Article Text

Abstract
Introduction Valvular heart disease (VHD) is an increasingly important cardiac condition, driven by an ageing population and lack of progress in the development of medical therapies. There is a dearth of accurate information to guide decision-makers in the development of strategies to combat VHD, and no population-based study has been performed specifically to investigate its contemporary epidemiology. This document describes the design and methodology of the OxVALVE population cohort study (OxVALVE-PCS), which was conceived to address this need.
Methods and analysis Participants aged 65 years and older attending a participating general practice in Oxfordshire, UK, are invited to attend a screening examination. Exclusion criteria include previously diagnosed VHD, inability to provide consent, terminal illness or excessive frailty. Demographics, a focused cardiovascular history and vital signs are recorded at the initial screening examination, accompanied by an echocardiogram. Any finding of significant VHD triggers a separate, more formal echocardiographic assessment (including acquisition of a three-dimensional dataset) and collection of blood samples for future genetic and biomarker analysis. Participants provide consent for longitudinal follow-up and enrolment in future cohort substudies. We also assess the acceptability of community-based echocardiographic examination and compare self-assessed quality of life between those with and without VHD.
Conclusions OxVALVE-PCS will provide contemporary epidemiological data concerning the community prevalence of undiagnosed VHD, facilitate accurate deployment of scarce resources to meet the anticipated increase in demand for VHD-associated healthcare and create a series of subcohorts with carefully defined genotypes and echocardiographic phenotypes for long overdue clinical studies.
Ethics and dissemination This study was approved by the local research ethics committee (Southampton, UK; REC Ref: 09/H0502/58).
Results Results will be submitted for publication in peer-reviewed scientific journals.
- Valvular Disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
-
Valvular heart disease is becoming an increasingly important problem due to the aging of the population.
-
Accurate information on the epidemiology and the natural history of the different forms of valve disease in the modern era is limited.
-
The OxVALVE population cohort study aims to investigate the contemporary epidemiology of previously undiagnosed valvular heart disease in the elderly.
Introduction
Valvular heart disease (VHD) is a significant cause of morbidity and mortality in the general population.1 There are few randomised controlled trials of medical therapy, all with negative results,2–4 and international guidelines are largely based on expert consensus.5 VHD is poorly researched at basic scientific and clinical level in comparison to other areas of cardiovascular disease. Principal limitations are the diverse nature of patients with VHD, inability to identify individuals at the earliest stages of disease and lack of an appropriate investigational infrastructure. VHD is frequently asymptomatic and can present late, and often requires significant interventions (surgical or percutaneous) after symptomatic presentation. Early detection and intervention may improve outcome and it is anticipated that detection could be undertaken in some primary care settings.
Previous population-based studies examining the prevalence of VHD have a number of limitations. Most were conducted via retrospective review of echocardiographic data collected initially to characterise ventricular structure and function,6–9 while one which prospectively recorded valvular disease was primarily focused on calculations of left ventricular mass.10 Furthermore, all of these studies were initiated in the previous millennium—as the population ages rapidly, there is a pressing need for contemporary epidemiological data.
We designed the OxVALVE population cohort study (OxVALVE-PCS) to specifically examine the prevalence of VHD in a contemporary cohort of elderly men and women living in Oxfordshire, UK. Collection of a well-characterised and annotated database of a large number of cases of VHD, including the full variety of types and severity, will also allow the identification of specific suitable populations for future clinical research studies. Such studies may not be confined to pharmacological interventions, but may include surgical and percutaneous procedures, novel imaging techniques and devices, genetic associations or new paradigms of clinical management, including evaluation of the impact of community screening and integration within primary and secondary healthcare service provision. Lay participants have contributed to the design and implementation of the programme. In this article, we focus on the design of the initial cross-sectional study and include details of follow-up where appropriate.
Study objectives
Primary
To establish a longitudinal cohort of patients with previously undiagnosed VHD via an echocardiographic screening programme.
Secondary
-
To define the prevalence of VHD in the Oxfordshire population.
-
To assess the influence of covariates, such as prior cardiovascular events, family history, obstetric history, body mass index (BMI) and medications on the likelihood of VHD.
-
To assess and compare morbidity and mortality in participants with and without VHD.
