Article Text

Abstract
Objective To ascertain whether different oral P2Y12 inhibitors might affect rates of acute stent thrombosis and 30-day outcomes after primary percutaneous coronary intervention (pPCI).
Methods The European Ambulance Acute Coronary Syndrome Angiography (EUROMAX) randomised trial compared prehospital bivalirudin with heparin with optional glycoprotein IIb/IIIa inhibitor treatment in patients with ST-segment elevation myocardial infarction triaged to pPCI. Choice of P2Y12 inhibitor was at the investigator’s discretion. In a prespecified analysis, we compared event rates with clopidogrel and newer oral P2Y12 inhibitors (prasugrel, ticagrelor). Rates of the primary outcome (acute stent thrombosis) were examined as a function of the P2Y12 inhibitor used for loading and 30-day outcomes (including major adverse cardiac events) as a function of the P2Y12 inhibitor used for maintenance therapy. Logistic regression was used to adjust for differences in baseline characteristics.
Results Prasugrel or ticagrelor was given as the loading P2Y12 inhibitor in 49% of 2198 patients and as a maintenance therapy in 59%. No differences were observed in rates of acute stent thrombosis for clopidogrel versus newer P2Y12 inhibitors (adjusted OR 0.50, 95% CI 0.13 to 1.85). After adjustment, no difference was observed in 30-day outcomes according to maintenance therapy except for protocol major (p=0.029) or minor (p=0.025) bleeding and Thrombolysis In Myocardial Infarction minor bleeding (p=0.002), which were less frequent in patients on clopidogrel. Consistent results were observed in the bivalirudin and heparin arms.
Conclusions The choice of prasugrel or ticagrelor over clopidogrel was not associated with differences in acute stent thrombosis or 30-day ischaemic outcomes after pPCI.
Trial registration number NCT01087723.
- bivalirudin
- stent thrombosis
- clopidogrel
- prasugrel
- ticagrelor
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Large randomised studies have associated prasugrel and ticagrelor with a reduction in ischaemic events versus clopidogrel in patients with acute coronary syndrome at long-term follow-up.
What does this study add?
We found no significant differences in acute stent thrombosis between patients with ST-segment elevation myocardial infarction (STEMI) given prasugrel or ticagrelor versus clopidogrel.
How might this impact on clinical practice?
Optimal antithrombotic strategies need to be developed to improve short-term outcome in patients with STEMI.
Introduction
A rapid and powerful platelet inhibition appears key in patients with ST-segment elevation myocardial infarction (STEMI) referred for primary percutaneous coronary intervention (pPCI). In pivotal trials,1 2 the use of prasugrel or ticagrelor versus clopidogrel was associated with a reduction in the rate of ischaemic events. While the overall rate of stent thrombosis was reduced with prasugrel or ticagrelor in the overall population1 2 as well as in the subgroup of patients with STEMI treated with pPCI,3 4 there was no difference in rates of acute stent thrombosis.5 6 Recent studies have provided a rationale for this observation, showing that the onset of antiplatelet effect with P2Y12 inhibitors such as prasugrel and ticagrelor can be delayed in STEMI compared with that in stable patients or healthy volunteers.7–10
The European Ambulance Acute Coronary Syndrome Angiography (EUROMAX) trial11 compared prehospital bivalirudin with heparin (unfractionated heparin [UFH] or low-molecular-weight heparin) with/without glycoprotein IIb/IIIa inhibitor treatment and found a significant reduction in death or major bleeding with bivalirudin. EUROMAX also confirmed an observation from the HORIZONS-AMI trial12 of an increased risk of acute stent thrombosis of approximately 1% in absolute terms, which appeared confined to the 4 hours after the end of PCI.13
We aimed to investigate whether use of prasugrel or ticagrelor, versus clopidogrel, was associated with a reduction in the rate of acute stent thrombosis and whether either of the newer P2Y12 inhibitors improved 30-day clinical outcomes, in the overall trial population and as a function of treatment.
