Article Text

Abstract
Objective To establish which risk factors are predictive for sudden death in hypertrophic cardiomyopathy (HCM) diagnosed in childhood.
Methods A Swedish national cohort of patients with HCM diagnosed <19 years of age was collected between 1972 and 2014, consisting of 155 patients with available ECGs, with average follow-up of 10.9±(SD 9.0) years, out of whom 32 had suffered sudden death or cardiac arrest (SD/CA group). Previously proposed risk factors and clinical features, ECG and ultrasound measures were compared between SD/CA group and patients surviving >2 years (n=100), and features significantly more common in SD/CA group were further analysed with univariate and multivariate Cox hazard regression in the total cohort.
Results Ranked according to relative risk (RR) the ECG risk score >5 points had an RR of 46.5 (95% CI 6.6 to 331), sensitivity of 97% (83% to 100%) and specificity of 80% (71% to 88%) (p<0.0001), and was the best ECG predictor, predicting a 5-year risk of SD/CA of 30.6%. The following are other features with importantly raised RR: Detroit wall thickness Z-score >4.5: 9.9 (3.1 to 31.2); septal thickness ≥190% of upper limit of normal for age (septum in % of 95th centile for age (SEPPER) ≥190%): 7.9 (3.2 to 19.4); ventricular tachycardia: 9.1 (3.6 to 22.8); ventricular ectopics on exercise testing: 7.4 (2.7 to 20.2); and left ventricular outflow gradient (left ventricular outflow tract obstruction (LVOTO)) >50 mm Hg: 6.6 (4.0 to 11.0). Family history was non-significant. Multivariate Cox hazard analysis gives the following as early predictors: limb-lead QRS amplitude sum (p=0.020), SEPPER ≥190% (p<0.001) and LVOTO at rest (p=0.054); and for late predictors: last ECG risk score (p=0.002) and last Detroit Z-score (p=0.001). Both early (p=0.028) and late (p=0.037) beta-blocker doses reduced risk in the models.
Conclusions ECG phenotype as assessed by ECG risk score is important for risk of sudden death and should be considered for inclusion in risk stratification of paediatric patients with HCM.
- sudden cardiac death
- paediatric arrythmias
- risk factors
- electrocardiography
- cardiomyopathy hypertrophic
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Most predictors used for risk stratification for sudden death in adults with hypertrophic cardiomyopathy (HCM) have failed to emerge as significant risk factors for sudden death in childhood HCM, with the exception of ventricular tachycardia on a 24-hour Holter ECG. The risk of sudden death in patients with HCM is higher in the 8–16 years old age range than among the 17–30 years old age range.
What does this study add?
This study is the first to show that the ECG phenotype as quantified by the ECG risk score is a powerful and independent predictor of risk of sudden death in childhood HCM, and also proposes a different Z-score cut-off for maximum wall thickness than that used in previous paediatric studies. Phenotypic factors are more important determinants of risk in childhood HCM than family history.
How might this impact on clinical practice?
Risk stratification for consideration of primary prophylactic internal cardiac defibrillator implantation could be improved by incorporating the ECG risk score, where a risk score >5 points predicts a 5-year risk of SD/CA of 30.6% in the population studied. The ECG risk score could easily be programmed to be calculated automatically by digital ECG machines and should be formally assessed in other paediatric populations. A separate paediatric risk algorithm for patients with HCM needs to be developed from observations solely on paediatric patients.