-
To explore the association between VHD and socioeconomic status.
-
To assess the acceptability of echocardiographic screening for VHD and to identify the extent and predictors of anxiety experienced.
-
To establish well-annotated phenotypes with linked and stored blood samples in the study population for future research.
-
To establish the prevalence of other cardiovascular disorders (in particular hypertension and left ventricular dysfunction) in participants not known to have VHD.
Methods and analysis
The OxVALVE protocol was developed according to STROBE guidelines for the conduct and reporting of observational studies.11
Study design and overview
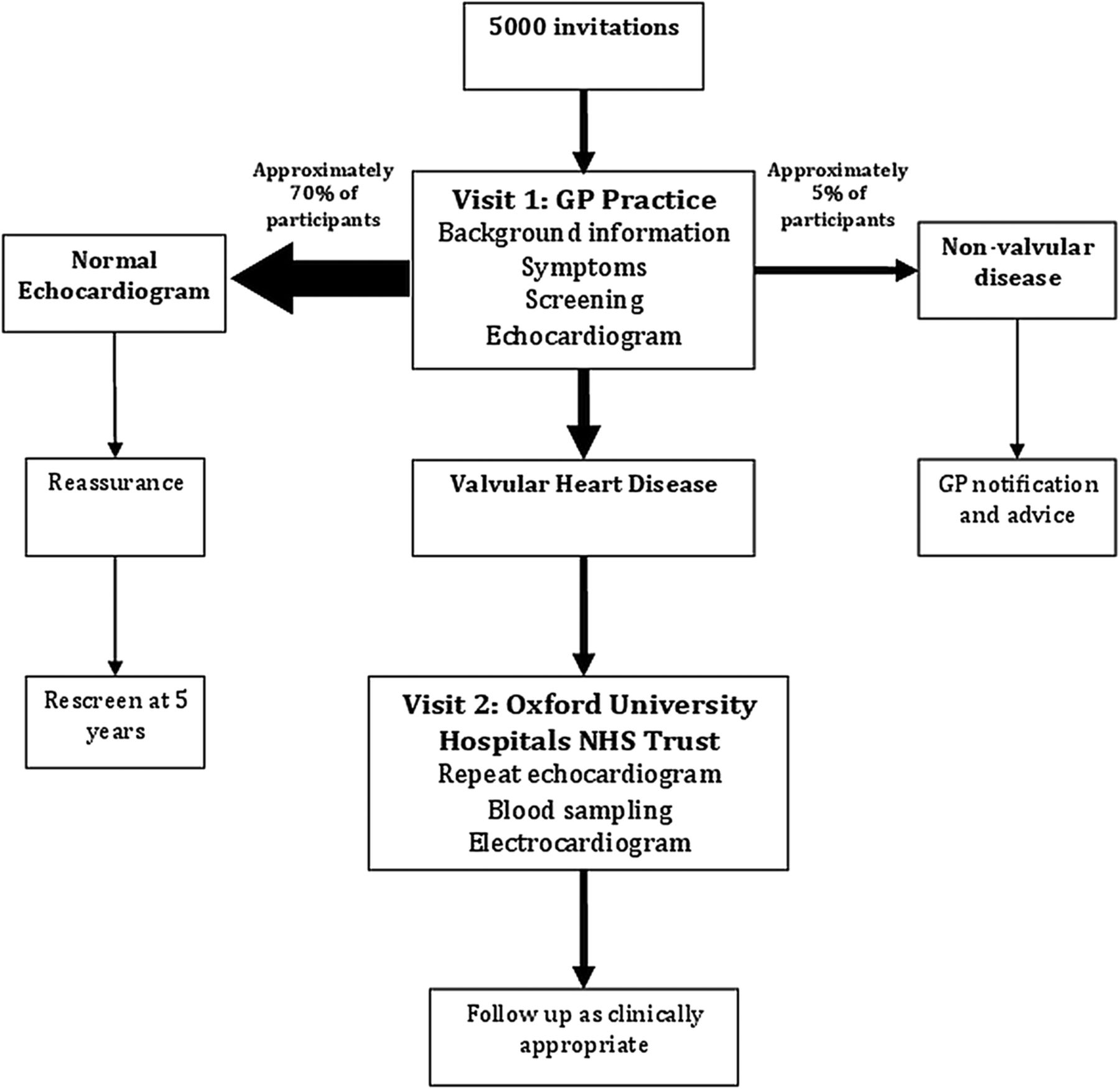
OxVALVE-PCS is a prospective cohort study examining the prevalence, incidence and outcomes of participants aged 65 and older with newly diagnosed VHD. Participants attend an initial visit at their local general practice, followed by a second visit at their local hospital if VHD is detected (figure 1).
