Article Text

Abstract
Objective Cardiac resynchronisation therapy (CRT) is an effective therapy for selected patients with heart failure (HF); however, a significant non-response rate exists. We examined current evidence on extracellular cardiac matrix (ECM) biomarkers in predicting response following CRT.
Methods Complete literature review of PubMed, Ovid SP MEDLINE, Cochrane Library and TRIP, reference lists, international cardiology conferences and ongoing studies between December 1999 and December 2015 conducted according to prospectively registered study selection and analysis criteria (PROSPERO:CRD42016025864) was performed. All observational and randomised control trials (RCT) were included if they tested prespecified ECM biomarkers’ ability to predict CRT response. Risk of bias assessment and data extraction determined pooling of included studies was not feasible due to heterogeneity of the selected studies.
Results A total of 217 studies were screened; six (five prospective cohort and one RCT substudy) were included in analysis with 415 participants in total. Study sizes varied (n=55–260), cohort characteristics contrasted (male: 67.8%–83.6%, ischaemic aetiology: 40.2%–70.3%) and CRT response definitions differed (three clinical/functional, three echocardiographic). Consistent observation in all ECM biomarker behaviour before and after CRT implantation was not observed between studies. Lower type I and type III collagen synthesis biomarkers (N-terminal propeptides of type I and III procollagens) expression demonstrated replicated ability to predict reverse left ventricular remodelling.
Conclusion Collagen synthesis biomarkers offer the most potential as ECM biomarkers for predicting CRT response. Heterogeneity between these studies was large and limited the ability to pool and compare results numerically. Use of different response definitions was one of the biggest challenges.
- Extracellular Cardiac Matrix
- Chronic Heart Failure
- Cardiac Resynchronization Therapy
- Systematic Review
- Response Definition
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Extracellular Cardiac Matrix
- Chronic Heart Failure
- Cardiac Resynchronization Therapy
- Systematic Review
- Response Definition
Key questions
What is already known about this subject?
Cardiac resynchronisation therapy (CRT) is associated with non-response in 20%–40% of selected patients with heart failure (HF). Selected vascular biomarkers are known to be associated with cardiac disease but it is unknown whether these can be used to predict CRT response.
What does this study adds?
We performed a systematic review of all studies examining vascular biomarkers in CRT. We found that collagen synthesis biomarkers have the most potential for predicting CRT response, particularly N-terminal propeptides of type I and III procollagens. Matrix metalloproteinases-2 and 9 have no conclusive predictive value and need further investigation.
How might this impact clinical practice?
Use of vascular biomarkers to predict CRT response could have enormous clinical benefit by selectively identifying those patients with HF who are likely to benefit. This has important implications for both patients and healthcare providers worldwide, especially given the current financial climate.
Introduction
Cardiac resynchronisation therapy (CRT) is an effective therapy for selected patients with heart failure (HF).1 2 Current guidelines suggest that CRT is offered to those with a left ventricular ejection fraction (LVEF) ≤35% with resting 12-lead ECG QRS duration ≥150 ms or 120–149 ms with Left Bundle Branch Block (LBBB) morphology and refractory to optimal medical therapy (OMT).3 CRT reduces mortality and improves morbidity, underpinned by reversal of pathophysiological adverse cardiac remodelling.1 2 Unfortunately, a significant non-response rate of 20%–40% exists and has remained unchanged over the last decade, despite extensive research and investment.1 2
The extracellular cardiac matrix (ECM) is a dynamic support structure that remodels following cardiac injury and HF.4 5 Progressive ECM remodelling is closely linked to HF severity and prognosis.4 5 Cardiac collagen turnover alterations are central to the development and progression of cardiac fibrosis and HF.5 Specific biomarkers of type I and type III collagen synthesis (N-terminal propeptides of type I and III procollagens (PINP and PIIINP),6 7 carboxy-terminal propeptide of procollagen type I (PICP))8 9 and degradation (carboxy-terminal telopeptide of type I collagen (ICTP or CITP))9 10 products are associated with poor outcomes in HF. The proteolytic enzyme system matrix metalloproteinases (MMPs) and their regulators tissue inhibitors of MMPs (TIMPs) are involved in collagen degradation and have been implicated in HF development and progression.4 5 Specifically, MMP-1,11 a collagenase, MMP-212 and MMP-9,13 both gelatinases and TIMP-111 are associated with HF outcomes. Galectin-3 (Gal-3) is a beta-galactoside-binding lectin released by activated cardiac macrophages, which are upregulated in HF, causing increased fibroblast proliferation, collagen deposition and ventricular dysfunction.14 Gal-3 is strongly associated with inflammation and fibrosis with raised levels strongly predict poor HF outcomes.14
Turnover of ECM alters in HF and with reverse cardiac remodelling following CRT implantation may offer potential biomarkers for response prediction.15 This systematic review examines the current evidence on the value of ECM biomarkers in predicting CRT response.
