
Physical signs, laboratory results and medical treatment
Treatment
Patients with low kidney function were less likely to be treated with ACE inhibitor, β-blockers, and aldosterone blockade (table 2). If treated, they were also less likely to receive what was considered by guidelines to be the target dose of ACE inhibitor, ARB and β-blockers. Statins and anticoagulant treatment were used less often whereas aspirin was used more often in those with poor kidney function.
Outcome
Almost one-third of the hospitalised patients in the poorest eGFR strata (eGFR <15) died during the actual hospitalisation. Half of all patients with ESRD (eGFR <15) had died after 6 months and after 1 year, over 40% of those with severe kidney dysfunction (eGFR 15–29) and 60% of the patients with ESRD (eGFR<15) had died (table 3).
Mortality and unadjusted and adjusted mortality risk in relation to eGFR
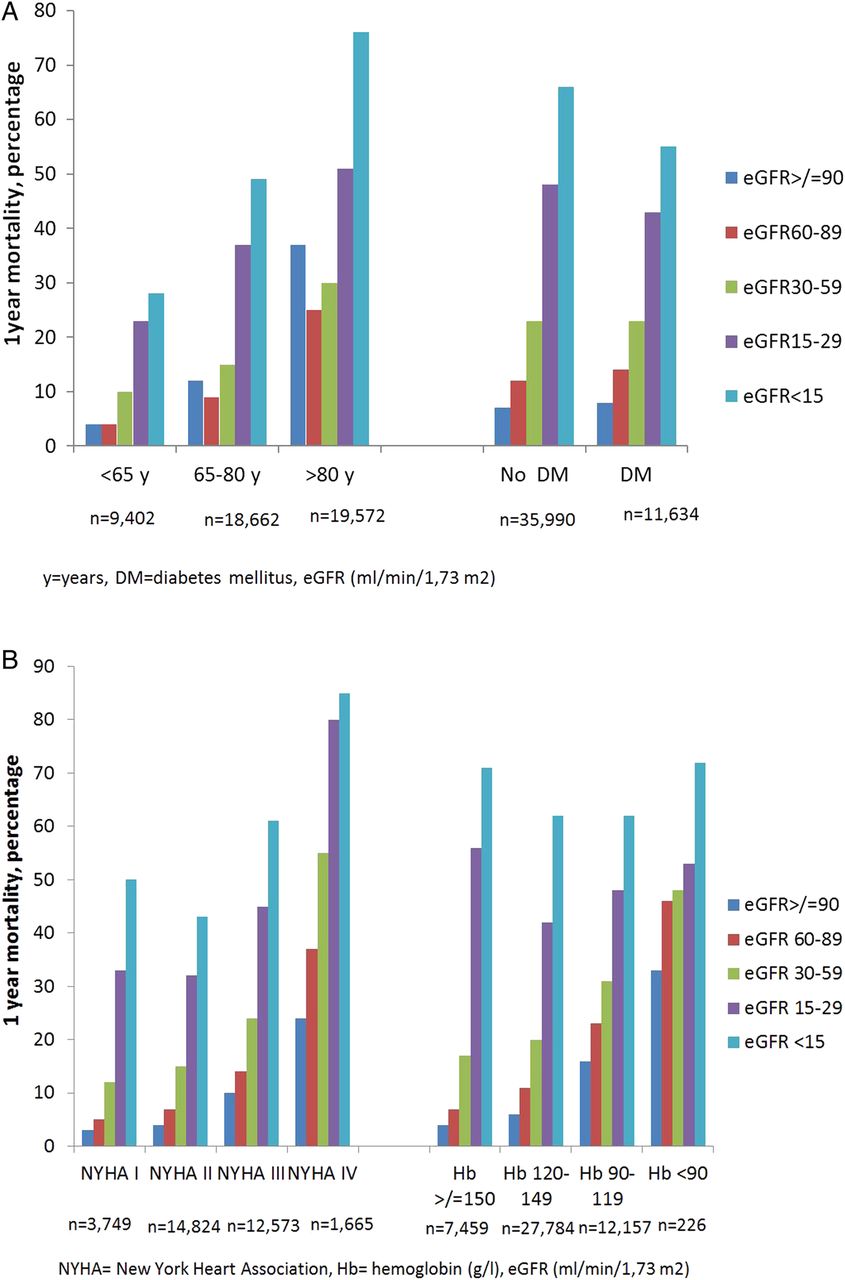
There was an increasing mortality with decreasing kidney function regardless of age, presence of diabetes or not, NYHA class, and haemoglobin levels (figure 2A, B).