Methods
Design and participants
The EUROMAX trial enrolled patients who presented within 12 hours of symptom onset with a presumed diagnosis of STEMI and undergoing pPCI (ClinicalTrials.gov registry, NCT01087723).11 The study complied with the Declaration of Helsinki. The protocol was approved by local ethics committees and health authorities. Patients provided written informed consent.
Treatments
All patients received aspirin and an approved oral P2Y12 inhibitor (clopidogrel, prasugrel, ticagrelor) as early as possible after first medical contact. Decisions regarding the choice of P2Y12 inhibitor, clopidogrel loading dose (300 or 600 mg) and other procedural options were left to physician preferences and local practices. Patients were randomised to bivalirudin or UFH/low-molecular-weight heparin with or without a glycoprotein IIb/IIIa inhibitor (per investigator usual practice and guidelines).
Patients in the bivalirudin arm received a bolus of 0.75 mg/kg followed by an infusion of 1.75 mg/kg/hour. The protocol specified that the infusion could be continued for ≥4 hours after PCI at a dose of 0.25 mg/kg/hour; however, continuation of the PCI dose (1.75 mg/kg/hour) was permitted.
Outcomes
Patients were followed to 30 days. The primary end point of this analysis was the occurrence of acute stent thrombosis as a function of the P2Y12 inhibitor used for the loading dose (ie, ticagrelor or prasugrel vs clopidogrel). Acute stent thrombosis was defined according to the Academic Research Consortium (ARC) definition as a stent thrombosis occurring <24 hours after the index PCI.14 Multiple secondary outcomes were analysed at 30 days, all of which were end points of the EUROMAX trial.11
In the EUROMAX trial, the primary outcome was the composite of all-cause death or protocol major bleeding not related to coronary artery bypass graft (CABG) surgery at 30 days. The key secondary 30-day outcome was a composite of all-cause death, myocardial re-infarction or non-CABG major bleeding. Other prespecified secondary outcomes included major adverse cardiovascular events (MACE; a composite of death, re-infarction, ischaemia-driven revascularisation or stroke), net adverse clinical events (NACE, a composite of MACE and non-CABG major bleeding), each of the components of the primary and principle secondary outcomes, ischaemia-driven revascularisation, major and minor bleeding, and ARC-defined stent thrombosis.14
Protocol-defined major bleeding was defined as bleeding unrelated to CABG surgery that included intracranial, retroperitoneal or intraocular bleeding; access-site haemorrhage requiring radiological or surgical intervention; a reduction in the haemoglobin concentration of >4 g/dL (2.5 mmol/L) without an overt source of bleeding; a reduction in the haemoglobin concentration of 3 g/dL (1.8 mmol/L) with an overt source of bleeding; re-intervention for bleeding; or use of any blood-product transfusion. Access-site haematomas, which did not require surgical or radiological intervention, were not counted as major bleeds regardless of their size. Protocol minor bleeding was defined as all other non-CABG-related bleeding or transfusion events. Bleeding events were also classified according to the Thrombolysis In Myocardial Infarction (TIMI) criteria.15
Statistical analysis
A prespecified comparison of outcomes as a function of oral P2Y12 inhibitor used (prasugrel or ticagrelor vs clopidogrel) was performed. Analyses were performed in the intent-to-treat population. The χ2 test or Fisher’s exact test was used for comparisons of event rates. The log-rank test was used to compute the significance of time-to-event data. Continuous variables are reported as medians (IQRs). The Wilcoxon rank-sum test was used to compare continuous variables. A p value of <0.05 was considered significant. Categorical variables are reported as frequencies and percentages. Rates of acute stent thrombosis were examined as a function of the P2Y12 inhibitor used for loading, and 30-day outcomes were examined as a function of the P2Y12 inhibitor used for maintenance therapy. To account for differences in baseline characteristics in this postrandomisation subgroup analysis, a logistic regression analysis was performed. Variables in the logistic regression model included age >65 years, female sex, anaemia, hypertension, hyperlipidaemia, diabetes, smoking, creatinine clearance ≤60 mL/min, prasugrel/ticagrelor versus clopidogrel, history of myocardial infarction, previous CABG, previous PCI, Killip class ≥II, access site (femoral vs radial), pre-PCI TIMI flow 0 or 1, single-vessel disease, placement of a drug-eluting stent, and treatment with bivalirudin versus standard of care. Analyses were performed with the use of SAS software, V.9.2.