{kind=link}
Overview of the OxVALVE population cohort study (GP, general practitioner; NHS, National Health Service).
Setting
We invited a number of general practices within Oxfordshire to participate in the study. Recruitment began in 2009 and is expected to continue until 2015. The first study visit with screening echocardiography is held in the general practice, and those with newly diagnosed VHD are invited to a second visit at Oxford University Hospitals Trust (a secondary and tertiary referral network of hospitals serving Oxfordshire). Clinical data are collated at visit 1 using OpenClinica open source software V.3.0.4.1 (OpenClinica LLC, Waltham, Massachusetts, USA).
Participants
The entire population of each participating practice is screened and all those aged 65 years or greater without known VHD are invited to participate. Exclusion criteria are a previous diagnosis of VHD (identified using relevant diagnostic codes), terminal illness, immobility or general frailty (as judged by the general practitioners (GPs)), or inability or unwillingness to provide informed consent. Potential study participants are identified from practice lists by the practices themselves—all patient identifiable information is held by the GPs until participants consent to take part in the study. The Oxfordshire population aged 65 years and over consisted of 103 742 adults in the 2011 census (45% men), with ethnicity as follows: Caucasian 97.8%, Asian 1.1%, African-American 0.6%, mixed ethnicity 0.3%, other ethnicity 0.1%.12 Potential participants are invited by letter with a single follow-up reminder to non-responders. Telephone contact was not permitted by the Research Ethics Committee. Those declining participation are asked to fill in a brief response indicating their reasons to allow detection of study bias.
Study details
Visit 1
Participants attend a dedicated research clinic at their general practice, where they undergo an eligibility check; provide informed consent, baseline demographics and a brief medical history and undergo a limited cardiovascular physical examination followed by transthoracic echocardiography. Participants are asked to self-complete two questionnaires, and provide comments about their participation in the study. When necessary, the National Health Service (NHS) Language Line Interpreting Service is used to ensure that all participant queries relating to the study are answered and that true informed consent is granted.
Classification
Participants are classified according to whether they have a normal echocardiogram, newly diagnosed VHD or an alternative cardiac pathology (figure 1). Each participant, along with his or her GP, is sent a letter summarising the findings and any further action plan. The threshold for inclusion in the screen-positive group is intentionally low to allow all manifestations of VHD to be captured with careful prospective follow-up. Participants in this group are invited to attend a specific OxVALVE clinic at a site within the Oxford University Hospitals NHS Trust for more detailed characterisation.
Visit 2
Participants with newly noted VHD undergo an ECG, a more sophisticated echocardiogram and blood sampling. A letter confirming the echocardiographic findings is sent to the participants and their GPs.
Follow-up
Participants with a normal echocardiogram are invited to attend a follow-up visit 5 years after initial evaluation to determine the period incidence of VHD and assist in the identification of initial ‘false-negative’ findings. Participants are also tracked via UK national databases (Medical Research Information Service, Hospital Episode Statistics and Myocardial Ischaemia National Audit Project) in order to provide a comparison of morbidity and mortality between screen-positive and screen-negative groups. We recognise that there may be participants with false-negative scans in the screen-negative group—the proposed follow-up programme will assess the clinical importance of an initial negative screening echocardiogram rather than a definitive absence of VHD. Continued follow-up in accordance with current European Society of Cardiology guidelines is offered to those with clinically significant newly diagnosed VHD or alternative cardiovascular pathology.
Variables
The primary measure is the new diagnosis of VHD detected by echocardiography performed in the primary care setting.