Methodology
Our systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines.16 It was prospectively registered with PROSPERO (CRD42016025864), an international registry of systematic reviews. A protocol was designed and implemented prospectively in-line with PRISMA-P 2015.17
Eligibility criteria
Strict eligibility criteria were applied to minimise heterogeneity of included articles. Observational studies (prospective or retrospective) and randomised control trials (RCTs) (including substudies) were included; basic science and review articles were excluded. Included study populations represented patients with HF meeting international CRT implant guidelines.3 Studies had to be conducted on adults (age ≥18 years). Articles were included if they examined an ECM biomarker previously reported to predict HF outcomes.4 Baseline ECM biomarkers, measured when patients were clinically stable prior to implantation, had to be compared with a predefined CRT ‘response’ criteria to evaluate their predictive value. Coronary sinus sampling and long-term trends in peripheral ECM biomarker behaviour were analysed if present.
A variety of clinical, functional or echocardiographic criteria and cardiovascular outcomes have been used to define CRT response in studies,18 which often correlate poorly. All response criteria were included in the review. Cardiovascular outcomes could form part of a response definition or be presented separately; their absence was not an exclusion criterion.
Database search strategies
Detailed searches were conducted on PubMed, Ovid SP MEDLINE, Cochrane Library (CENTRAL) and TRIP in February 2016 by one author (CM) and reviewed by another independently (DA). The search strategy used specific terms (cardiac resynchronisation therapy/cardiac pacing/extracellular matrix) in combination, within titles/abstracts or Medical Subject Headings. Specific vascular biomarkers (‘TIMP’ ‘MMP’ ‘collagen’ ‘Myostatin’ ‘Syndecan-4’ and ‘Galectin-3’) were included in the search. A grey literature search involved searching the Clinical Trials database (www.clinicaltrials.gov) and international cardiology conferences (European Society of Cardiology, American Heart Association, American College of Cardiology) indexes for ongoing, abstracts and unpublished work. All included articles had their references searched for relevant publications. A date limitation of the last 15 years (31 December 1999– 31 December 2015) was applied. No language restrictions were applied.
Title and abstract reviews were performed independently (CM/DA), consensus on eligibility criteria was required to be taken forward to full paper review; any conflicts were decided by an independent reviewer (FO). Duplications of articles or cohort use were identified and only the most relevant (decided by consensus) taken forward. The Critical Appraisal Skills Programme checklist (dependent on study design) was applied to full paper review to guide evaluation of article quality.19 Consensus had to be reached on full paper reviews before being selected for inclusion; where consensus was not reached a third reviewer (FO) made the final decision. Contact was attempted with all included article authors and any others at full paper review that were indicated.
Data extraction and management
Full texts of included articles were obtained. Pilot data extraction was performed on two randomly selected articles and reviewed for robustness (CM, DA, FO, PB). A standardised data extraction form was created to collect data on each study’s design (eligibility criteria, methodology, assessment period), patient population (numbers, age, gender, aetiology, ECG, left ventricular (LV) geometry, quality of life, New York Heart Association (NYHA), functional assessment), vascular biomarker/predictor (specific ECM surrogate biomarkers, units, conditions of sampling, laboratory assessment, statistical prediction model) and outcome (response definition and cardiovascular outcomes). Data extraction was performed by two independent reviewers (CM/DA), a third independent reviewer (FO) resolved any disagreement.