Results
Population
Of the 2198 patients triaged to pPCI in the EUROMAX trial, 2104 (95.7%) received an oral P2Y12 inhibitor loading dose (90.9% received the loading dose before angiography). Clopidogrel was used for loading in 1069 patients, prasugrel in 629 patients and ticagrelor in 406 patients. P2Y12 inhibitor maintenance therapy after the procedure was used in 1927 patients (87.7%). Eight of these received ticlopidine and were excluded, leaving a population of 1919 patients. Figure 1 details the numbers of patients with data who received loading and maintenance doses for each drug.

Flow chart. The numerical differences between loading and maintenance dose totals are due to missing data.
Baseline characteristics
Patient and procedural characteristics according to P2Y12 inhibitor loading are shown in table 1. Patients given clopidogrel for the loading dose were older, more likely to be female, to have a history of myocardial infarction and to have had a failed procedure. In contrast, they were less likely to present with congestive heart failure and to have the procedure done by the radial approach. The type of P2Y12 inhibitor used for the loading dose was highly dependent on the country in which the patient was randomised. Patients who had a clopidogrel loading dose were more likely than those on prasugrel or ticagrelor to receive it before the angiogram was performed. Median delays between loading dose and angiogram were 50 min (IQR 35 to 66) in the overall population, 48 min (IQR 30 to 65) in patients who received newer P2Y12 inhibitors as loading dose and 51 min (IQR 38 to 67) in patients who received clopidogrel as loading dose.
Patient and procedural characteristics according to loading P2Y12 inhibitor
Patients on clopidogrel maintenance therapy showed features indicative of higher cardiovascular risk, with an older age, higher prevalence of major risk factors and history of myocardial infarction, higher Killip class and kidney dysfunction (see supplementary table S1). In addition, the rate of pre-PCI TIMI 3 flow was lower for patients receiving clopidogrel; they also had PCI less frequently performed and more frequently had a procedural failure.
Supplementary file 1
Acute stent thrombosis according to loading P2Y12 inhibitor
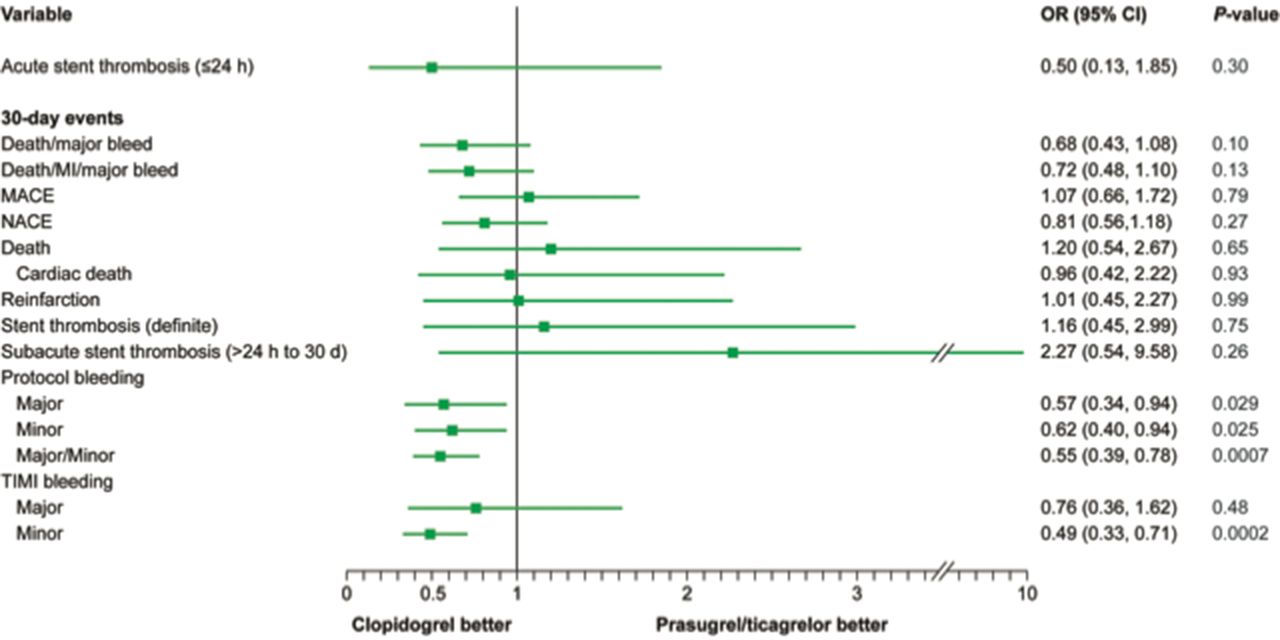