Introduction
Hypertrophic cardiomyopathy (HCM) accounts for a large proportion of cases of childhood cardiomyopathy.1 2 Sudden death due to arrhythmia, which at 0.112 deaths per 100 000 age-specific population has a significantly higher rate in patients with HCM aged 8–16 years old than in the 17–30 years old age range,3 is the most common autopsy-proven cause of sudden death in children after infancy in Sweden and Japan.3 4 HCM was also reported as the most common cause of sudden death in athletes, with a mean age at sudden death of 17±3 years,5 although neither of the above studies looked for channelopathies with molecular autopsy. The implantation of an internal cardiac defibrillator (ICD) offers an approach to protection of high-risk individuals,6 but the procedure has significant morbidity, and even mortality,7 and is associated with serious psychological sequelae in 43% of children and young adults.8 Current approaches to risk stratification recommended by the American Heart Association9 and the European Society of Cardiology (ESC)10 differ somewhat but are based on research findings in populations of adult patients with HCM.11 Studies from paediatric cardiology centres have failed to reproduce a significant role in childhood HCM for most of the risk factors used for adult patients with HCM,12–15 with the exception of the presence of non-sustained ventricular tachycardia (nsVT),12 14 15 although they have been handicapped by a low statistical power due to few (n=7–22) endpoints reached. A limb-lead QRS amplitude sum (LLQRSS) >10 mV has been shown to be an independent risk factor for sudden cardiac death in childhood HCM.16 More recently, an ECG risk score including both morphological features and voltage-amplitude criteria, which are a powerful predictor for sudden death or cardiac arrest in adult patients with HCM, has been described.17 The current study uses a large national paediatric HCM cohort collected over more than 40 years to compare previously proposed risk factors as well as the new ECG risk score in their ability to predict risk of subsequent sudden death/cardiac arrest (SD/CA) in childhood HCM.
Methods
Study patients
A national cohort of Swedish paediatric patients with HCM diagnosed <19 years of age was assembled as described previously16 18 between 1972 and October 2014 (details in online supplementary methods). A comparison of pre-1999 and post-1999 patients are shown in online supplementary table S1. With more emphasis on systematic family screening after the multicentre study published in 1999,18 the more recent cohort comprises a greater proportion of slightly older children with familial and milder disease. The total cohort comprised 162 patients with a minimum of 2 years of follow-up in survivors, and an average follow-up of 10.9±(SD 9.0) years; a total of 39 patients had suffered sudden death or resuscitated cardiac arrest (30 sudden deaths, including 12 with sudden death as first disease manifestation, plus 6 resuscitated cardiac arrests and 3 appropriate ICD interventions), together termed the SD/CA group. The 12 presenting with sudden death did not differ significantly in clinical characteristics from sudden deaths during follow-up, although a slightly higher proportion were male (85% as compared with 62% for those with SD/CA on follow-up, p=0.27). In the total cohort 48% had a family history of HCM, and 23% were associated with a Noonan spectrum syndrome. A total of 155 patients (with 32 SD/CA) had available ECGs and were used in the assessments of relative risk of different ECG features. One hundred and forty patients in the cohort have both ECG and wall thickness measurements, out of whom 27 had suffered either SD/CA (n=24) or an appropriate ICD shock (n=3) (SD/CA group). Those 140 were used for the univariate and multivariate Cox hazard analyses.
Supplementary file
Primary endpoint
The primary endpoint was sudden cardiac death/cardiac arrest/appropriate ICD intervention (SD/CA).