Risk of bias assessment
Risk of bias for each study was assessed by two independent reviewers (CM, DA) utilising either the Risk of Bias Assessment Tool for Non-randomised Studies or the Cochrane Collaboration ‘Risk of Bias’ assessment tool.20 21 Both have established criteria to examine selection bias, exposure measurement, blinding and completeness of outcome data.20 21
Data synthesis and analysis
A descriptive synthesis was performed to summarise findings of all selected articles. A meta-analysis of included study data for each specific ECM biomarker was not possible due to heterogeneity of outcome definitions and study designs. Evaluation of study designs, defined outcomes and cohort characteristics was performed. The same biomarkers compared in different included articles were compared. Continuous variables were summarised using the same units for each variable in the original text. Data were presented as mean ± standard deviation (SD), unless specified otherwise.
Results
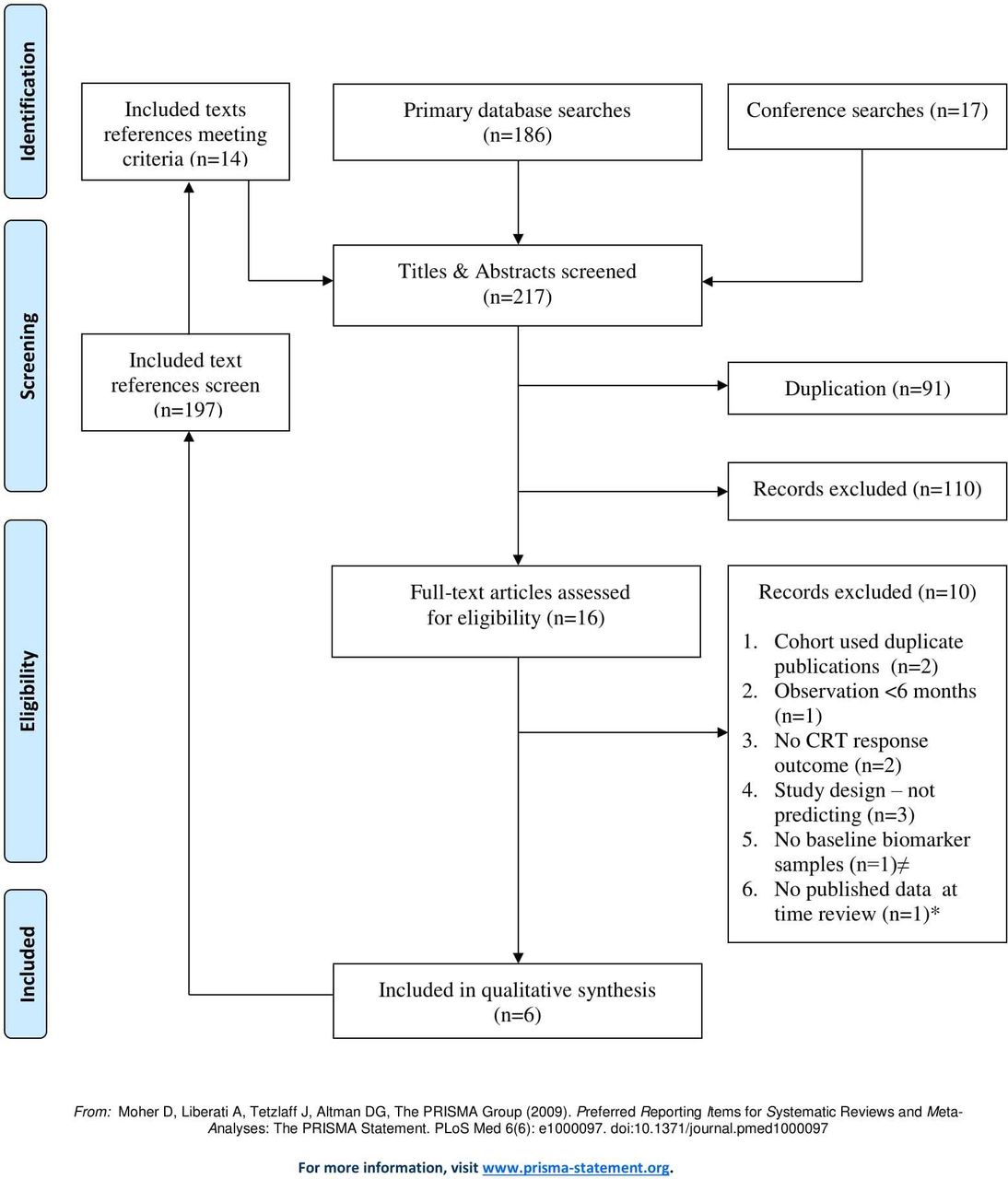
Figure 1 shows the screening and selection of published articles; 110 records were excluded after the screening stage as they did not meet inclusion criteria. Six articles met the inclusion criteria. Two abstracts22 23 and one clinical trial entry (www.clinicaltrials.gov) (NCT15019908) were taken to full review (for potential inclusion). Related articles and information were sought, including contacting authors (all three kindly responded). None yet had articles published and additional information provided led to exclusion from review (no baseline biomarkers taken22 or study design did not test biomarkers as predictors23).