Secondary measures are:
-
Impressions of screening (questionnaire assessment)
-
Morbidity and mortality (national database tracking)
-
Health status measurement (EuroQol-5D (EQ-5D))
-
Left ventricular function
-
Two-dimensional (2D) measurements of major cardiac structures (ventricles and atria)
-
ECG abnormalities
-
Biomarker abnormalities
Predictor and confounder variables recorded are demographics, medical and social history, medication, blood pressure, BMI, genetic profile and socioeconomic status.
Data sources/measurement
Clinical assessment
At visit 1, information is obtained concerning age, gender, time spent in countries other than the UK, ethnicity, cardiovascular medical history, smoking status, medication and the presence or absence of heart failure symptoms (New York Heart Association classification (NYHA) or chest pain (Canadian Cardiovascular Society (CCS) score)).13 Women are asked the number of pregnancies and details of any associated complications. A focused clinical examination is then performed consisting of height, weight, pulse and blood pressure (Omron M6 blood pressure monitor, Kyoto, Japan) and assessment of the presence or absence of ankle oedema. An echocardiogram is performed and the participants complete two questionnaires.
Echocardiography—visit 1
Echocardiography is performed by the British Society of Echocardiography (BSE) accredited sonographers or physicians using a Vivid-Q portable machine (Vingmed-General Electric, Horton, Norway)—the same pool of operators also perform visit 2 scans. BSE accreditation is directly comparable to European Association of Cardiovascular Imaging accreditation in transthoracic echocardiography (with which there is reciprocal recognition). A two-beat clip for each image is stored in sinus rhythm, while a five-beat clip is acquired in patients with irregular rhythm (usually atrial fibrillation). Measurements are not recorded immediately following an ectopic beat. When assessing regurgitation with colour flow Doppler, the Nyquist limit is set to 50–60 cm/s. For views of each valve, the colour gain is optimised until just before ‘speckling’ occurs.
In addition to standard acquisition protocols, the following images/measurements are obtained (corresponding views listed in brackets):
-
Zoomed images of the aortic valve, aortic root and ascending aorta, along with any regurgitation (parasternal long and short axis).
-
Diastolic function assessment (to include mitral valve inflow, pulmonary vein flow and pulsed wave (PW) tissue Doppler imaging (TDI) of the septal and lateral walls).
-
Tissue velocity imaging (TVI) 2D loop of left ventricle.
-
Continuous wave Doppler through aortic, mitral and tricuspid valves to demonstrate presence/absence of any regurgitation (apical five/four/three and two-chamber views, as appropriate).
Left ventricular ejection fraction is assessed using the Teichholz calculation if left ventricular systolic function is qualitatively normal, accompanied by experienced visual assessment of overall systolic function. In this setting, the Teichholz calculation performs well14—a recent study showed closer values than biplane ejection fraction assessed using the gold standard of cardiovascular magnetic resonance.15 Visual assessment, despite its semiqualitative nature, is also accurate when undertaken by experienced practitioners.16 ,17 Abnormal systolic function leads to a formal biplane volumetric assessment of ejection fraction, classified as follows: normal ≥60%, mildly impaired 45–59%, moderately impaired 35–44% and severely impaired <35%. A high threshold for normality was chosen to ensure that a large proportion of participants underwent volumetric assessment.
Diagnosis of VHD
Valve anatomy and physiology are assessed in accordance with BSE criteria for stenosis and regurgitation,18 which were adapted from internationally recognised guidelines.19 ,20 Aortic valve sclerosis is defined by the presence of all of the following echocardiographic features:
-
Focal areas of thickening and increased cusp echogenicity (calcification)—minor leaflet tip thickening in itself is insufficient and abnormal cusp echogenicity must be demonstrated.
-
Normal or near normal cusp mobility.
-
Maximum aortic valve transvalvular velocity less than or equal to 2.5 m/s.
These criteria are minor modifications of the European Association of Echocardiography/American Society for Echocardiography guidelines.20 A calcified or thickened aortic valve with transvalvular velocity greater than 2.5 m/s is diagnosed as aortic stenosis.
Extrapolating from the American Society of Echocardiography guidelines,19 we define mild (as opposed to trivial or ‘physiological’) valvular regurgitation if the regurgitant jet has a clear origin and is visible in more than one view on colour Doppler. Trivial mitral regurgitation requires the presence of normal mitral valve anatomy and a regurgitant jet that extends less than 1 cm into the left atrium at Nyquist limit 50–60 cm/s in all views.