Clinical measures collected
All ECGs had voltages measured from entry ECG and latest follow-up ECG by one investigator who was the registry holder (IÖ-S) for entry into a national registry, 1990–1999 retrospectively, when many of the patients who subsequently died suddenly were still alive,18 and from 2000 prospectively, as part of studies originally focusing on treatment effects.16 18 The ECG risk score was recently calculated from those previously entered measurements as described17 (method in online supplementary table S2). Since the ECG risk score was not published until 2010, and 87% of survivor ECG measurements and 84% of SD/CA ECG measurements were entered into the registry before 2010, bias could not have occurred. From 2000 virtually all ECGs were digitally recorded allowing automatic calculation of QRS duration, QTc, voltages and ST-T wave deviations by the ECG machine to be used, so reproducibility is excellent. For digital ECGs previously having ECG risk score calculated by other physicians, there have been no disagreements on risk score points. Original M-mode and two-dimensional ultrasound measurements were remeasured where available (IÖ-S and EF); otherwise reports in hospital notes were accepted. Detroit Z-scores for maximum wall thickness were calculated using the Cardio Z app,19 and septal thickness related to upper limit of normal for age (septum in % of 95th centile for age (SEPPER)) according to the published formula.18 A left ventricular outflow tract (LVOT) gradient >20 mm Hg at rest was considered significant obstruction (LVOTO).13 Presence of obvious systolic anterior movement of mitral valve apparatus plus a systolic murmur was judged evidence of LVOTO in an era before Doppler measurements were available. Hospital records were scrutinised for information about syncope and family history of sudden death below the age of 40 years, 24-hour Holter and exercise test results. Latest ultrasound and ECG measures recorded were retrieved from the hospital records, even for those patients who had entered adult cardiology follow-up, and in the majority last follow-up measurements are obtained within 1–2 years of the endpoint. Medical treatments and interventional procedures have been documented. Of the patients, 62.4% received beta-blocker therapy (largely propranolol or metoprolol, only 2% received atenolol), 8.6% calcium-blocker therapy and 4.3% amiodarone. Of the patients, 24.0% received a combination of disopyramide and high-dose beta-blocker. Beta-blocker doses used were converted to propranolol equivalents using the conversion propranolol 80 mg=metoprolol 100 mg20=bisoprolol 5 mg=atenolol 50 mg.
Causes of death
All Swedes have a unique personal identification number, and vital status was last ascertained on 6 October 2016. Where causes of death were not recorded in hospital notes, they were obtained from death certificates from the National Board of Health and Welfare. Apart from the 39 classed as SD/CA group, there were 17 additional cardiac deaths. No patient was lost to follow-up.
Statistics
Statistical analyses are described in detail in online supplemental methods.
Results
The rate of SD/CA
The median age at SD/CA was 15.4 years (IQR=11.8–22.0 years); however, SD/CA was unevenly distributed across the age ranges, with the majority (29/39) in the 8–19 years old age range. Excluding the 12 patients who presented with sudden death as the first sign of illness, there were 27 primary endpoints in 1635 patient years, corresponding to an overall annual rate on follow-up of 1.7%, but with all but one event occurring after the age of 8 years. In the 1972–1999 cohort overall annual rate was 1.8%, and in the 1999–2014 cohort 1.1%. SD/CA occurred 7.0 (3.0–15.4) years after diagnosis, but with a range of 1 month−35 years. Table 1 compares categorical features in patients free of SD/CA (and surviving at least 2 years) with the SD/CA group. In this table all 39 patients who suffered SD/CA are included for age and gender, and some other categorical features, and 32 SD/CA for ECG measures.
Categorical clinical features in the national cohort of paediatric patients with HCM: SD/CA individuals compared with survivors
Important risk predictors
Table 1 shows that there was no gender preponderance for SD/CA, and that all the morphological ECG features used in the ECG risk score17 were significantly more common in the SD/CA group. The only medical therapy that was more common among survivors than the SD/CA group was beta-blocker therapy, whereas absence of any medical therapy was more prevalent in the SD/CA group.
Table 2 illustrates the distribution of quantitative ultrasound and ECG measures between the SD/CA group and surviving patients. Both ultrasound measures of hypertrophy and ECG measures had significantly higher values in the SD/CA group. All SD/CA patients had substantial cardiac hypertrophy at least of interventricular septum (last Detroit Z-score 4.02–8.7), although occasionally predominantly apically.