(A) 1-year mortality in relation to estimated glomerular filtration rate (eGFR), age (n=47 636) and presence of diabetes mellitus (n=47 624). (B) 1-year mortality in relation to eGFR and New York Heart Association class (n=32 811) and haemoglobin level (n=47 626). DM, diabetes mellitus; y, years.
Although patients with heart failure for more than 6 months had a higher 1-year mortality than patients with heart failure of a shorter duration (25% vs 16%), the prognosis was mainly dependent on the eGFR. One-year mortality in patients with normal kidney function was 7% for heart failure under 6 months versus 8% for heart failure over 6 months; in patients with eGFR< 15, the 1-year mortality was 61% versus 63% (see online supplementary table S1).
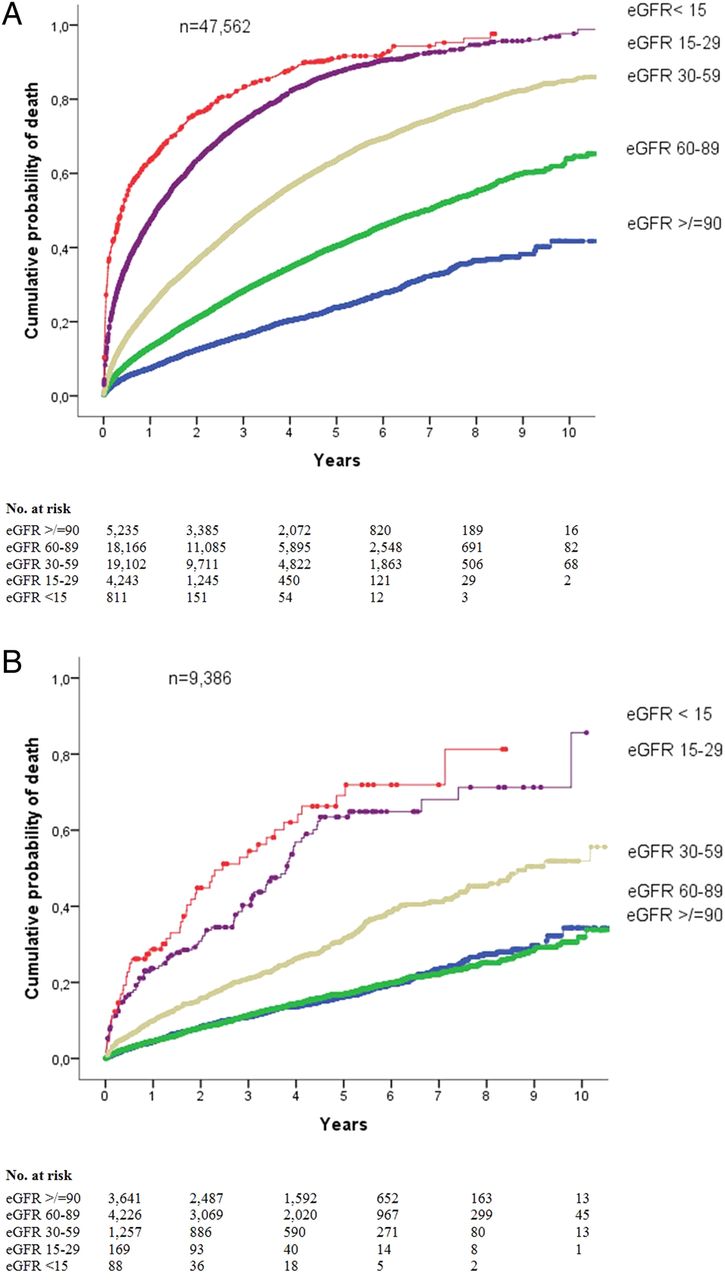
During long-term follow-up, the cumulative probability of death in 5 years was above 80% in patients with at least severe kidney dysfunction (eGFR <30), and 60% in those with moderate kidney dysfunction (eGFR 30–59; figure 3A). Even in the age group below 65 years, the prognosis was sinister with a 60% probability of death in 5 years for those with severe kidney dysfunction (figure 3B).