Classification of newly diagnosed VHD
A low threshold for inclusion in the screen-positive group is specified in order to capture all manifestations of VHD and establish cohorts for future study. As a general rule, any left-sided valve disease (except ‘physiological’ regurgitation) is considered significant while isolated right-sided valve disease is only considered significant if moderate or greater in severity. A patient is referred for visit 2 assessment if any of the following conditions are identified:
-
Sclerotic aortic valve
-
Mild or above aortic stenosis or regurgitation
-
Mild or above mitral stenosis or regurgitation
-
Mild or above tricuspid or pulmonary stenosis
-
Moderate or above tricuspid or pulmonary regurgitation
Echocardiography—visit 2
An IE33 machine (Phillips, Eindhoven, The Netherlands) is used to obtain echo images at visit 2 by a sonographer blinded to the visit 1 findings. A replica dataset is obtained, with the addition of the following images (corresponding views):
-
Zoomed images of mitral valve (parasternal long and short axis)
-
TVI at mid-left ventricle (parasternal short axis)
-
Optimisation for Simpson's biplane volumetric assessment (apical four-chamber and two-chamber view)
-
Biplane left atrial volumes (X-plane through centre of mitral annulus)
-
PW TDI of inferoseptal and anterolateral walls (apical four-chamber view)
-
Three-dimensional (3D) datasets in those with adequate 2D images
For 3D dataset acquisition, a single cardiac cycle is constructed of four stitched cycles using images acquired with and without breath hold. The 3D datasets (and corresponding views) are as follows:
-
Three full volume loops focusing on mitral and aortic valves (parasternal long axis);
-
Three full volume loops focused on the left and right ventricle with mitral annulus still visible (apical four-chamber view);
-
Three full volume loops of 3D zoom over mitral valve, commissures and annulus (apical four-chamber view).
Image reporting and storage
The echocardiographic study is reported by the performing operator and stored using EchoPac V.110 (Vingmed-General Electric, Horton, Norway) with digital versatile disk backup. Strain analyses (whether 2D or 3D) will report the frame rate used in the final image analysis.
Quality assurance
Rolling review with blinded re-reporting of a random sample of approximately 15% of scans by the pool of BSE accredited sonographers and physicians is undertaken for quality assurance and to ensure consistency of reporting across sites. Reproducibility between the original assessment of VHD and that delivered by the group will be reported using Cohen's κ coefficient. When differences in reporting emerge, scans are reviewed by an independent blinded cardiologist.
Questionnaires
To explore associations between VHD and health status, all participants complete the Spielberger State-Trait Anxiety Index (STAI) and EQ-5D questionnaires during visit 1. In addition, a random sample of participants (approximately 10–20%) receives a postal version of the STAI and EQ-5D questionnaires at the point of study invitation and again 3 months after visit 1. There are natural comparisons to be made between our study, using as it does cardiac imaging in a primary care setting in participants without known heart valve disease, and a screening programme. We therefore assess the acceptability of echocardiographic screening for VHD in primary care using our own ‘Impressions of Screening’ questionnaire, which is completed during visit 1.
Spielberger State-Trait Anxiety Index
The STAI is a reliable and widely used measure of anxiety. We wished to examine how echocardiography affects our asymptomatic participants, and in particular whether the finding of mild VHD, which is usually clinically silent, causes them anxiety. We use the state scale, which focuses on short term as opposed to general feelings or traits, and the 6-item short form assessment, which has proven reliability and validity but offers a significant reduction in completion time compared with the original 40-item STAI questionnaire.21
Impressions of Screening questionnaire
We devised a short questionnaire which all participants complete immediately after their visit 1 echocardiogram to investigate general views concerning VHD screening. This was based on a questionnaire we had previously used to assess acceptability of faecal occult blood testing to detect colorectal carcinoma.22
EQ-5D questionnaire
The EQ-5D assesses self-described health status across a number of domains that is then condensed into a single index.23 It has been widely used and extensively validated across different populations and disease states.24 We elected to use the EQ-5D without visual analogue scale.