The rate of acute stent thrombosis did not differ according to the P2Y12 used for the loading dose: eight patients (0.8%) with prasugrel or ticagrelor versus five patients (0.5%) with clopidogrel (p=0.37). One additional case of stent thrombosis was excluded from the analysis due to missing data on the loading dose. After adjustment, no difference was observed (adjusted OR 0.50, 95% CI 0.13 to 1.85, p=0.30, figure 2).

{kind=link}
{kind=link}
Adjusted* ORs for outcomes by maintenance P2Y12 treatment. *Adjusted for age>65 years, anaemia, bivalirudin versus heparin±glycoprotein IIb/IIIa inhibitor, new P2Y12 maintenance dose, creatinine clearance ≤60 vs >60 mL/min, current smoker, diabetes, drug-eluting stent, female sex, femoral versus radial access, hyperlipidaemia, hypertension, Killip class≥II, preprocedural TIMI flow 0/1 vs 2/3, history of coronary artery bypass graft, previous percutaneous coronary intervention, previous MI, single-vessel disease. MACE, major adverse cardiac events (death or myocardial infarction, ischaemia-driven revascularisation or stroke); MI, myocardial infarction; NACE, net adverse clinical events (death or myocardial infarction, ischaemia-driven revascularisation, stroke or bleeding); TIMI, Thrombolysis In Myocardial Infarction.
Thirty-day outcomes according to P2Y12 used for maintenance dose
There was no association between the type of P2Y12 inhibitor used for the maintenance dose and rates of the 30-day endpoints (table 2). The rate of death was lower (1.3% vs 2.7%; p=0.03), and minor bleeds were higher in patients on prasugrel or ticagrelor (table 2). The rate of stent thrombosis was similar across subsets defined according to type of P2Y12 inhibitor.
Unadjusted outcomes by P2Y12 inhibitor
After adjustment, there was no significant difference in clinical outcomes between groups except for lower rates of protocol major bleeding (p=0.029) and minor bleeding (p=0.025), as well as TIMI minor bleeding (p=0.0002) with clopidogrel (figure 2).
Effect of P2Y12 type according to treatment arm (bivalirudin vs heparin with optional glycoprotein IIb/IIIa)
Information on the loading and maintenance P2Y12 inhibitors used in the bivalirudin and heparin (with optional glycoprotein IIb/IIIa inhibitor) treatment arms is detailed in supplementary table S2.
Overall, the benefits of bivalirudin over heparin with optional glycoprotein IIb/IIIa inhibitor treatment were consistent across subgroups defined by the use of prasugrel/ticagrelor or clopidogrel, with no statistical interaction between these subgroups (table 2). In particular, the interaction for acute stent thrombosis according to loading dose was not significant (p=0.74).