{kind=link}
{kind=link}
{kind=link}
(A) Mortality in patients with heart failure and different estimated glomerular filtration rate (eGFR) strata, crude survival assessed by Kaplan-Meier analysis, log rank p<0.001. (B) Mortality in patients under 65 years with heart failure and different GFR strata, crude survival assessed by Kaplan-Meier analysis, log rank p<0.001.
When adjusting for baseline variables possibly influencing both kidney dysfunction and outcome (age, gender, smoking, hypertension and diabetes) in model 1, the association between eGFR and mortality was attenuated (table 3). When adding heart failure-related variables in model 2, the association between eGFR strata and mortality was further somewhat weakened, but still significant. When adjusting for differences in medical treatment in model 3, the association between eGFR strata and mortality remained unchanged.
Discussion
The present study has several important findings. First, kidney function is indeed strongly associated with short and long-term mortality in heart failure patients. In hospitalised patients, the inhospital mortality increased from 2% in those with normal kidney function (eGFR >90) to 30% in those with ESRD (eGFR <15). For 5-year mortality, this cumulative probability of death was above 60% in those with moderate kidney dysfunction and above 80% in patients with severe kidney dysfunction. Second, this strong association with outcome was evident in all age groups regardless of NYHA class, duration of heart failure, haemoglobin level and presence or absence of diabetes mellitus. Third, after a stepwise adjustment for differences in baseline data, aetiology, and severity of heart disease and treatment, the strong association remained.
Damman et al3 has recently, in a meta-analysis including more than 1 million patients, clearly demonstrated the strong association between kidney function and outcome.
Our study is so far the largest and most extensively covariate-adjusted cohort study on the association between kidney dysfunction and outcome in an unselected heart failure population. The size of the study and the long-term follow-up allowed us to examine the whole spectrum of kidney disease and its association with subsequent mortality. It was also possible to examine the prognostic influence of different degrees of kidney dysfunction in important subgroups and it provides us with important findings regarding these patients’ risk profile.
In our registry, half of the patients had at least a moderate kidney dysfunction (eGFR <60 mL/min), which is in line with earlier observations.17 For lower kidney function, the patients were older and more often had hypertension, diabetes mellitus and other cardiovascular disease as seen in other studies.18 They also more often had a long duration of disease and more severe NYHA class, in line with other previous studies.19
The higher mortality in patients with kidney dysfunction seen in the present study, compared to several previous studies,13 ,20 is probably explained by the unselected nature of the material. Since this is registry data collected from the clinical routine, patients were considerable older (median age of 77 years) than in the other studies.12 ,21 However, even though the mortality was lower in patients under 65 years of age, there was still a high 5-year mortality, well in line with earlier results in more selected population.22
The associations between kidney function and outcome was similar regardless of age, NYHA class, duration of heart failure, haemoglobin level and presence or absence of diabetes. Notably, when kidney function was known, presence of diabetes had very little effect on mortality (figure 2A). Furthermore, in patients with at least severe kidney dysfunction, the mortality was very high and the additive prognostic value of NYHA class and haemoglobin level limited.