Blood tests and genetic profiling
Visit 2 participants undergo venepuncture and approximately 20 mL blood is divided into separate tubes containing EDTA, heparin and serum-separating tubes (Becton Dickinson, Franklin Lakes, New Jersey, USA). These are refrigerated immediately and centrifuged within 2 h at 1300 rpm for 10 min at 4°C. The plasma/serum fraction is removed and stored in 500 μL aliquots. Whole blood stored on EDTA is refrigerated at 4°C until DNA extraction is performed within 5 days of sample collection. DNA is extracted using the QIAamp DNA blood Midi kit (Qiagen, Venlo, The Netherlands) according to the manufacturer's instructions and, along with the remaining samples, is stored for future analysis at −80° C with Oxford Radcliffe Biobank. Separate EDTA plasma samples are collected for B-type natriuretic peptide (BNP) analysis and these are frozen prior to analysis for up to 3 days following centrifugation and separation. BNP analyses utilise the Siemens ADVIA Centaur analyser (Siemens Healthcare Diagnostics, Frimley, UK) in accordance with manufacturer’s recommendations. Sample registration and tracking are collated using Sapphire V.5.1 (LabVantage, Somerset, New Jersey, USA).
Bias
A brief questionnaire identifying reasons for non-participation is sent to those declining the invitation, allowing us to examine potential bias owing to differences between participants and non-participants. Once results are collated, we will report the final study uptake and provide comparisons of those accepting and declining the invitation to participate.
Diagnosis of VHD using echocardiography may also introduce bias since this modality has limitations in image acquisition, particularly in participants with obesity or significant lung disease. Given the association between these conditions and cardiovascular disease, this may lead to underestimation of the prevalence of VHD.
Study size
We aim to invite 5000 individuals from the Oxfordshire population to participate in OxVALVE-PCS. Based on previous experience in community heart failure screening programmes, it is expected that approximately 4000 (80%) will participate. The threshold for inclusion in the screen-positive group is low to allow all manifestations of VHD to be captured with subsequent careful prospective follow-up. Based on a detection rate of 30%, this total of 4000 participants will identify approximately 1200 cases of newly diagnosed VHD. However, most of the VHD detected will be mild. In the meta-analysis by Nkomo et al,1 moderate-to-severe VHD was detected in 1.3% of those aged 65–74 years. Our sample size of 4000 participants was therefore chosen to detect at least 50–60 participants with moderate-to-severe VHD.
Quantitative variables and statistical methods
We describe methods of statistical analysis for the primary outcome—secondary outcome analyses will be conducted in a similar way. Participants with missing key data (in particular, measurement of ejection fraction, left ventricular, left atrial and interventricular septal dimensions) will be removed from the analysis. Descriptive statistics will be presented using means and SDs for continuous variables and counts (percentages) for categorical variables. t Test and χ2 test will be used to explore associations between VHD and quantitative and categorical variables, respectively. Trends across age groups will be examined using the Cochran-Armitage test, and logistic regression models will be used to test the association of VHD (as previously defined) with clinical and echocardiographic characteristics. Initial regression models will be unadjusted, and then adjustments made for potential confounders such as age, sex, BMI, study centre, clinical variables and socioeconomic status. All results from the regression analysis will be expressed as ORs with 95% CIs and a two-tailed p value <0.05 considered statistically significant.
Ethics and dissemination
Research sponsorship is provided by the Oxford Radcliffe Hospitals NHS Trust (precursor to Oxford University Hospitals Trust, Research and Development Reference 5942).
The results of the study will be submitted for publication in peer-reviewed scientific journals. We will also provide summaries of findings in a more accessible format through a newsletter to our participants and on our website (http://www.oxvalve.nhs.uk).
Discussion
OxVALVE-PCS is the first population-based prospective cohort study focusing primarily on investigating the epidemiology of VHD in the elderly. The study also assesses the impact of echocardiographic screening for occult VHD and other cardiovascular disease in primary care for the first time, allowing earliest detection of not only VHD but also other key cardiac conditions (eg, latent left ventricular systolic dysfunction). Participants with previously unidentified VHD may benefit from detailed follow-up and participation in future research studies of novel therapies. In anticipation of the increasing prevalence of VHD in the growing elderly population, the study will also direct healthcare policy and financial planning by accurate delineation of the contemporary epidemiology of VHD in a European nation.