Discussion
In this prespecified analysis from the EUROMAX trial, we observed that use of the newer oral P2Y12 inhibitors, prasugrel or ticagrelor, was not associated with a lower rate of acute stent thrombosis or 30-day ischaemic outcomes as compared with the use of clopidogrel.
Rapid and potent platelet inhibition is key in order to reduce the risk of ischaemic complications in patients with STEMI. As a consequence, current guidelines recommend the early use of P2Y12 inhibitors.16 17 However, whereas the European Society of Cardiology guidelines16 recommend using prasugrel or ticagrelor over clopidogrel, the American College of Cardiology/American Heart Association guidelines17 stipulate the same level of recommendation for all three.
The absence of a difference in the rate of acute stent thrombosis according to the oral P2Y12 inhibitor used for the loading dose in our analysis is consistent with the existing literature. In the PLATO trial, the rate of acute stent thrombosis was not significantly different in patients on ticagrelor versus those on clopidogrel.5 In the ATLANTIC trial, prehospital administration of ticagrelor did not improve pre-PCI coronary reperfusion. However, the rates of definite stent thrombosis were lower in the prehospital group, which can be interpreted as indicating that earlier administration may counteract a delayed onset of action of this agent in patients with STEMI18 as the action of P2Y12 inhibitors is delayed due to a slower gastrointestinal absorption compared with that in healthy controls.7–10 This delay may be due to several factors, including the action of morphine or morphine derivatives, which are frequently used prehospital or intrahospital to relieve pain in patients with STEMI10 18 19 and haemodynamic dysfunction in patients with shock or preshock.20
The lack of a difference in 30-day outcomes according to the P2Y12 inhibitor used as maintenance treatment in our study appears somewhat at variance with the results of the TRITON and PLATO trials, both of which demonstrated a significant reduction in the rate of ischaemic events in the overall population as well as in the group with STEMI.1 2 However, the present analysis is underpowered since EUROMAX was much a smaller trial than TRITON or PLATO, and we analysed 30 day rather than 1-year outcomes.
As detailed in figure 1, a substantial proportion of patients had a switch of P2Y12 inhibitor between loading and maintenance doses. This is probably because the loading dose was administered in a prehospital setting for most patients, while the maintenance dose was given in hospital. Hospital and prehospital antiplatelet protocols might differ as they are usually managed by different teams. This might be a confounding factor when analysing 30-day outcomes.
The use of bivalirudin for pPCI has been associated with an increase in the risk of acute stent thrombosis.11 12 In the HEAT-PPCI trial, despite the fact that newer oral P2Y12 inhibitors were used in >90% of cases, an increase in both early stent thrombosis and other ischaemic events was observed.21 Those results are consistent with our observations. The mechanism of bivalirudin-associated acute stent thrombosis is probably associated with a rapid clearance of the drug after discontinuation of the drug, resulting in an insufficient thrombin inhibition in the first hours following stent implantation and prior to the effectiveness of oral antiplatelet agents. Therefore, there is a ‘gap’ in antithrombotic protection.8 9 22 Whether this risk could be addressed by an intravenous antiplatelet agent with faster onset of action, for example, cangrelor, remains to be demonstrated.23–25 In contrast, several analyses tend to demonstrate that potent post-PCI thrombin inhibition decreases the risk of acute stent thrombosis. In the BRIGHT trial,26 in a subgroup analysis from EUROMAX27 and in an exploratory analysis of the MATRIX trial,28patients who received a prolonged infusion of bivalirudin at the full dose of 1.75 mg/kg/hour after PCI had no excess risk of acute stent thrombosis.