There are several possible reasons for the association between kidney dysfunction and outcome in the present population. The worse prognosis can at least partially be explained by a higher prevalence of traditional risk factors such as higher age, hypertension and diabetes. Though, even after adjustments for these risk factors, impaired kidney function remained strongly associated with mortality confirms results from earlier observations indicating that GFR is an independent predictor itself for outcome.18
Kidney dysfunction may be secondary to venous congestion, forward failure, renin-angiotensin-aldosterone system (RAAS) stimulation and sympathetic activation in heart failure, but may also suppress the cardiac function further. In the present study, adjusting for factors related to aetiology and severity of heart failure reduced the association between the degree of kidney dysfunction and outcome, but to a limited extent. This can be explained by residual confounding that arises from unmeasured or dichotomised variables. However, it may also indicate that factors that are strongly related to kidney dysfunction, such as activation of neurohormones, immunological activation, inflammation and uraemia, are of crucial importance for outcome as these affect vital organs.23
Several studies have shown that patients with cardiovascular disease and CKD receive less of guideline recommended treatments, partly due to lack of evidence from clinical trials and concerns regarding drug toxicity.13 In the present study, differences between eGFR strata regarding the use of antithrombotic treatment, statins and β-blockers were rather small despite the large differences in age distributions. Patients with low eGFR were less often treated with ACE inhibitors and less often reached target doses of RAAS blockade. However, though these drugs are believed to be beneficial even with severely depressed kidney function caution is recommended when treating patients with CKD.7 ,24 ,25 When adjusting for treatment in our study, the association between kidney function and outcome remained unchanged. This may indicate that under treatment is not an important cause of the association between kidney dysfunction and outcome.
There are limitations to this study. This is a registry that reflects clinical practice. There may be a certain selection of patients, as some patients may not have been included in the register because of frailty, comorbidity, or other reasons. This may affect the generalisability of our study. However, compared to many other studies, our study sample should be considered as fairly unselective, closely reflecting the everyday clinical practice. Patients are included according to clinician-judged heart failure, which due to the heterogeneity of the disease and difficulty in establishing the correct diagnoses is likely to contain a certain degree of misclassification. The register has no information of creatinine over time and no data regarding blood urea nitrogen. Dialysis status was not collected as part of the SwedeHF and hence this cannot be reported; however, in an earlier SwedeHF study with linkage to the Swedish Patient Registry, dialysis was used in about 1% of the patients.26 In spite of adjusting for a large number of confounders, residual confounding may still exist due to unmeasured factors that could not be adjusted for.
In conclusion, this large and extensively covariate-adjusted study from a nationwide and generalisable registry shows that kidney dysfunction is strongly associated with short-term and long-term outcome in patients with heart failure. These findings emphasise the importance of close follow-up and kidney preservation in patients with heart failure and kidney disease.
Acknowledgments
The authors would like to thank the steering group of the Swedish Heart Failure Registry, and all the hospitals and outpatient clinics that report to the registry.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors IL, KS and TJ have worked with all parts of the study. LHL, IH and UD were involved with the planning of the study, analysing and interpretation of the data, and the revising of the manuscript. All authors have approved the manuscript and its submission. There has been no relationship with the industry.
Funding This work was supported by the Swedish Foundation for Strategic Research, the Swedish Heart and Lung Foundation and the Stockholm County Council (ALF project). KS was supported by the Stockholm County Council (clinical post-doctoral appointment).
Competing interests UD reports grants from Astra Zeneca Inc, other from Novartis Inc, outside the submitted work. LHL has received grants to his institution from Boston Scientific and Astra Zeneca, and honorary for lecturing from Novartis. TJ has received honorary from Astra Zeneca for lecturing and consulting. KS has received lecture honorary from Astra Zeneca and Aspen.
Ethics approval Ethics Committee of Stockholm.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.