Ultrasound and ECG measures comparing cardiac arrest group with survivors
In table 3 we show relative risk between SD/CA group and survivors using both previously published suggested risk factor cut-offs and additional cut-off values suggested by the frequency distribution plots of our SD/CA group compared with survivors. SD/CA group has n=32 for ECG measures and n=27 for echocardiographic measures. The ECG risk score >5 had the highest relative risk and the best sensitivity of 97% as well as a specificity of 80%. Of wall thickness measures the two measures related to body size (Detroit Z-score maximum wall thickness >4.5) or to upper limit of normal for chronological age (SEPPER ≥190% of normal) show better discrimination than absolute wall thickness measures. Note, however, that the previously suggested cut-off for Z-score >613 has a sensitivity of only 56%, but a high specificity, whereas the Z-score cut-off >4.5 suggested by the frequency distribution in our groups has better sensitivity. ST depression ≥2 mm at rest (in any one lead but usually precordially) has high specificity (92%). In the lower part of the table are values where we have less complete data, but nevertheless nsVT on Holter, ventricular ectopics on exercise and ST depression at exercise all have relative risks between 9.1 and 5.7, with nsVT on Holter having the highest sensitivity. Any LVOT gradient at rest confers a significant risk, but it is at its highest at gradient >50 mm Hg at rest. The left atrium-to-aorta diameter (LA:Ao) ratio >1.5 has a lower degree of increased risk, and neither pathological blood pressure on exercise, family history of sudden death among those patients who had familial HCM or cardiac syncope reached a significant relative risk.
Ranking based on relative risk value of risk factors for sudden death in the national cohort, as recorded at last follow-up: sudden death/cardiac arrest individuals compared with survivors, values with (95% CI)
To assess the impact of these risk factors on all patients in the national cohort, that is, also including those who had had heart transplants or died from other types of cardiac death than sudden arrhythmia death, we used Cox hazard regression. The endpoint assessed, however, is still only SD/CA. Some parameters have incomplete data (see table 3 for numbers).
Table 4 shows the possible early predictors of SD/CA on univariate analysis. Factors significantly increasing risk were first LLQRSS, first ECG risk score, degree of hypertrophy at presentation both related to chronological age or when expressed as Z-score, and left atrial enlargement expressed as LA:Ao ratio. One factor reduced the risk, namely increasing amount of early beta-blocker dose. Cox hazard regression with categorical factors suggested increased risk from LVOTO at rest, but significant protection by beta-blocker-therapy and by disopyramide combined with beta-blocker, whereas calcium-blocker therapy, amiodarone therapy or myectomy, like family history of sudden death, gender and age at diagnosis, had no significant effect on risk for SD/CA. In spite of incomplete data nsVT on Holter was highly significant.
Cox hazard univariate proportional regression: risk factors for sudden death at presentation and early follow-up in total cohort of patients with both ECG and wall thickness data (n=140; SD/CA=27)
Independent early risk factors and influence of therapy
At diagnosis the LLQRSS was more predictive than the ECG risk score and remained in the multivariate model (whereas at latest follow-up the ECG risk score was more predictive than LLQRSS and accordingly remained in that model) (table 5). Analysed together SEPPER eliminated Detroit Z-score and maximum wall thickness for measure at diagnosis; however the multivariate model using Z-score instead of SEPPER produces essentially the same additional early significant risk factors in the model, namely LLQRSS and LVOTO at rest, together with degree of hypertrophy expressed as either SEPPER or Detroit Z-score. Importantly, early beta-blocker dose is independently associated with significant reduction in risk with increasing dose also in the multivariate model. Excluding patients with Noonan spectrum syndrome does not alter results; the same factors remain in the final multivariate models (online supplementary table S3).
Cox hazard proportional regression multivariate analysis of risk factors: significant risk factors remaining in model after testing factors in table 4 (n=140; SD/CA n=27)
Independent predictors at latest follow-up
The last Z-score is the most predictive wall thickness measure in the multivariate model together with last ECG risk score as the most predictive ECG measure (table 5). Tested together the ECG risk score eliminated the presence of nsVT on Holter from the model. Disopyramide+beta-blocker therapy was associated with greater reduction in risk in the multivariate analysis than last beta-blocker dose, but this was not unrelated to beta-blocker dose, as the average beta-blocker-dose in the patients also receiving disopyramide (n=39) was 11.7±12.2 (±SD) mg/kg of propranolol equivalents as compared with the average dose in all beta-blocker-treated patients of 5.5±8.2 mg/kg. Thus the multivariate Cox hazard regression data for last beta-blocker dose in the multivariate model are also given in table 5.