Limitations
These data were derived from a prespecified analysis of postrandomisation data. Thus, the decision to use clopidogrel or one of the newer P2Y12 inhibitors was left to the discretion of the investigators and confounding cannot be excluded. In addition, there were major differences in the geographical distribution and the baseline clinical characteristics as a function of the agent used, some of which can affect the risk of ischaemic or bleeding complications. Even if we performed multivariable adjustments, our results may be partially due to residual confounding. The low number of events and the large CI observed in the comparison of stent thrombosis between the two groups makes a statistical type 2 error possible. This result should therefore be interpreted with caution. The fact that most patients received pretreatment with P2Y12 inhibitors might have attenuated differences in platelet inhibition between the two groups. However, precise information on the timing of the administration of the loading dose is not available. The relatively low numbers of patients receiving each of the two newer P2Y12 agents and low number of stent thromboses prevent a sound comparison between prasugrel and ticagrelor. This comparison is currently being done in a randomised trial (ISAR-REACT 5 trial NCT01944800). Finally, EUROMAX was an open-label trial. However, a central adjudication committee blinded to treatment allocation reviewed all events.
Conclusions
The rate of acute stent thrombosis did not differ between patients who received a loading dose of prasugrel or ticagrelor and those who received clopidogrel. Following adjustment, 30-day outcomes were similar between patients receiving prasugrel or ticagrelor and those receiving clopidogrel for the maintenance dose, with the exception of an increased risk of bleeding events with the newer agents. These results were consistent regardless of the anticoagulation strategy used.
Acknowledgments
Sophie Rushton-Smith (MedLink Healthcare Communications Limited) provided editorial assistance with editing and formatting and was funded by INSERM U1148.
References
Footnotes
KH and GD contributed equally.
Contributors Conceived and designed the research: KH, GD, PGS. Performed statistical analysis: DB, JP. Handled funding and supervision: PGS, KH, GD, END. Acquired the data: KH, GD, CWH, AVH, FL, PCl, GG, JS, FWV, JA, LN, VK, PCo, UZ. Drafted the manuscript: GD, KH, PGS. Made critical revision of the manuscript for key intellectual content: all authors.
Funding This work was supported by The Medicines Company, Parsippany, New Jersey, USA.
Competing interests KH has received personal fees from Daiichi Sankyo, Eli Lilly and The Medicines Company and personal fees and grants from AstraZeneca. GD has received personal fees from AstraZeneca, Biotronik, Bristol-Myers Squibb, Daiichi Sankyo and Eli Lilly. CWH has received personal fees from AstraZeneca, Eli Lilly and Sanofi-Aventis. AH has received grants from Daiichi Sankyo, Iroko and Medtronic. FL has received personal fees from AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Correvio, Eli Lilly, Merck-Serono and The Medicines Company. PCo has received personal fees from The Medicines Company and grants from Daiichi Sankyo. GG has no disclosure to report. JS has received personal fees and grants from The Medicines Company. FWAV has received personal fees from AstraZeneca, Boehringer Ingelheim and Eli Lilly. JA has no disclosures to report. LN has received personal fees from Boehringer Ingelheim Pharma GmbH&Co. KG and The Medicines Company. VK has received personal fees from AstraZeneca and Boston Scientific. PCl has received personal fees from Bayer, Boehringer Ingelheim and Bristol-Myers Squibb and personal fees and grants from AstraZeneca, Daiichi Sanko, Eli Lilly, Medtronic, Pfizer, Sanofi and The Medicines Company. UZ has received personal fees from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Merck Sharpe & Dohme, Novartis, Pfizer and Sanofi. DB has received personal fees from The Medicines Company. JP has received personal fees from The Medicines Company. END was an employee of The Medicines Company at the time of the analysis and remains a shareholder. PGS has received personal fees from Amarin, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, CSL Behring, Daiichi Sankyo, Eli Lilly, GlaxoSmithKline, Janssen, Medtronic, Merck Sharpe & Dohme, Novartis, Pfizer, Regeneron and Roche, personal fees and grants from Sanofi and Servier, and personal fees and non-financial support from The Medicines Company.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Local ethics committees and health authorities.
Provenance and peer review Not commissioned; externally peer reviewed.