Limitations
OxVALVE-PCS will underestimate the overall prevalence of VHD as a result of (1) limited echocardiographic imaging in some participants, (2) exclusion of the very frail elderly and (3) exclusion of those with known VHD.
Assessment of a healthy asymptomatic population sample and exclusion of participants with known VHD will systematically underestimate overall prevalence. The use of echocardiography has risen steadily over the years, with an average of 1.1 echocardiograms performed per person per year in a recent US-based Veterans Health Association study.25 Participants with comorbidities predisposing to VHD, especially ischaemic heart disease, are likely to have had an echocardiogram based on current recommendations.26 Any incidental (even mild) VHD would exclude a participant from our study, leaving our sample potentially consisting of participants with a lower range of comorbidity than the general population. For example, pre-existing bicuspid aortic valve disease is likely to present clinically in participants less than 65 years of age—our study design will therefore systematically underestimate its prevalence in the overall population. However, since one of our aims is to determine the prevalence of newly diagnosed VHD, our approach is integral to the study with the large sample size still allowing us to detect a significant number of new cases of VHD. Amalgamation of the prevalence of known and newly diagnosed VHD will be carried out at the time of final data analysis using pre-existing primary and secondary care databases.
The epidemiology of VHD in frail elderly adults was investigated in early echocardiographic studies conducted among participants in long-term residential care.27–29 Frail elderly participants are often unable or unwilling to tolerate medical or surgical therapies—intervention earlier in the course of the disease, before the onset of frailty is more acceptable and less risky. OxVALVE-PCS was designed pragmatically in conjunction with primary care colleagues and aims to provide epidemiological information on a population where VHD may be more amenable to intervention in the future. Although exclusion of the very frail elderly reduces the overall number of participants with VHD, the large sample size provides the study power required to accurately delineate different subpopulations of VHD.
We also recognise that our study population may not be representative of other areas of the UK, Europe and beyond. Consistent with local census data, 98% of the population sampled by OxVALVE-PCS is of white ethnicity, compared with, for example, 86% of the elderly US population.30 Clearly, the prevalence of VHD may vary in areas with greater ethnic mix where previous exposure to such diseases as rheumatic fever may be a major confounding variable. Socioeconomic factors may also bear influence on the prevalence of VHD, and this will be the subject of further investigation. However, the characteristics of the OxVALVE-PCS population are not dissimilar to those of the total population of England and Wales, where 95% of the elderly are of white ethnicity—despite increasing heterogeneity in younger age groups, older age groups in many high-income countries remain largely ethnically homogenous.12 Our findings are therefore germane to other similar populations.
Conclusions
OxVALVE-PCS is a large population-based prospective study that will provide important new insight into the epidemiology of VHD. Cardiac services are under pressure to deal cost-effectively with ‘the new cardiac epidemic’.31 The study will therefore be important in providing clinicians and health service planners with the evidence necessary to plan for the future.
Acknowledgments
This article has been submitted on behalf of the OxVALVE-PCS group. The authors would like to thank the coinvestigators: Richard Hobbs, Peter Grimwade, David Ebbs, Harald Becher, Louise Locock; statistical support: Abdelouahid Tajar, Jacqueline Birks; echocardiographers: Linda Arnold, Cassandra Hammond, Claire Mabbett, Nadia Pinheiro, Rebecca Reynolds, Claudio Eduardo Lima; administration: Andrew Kennedy, Hema Collappen, Lee Potiphar, Sabrina Harris, Jo Wilson.
References
Footnotes
-
Contributors The original study was designed by JLdA, DM, AJF and BDP. The protocol was written by SC and MAL, with input from the other authors. All authors reviewed and approved the final draft.
-
Funding The study is supported by the National Institute of Health Research (NIHR) Thames Valley Comprehensive Local Research Network (UKCRN ID 6086) and the NIHR Oxford Biomedical Research Centre Programme, with initial support coming from the NIHR School for Primary Care Research.
-
Competing interests None.
-
Ethics approval The study was granted ethical approval by the local research ethics committee (Southampton, UK; REC Ref: 09/H0502/58).
-
Provenance and peer review Not commissioned; externally peer reviewed.