How predictive are the risk factors?
This is illustrated in table 6 based on results from last follow-up. It can be concluded that ECG risk score is the most consistent of the predictors and has the best combination of positive (45%) and negative (99%) predictive values.
Positive and negative predictive values of important risk factors
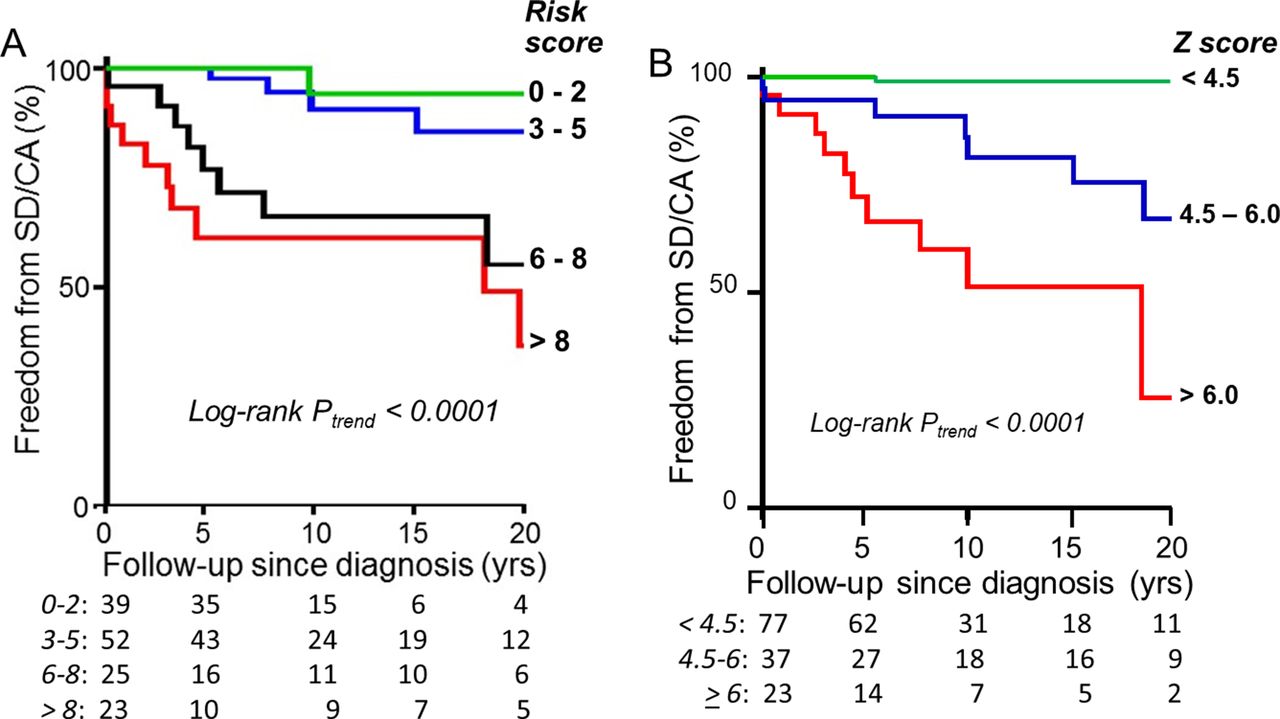
ECG risk score is also a powerful early predictor, with 30.6% of patients with initial ECG risk score >5 having SD/CA during the first 5 years of follow-up. In five patients suffering a later SD/CA but diagnosed at aged 0–2 years, four had limb-lead QRS sum >10 mV at diagnosis and two already had risk scores >5 on the first ECG; all developed high-risk scores on follow-up several years before SD/CA. Among patients with later SD/CA but diagnosed at age 3–10 years, 16/18 had limb-lead QRS sum >10 mV and 16/18 had risk score >5 points already at diagnosis; thus, ECG appearance is a very early indicator of risk. Among the 10 patients with SD/CA occurring after 19 years of age, 9/10 had an ECG risk score >5 already at last childhood follow-up. Freedom from SD/CA in the first 5 years is 100%, with initial risk score of 0–2, and 97.6% with initial risk score of 3–5. ECG risk score is not a binary risk factor but confers an incrementally increased risk (figure 1A), and the same is true of Detroit Z-score (figure 1B).

{kind=link}
(A) illustrates Kaplan-Meier analysis of freedom from sudden death or resuscitated cardiac arrest in patients stratified according to the ECG risk score at diagnosis, and illustrates a progressively increasing risk with increasing risk score, with p value for log-rank trend <0.001. The patients with risk score ≤2 have excellent long-term prognosis with only 1/39 later progressing to a risk score of 10 points and sudden death. The group with risk scores 3–5 points has a good 5-year prognosis, but later on 4/52 suffered SD/CA with progressive disease. The groups with risk scores 6–8 points and >8 both have early attrition with SD/CA, fastest in the group with the highest scores. The numbers below the x-axis relate to the numbers of subjects at risk at various time points. (B) illustrates corresponding analysis in the patients stratified for initial Z-score of maximum wall thickness. The group of 77 patients with initial Detroit Z-score <4.5 has 98.7% freedom from SD/CA during the first 20 years of follow-up (although an additional two SD/CA occurred after 20 years in patients with progressive disease). Those with initial Z-scores of 4.5–5.99 have significant early risk of SD/CA, although the risk is clearly proportionately greater in the group with Z-scores ≥6, p-value for log-rank trend <0.001. The numbers below the x-axis relate to the numbers of subjects at risk at various time points. SD/CA, sudden death/cardiac arrest.
Malignant family history
High-risk ECG risk score was more common in familial HCM with family history of sudden death (43%) than in familial HCM without malignant family history (33%). Looking at the subpopulation of familial HCM where there was a family history of sudden cardiac death (n=35), there were eight individuals with SD/CA. From table 7 it is apparent that those patients with a malignant family history who suffered SD/CA were readily identifiable solely on phenotypic markers as high-risk patients already at diagnosis, and with median ECG risk score at last follow-up of 8 (8/8 had a risk score >5), and other risk indicators also emphatically in high risk range. The survivors who had not experienced a cardiac arrest on the other hand had median and IQR values indicating low risk in all ECG and ultrasound measures; only 22% of those had an ECG risk score >5 (p=0.0001). This suggests that it is the phenotype per se that defines the risk, not the family history.
Characteristics of patients with family history of sudden death
Discussion
As described in the Introduction, the risk stratification strategies that have been used hitherto have not been particularly successful in selecting the right paediatric patients with HCM for primary prevention of ICD implantation, since in paediatric patients with ICD the annual rate of appropriate shocks was 3%/year, with the rate of serious complications threefold larger, 9%/year.6 The considerable morbidity of ICD implantation detailed in the Introduction makes it desirable to identify a population with a higher event rate for primary prophylactic ICD implantation. How to improve risk stratification for adult patients has been discussed extensively elsewhere,10 11 21 but the proposed ESC risk calculator is not applicable to patients <16 years of age.10
What is the role of ECG in risk stratification?
It has been shown that risk factors for sudden death were different from risk factors for heart failure-related death in paediatric patients with HCM, and that a limb-lead QRS amplitude sum (LLQRSS) >10 mV was a risk factor that was independent from degree of ultrasound-measured hypertrophy.16 McLeod et al 22 reported that there were no sudden deaths in adult patients with HCM with a normal ECG. Furthermore, the appearance of ST segment hump during exercise testing, ST segment depression in high lateral leads and prolongation of QTc are risk factors for sudden death in adult patients with HCM.23–27 A detailed study of the resting ECG in adult patients with HCM showed LLQRSS, 12-lead amplitude duration product, QTc >440 ms, T wave inversion, ST depression and dominant S waves in V4 to be correlated with risk for arrhythmia, and an ECG risk score was proposed, which when >5 points gave a sensitivity for cardiac arrest of 84% and high specificity in patients <40 years of age.17 The same cut-off confers a relative risk of 46.5 (6.6–331) in this paediatric national cohort, with sensitivity of 97% and specificity of 80%, for the prediction of SD/CA in paediatric patients with HCM (see table 2). It is a powerful predictor of adverse outcome already at diagnosis (see figure 1A), as well as the single most powerful ECG risk predictor at late follow-up on multivariate Cox hazard regression (see tables 5 and 6). LLQRSS may be a more sensitive marker for high risk of sudden death at the time of diagnosis (see Table 5), but it is a less specific risk indicator than the initial ECG risk score (table 3). We have observed on serial ECGs in the same patient that peak voltages often drop when QRS complex durations increase, and this impression may explain why we find that the ECG risk score, which also scores the 12-lead amplitude × duration product, is the more dependable risk indicator to follow long-term. ST segment depression is probably more predictive in paediatric patients where it is rare and has a specificity of 92% than it could be in adult tertiary specialist centre populations, where it was present in 56% of a population with a mean age of 50 years.27 In addition increased QTc dispersion has been associated with increased risk in paediatric HCM populations,12 15 but this measure was not entered in our registry. It is desirable that the ECG risk score is tested also in other paediatric cohorts, and that a separate paediatric risk calculator is developed for those risk factors that are important in childhood HCM.
Why do adult and paediatric populations differ in the risk prediction from family history of sudden death?
There are two major possibilities: the paediatric studies might have had insufficient statistical power to detect a small but significant effect, or the adult studies have not carried out a multivariate analysis that included all important inheritable risk factors. As regards insufficient statistical power that cannot be totally excluded for the univariate analysis in the paediatric studies. However when one looks at the relative risk or HRs shown in the paediatric studies (Decker et al relative risk 1.0,13 Moak et al HR 1.0,14 our data relative risk in familial HCM 1.2 (0.5–2.8)), it is clear that any increase in risk if it exists would have to be very small in relation to that caused by other much more powerful risk predictors, and that specificity is very poor, only 55% (table 2). In our data any risk evaporates in multivariate analysis. None of the adult studies that have shown malignant family history as a significant risk factor have carried out a multivariate analysis that included any ECG-derived risk factor. In one large study (1004 patients) that did include some ECG risk factors in multivariate analysis, the influence of a family history of sudden death was no longer significant in the multivariate model.27 A Cochrane review by Christiaans et al 11 reported that five studies failed to show that family history of sudden death was a significant risk factor, with three actually showing HRs <1.0, and the four studies showing a significant effect emanated from only two supraregional centres with special interest in HCM. McKeown and Muir21 has, in an editorial, raised the possibility that risk factor data from centres with a long-standing renown for HCM research might be influenced by referral bias, with families with a malignant family history more likely than others to be referred there. As we found that a malignant ECG phenotype is 32% more common in HCM with a family history of sudden death than in those with a benign family history, it is possible that there is a linkage between high ECG risk score and a malignant family history. It may be that what is inherited is not a risk by itself, but a higher propensity to develop HCM with a malignant ECG phenotype, a notion that would be supported by the findings by Biagini et al.27 Further studies of correlations between genotype and ECG phenotype would appear to be indicated. What our data in table 7 show is that phenotypic markers are far more accurate than family history in pinpointing risk.
Which risk factors are we to include in evidence-based paediatric risk stratification?
ECG phenotype is important, and in our cohort the ECG risk score >5 points is the single most powerful predictor; it identifies 97% of patients suffering from SD/CA, with a negative predictive value of 99%, and confers a 30.6% risk of having SD/CA during first 5 years of follow-up. The degree of hypertrophy relative to normal for age or body size, not as absolute wall thickness numbers, is also an important predictor,16 but it is crucial that Z-scores used agree with in-house measurement data (see online supplementary methods). Suitable high-risk indicator values might be SEPPER >190% or Detroit Z-score >4.5, although they are continuous and not binary risk factors. Presence of LVOTO at rest remains a significant risk factor in the multivariate model (table 5), and is particularly prominent if resting gradient >50 mm Hg. The presence of non-sustained VT on Holter is an important risk factor,12 14 15 also noted in our univariate analysis, with a high positive predictive value of 59 (36–79)%, although in our multivariate model it is eliminated by the ECG risk score, which has higher sensitivity. The above four factors are elements that ought to be included in a paediatric risk calculator. A family history of sudden death has not been shown to be a risk factor, let alone an independent risk factor, in now five out of five paediatric studies,12–15 and thus present balance of evidence suggests that it should not be included in paediatric risk calculators.
Pathological blood pressure response on exercise testing has low specificity,13–15 but exercise testing can give other potentially important indicators; both the appearance of ventricular ectopics during exercise testing and ST segment depression on exercise testing had high specificity, 93% and 83%, respectively, for SD/CA, but low sensitivity (table 2). Further studies with more complete data are desirable to define the role of exercise testing.
On current data a reasonable clinical approach might be to, as a minimum, refer all paediatric patients with HCM with ECG risk scores ≥3 points and/or Detroit Z-score ≥4.5 for Holter recording and exercise testing, and to ensure that a 12-lead ECG is performed at every follow-up visit.
The effect of pharmacological therapy
There are no prospective randomised trials of long-term effects of any pharmacotherapy in HCM using mortality as endpoint. In adults with chronic heart failure, however, it has been established by several large randomised prospective studies that beta-blockers, particularly lipophilic ones, give significant reduction in sudden deaths (see review by Hjalmarson28). Duration of action and use of slow-release preparations to obtain relatively even beta-blockade over 24 hours may also be important in protection as well as reducing side effects. High-dose beta-blocker therapy (>4.4 mg/kg propranolol equivalents), in this cohort mostly given as slow-release propranolol or metoprolol preparations twice daily (both lipophilic), has previously been associated with a significantly improved survival in paediatric HCM,16 18 29 which was dose-dependent over a range of doses30 and with a lower risk of sudden death.16 The fact that the protective effect of beta-blockers remains clearly significant on multivariate analysis in the current study, as well as being dose-related, suggests that this might indeed be a pharmacological effect and not a chance association. The finding implies that future studies of risk factors ought to include possibly modifying pharmacological therapy in their multivariate models, and that further studies of the effect of beta-blocker dose on survival in prospective registers are desirable. As regards disopyramide it can be concluded that disopyramide therapy is not harmful or proarrhythmic in paediatric HCM.
Limitations of study
A retrospective national cohort study without referral bias is ideal for the study of risk factors for adverse outcome, and enables calculation of true positive and negative predictive values, but a retrospective study is not designed for the assessment of treatment effects. Nevertheless, our long and complete follow-up provides a large number of patient years for analysis not easily achievable in prospective randomised trials in this condition.
Conclusions
ECG changes are a powerful predictor of risk for malignant arrhythmia in childhood HCM, and the simple resting ECG, together with ultrasound Z-scores of cardiac hypertrophy, provides a cheap and accessible tool for rapid early risk stratification and selection of high-risk patients of high priority for further investigations. A family history of sudden death is not an independent risk factor, and should not on its own be an indication for ICD implantation in a child who has a low-risk phenotype.
References
Footnotes
Contributors Study conception and design: IÖ-S. Acquisition of data: IÖ-S, GS, AR, PL, EF. Analysis and interpretation of data: IÖ-S, EF. Drafting of manuscript: IÖ-S. Critical revision: IÖ-S, GS, AR, PL, EF.
Funding The study was supported by grants from the Swedish Heart and Lung Foundation (Number 20080510), and by Gothenburg University ALF project grant (ALFgbg-544981).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Detailed data on type of pharmacotherapy and dose are available to share with any collaborative studies studying relationship between pharmacotherapy and outcome.