{kind=link}
Flowchart of studies screening and selection. ≠Author contacted, poster presentation sent and no baseline extracellular cardiac matrix biomarker sample taken.22 *Clinical trial (NCT15019908) author contacted and manuscript in preparation. CRT, cardiac resynchronisation therapy.
Study design
Five prospective cohort studies and one RCT substudy11 were included. Table 1 summarise the different study designs and CRT response outcome definitions used. Studies selected were published between 2008 and 2014. Risk of bias was assessed in each study using appropriate quality check tools. The lowest risk of bias was in the single RCT substudy.11 The prospective cohort studies varied minimally in their bias assessment and none were excluded.
Study designs and response outcome definitions
Garcia-Bolao et al9 stated that 61 participants were consented; during the observation period there were four mortalities (three cardiac/one non-cardiac) and one functional assessment not performed at follow-up (6 min walk test not completed due to stroke). The cohort was 59 but no explicit statement about the two exclusions made. Lopez-Andres et al11 published a substudy in 2012 of the ‘The Effect of Cardiac Resynchronization on Morbidity and Mortality in Heart Failure’ (CARE-HF)1 RCT which itself was published in 2005; interpretation of results is within this context. All studies included NYHA III–IV patients (mostly NYHA III). Two studies recruited NYHA II patients24 25 with one also requiring a bradycardia pacing indication.24 All studies included QRS duration >120 ms, except Garcia-Bolao et al9 (QRS≥130 ms). In the CARE-HF trial, those with QRS duration 120–149 ms needed dyssynchrony on echocardiography.1 8 All transvenous LV leads were implanted preferably to the most lateral position possible. Dong et al26 performed only de novo CRT-defibrillator (CRT-d) implants. Three studies10 24 26 commented on right ventricular lead placement with two26 explicitly aiming for the right ventricular apex. In CARE-HF (and substudy), all had CRT-pacemaker (CRT-p) devices only.1 11 CRT response definitions varied between included studies. Broadly, response definitions used were classified as three clinical and three echocardiographic. Reported response rates varied between 48.9% and 71.8% (table 1).
Baseline characteristics
The baseline characteristics of the patients are shown in table 2.
Baseline characteristics
A total of 415 patients were included. The five prospective observational studies had mean age of 67±10 years9 10 (Lopez-Andres et al8 excluded as presented as median and IQR). There were 315 (75.9%) males in included studies, ranging 67.8%9–83.6%.25 There was large variation in frequency of CRT-d/CRT-p implants in each study with two not providing this data.10 25 One study included a high proportion of device upgrades25; the CARE-HF trial excluded upgrades,1 8 the remaining four studies did not state upgrade status.9 10 24 26 Atrial fibrillation (AF) was included in three prospective observational studies8 24 25; one did not report on AF or related publications.10 27 Precise QRS duration was not stated in two studies.24 26 Reporting of LV volumetric data varied between included studies. Three reported unadjusted LV end systolic volume (LVESV) and LV end diastolic volume (LVEDV) data which were similar to each other (table 3).10 24 25 Dong et al26 presented LVESV and LVEDV volume indexed figures only. Garcia-Bolao et al9 provided LVEF only. LVEF was compared between the five prospective cohorts and showed similar mean LVEF between 25%–27%.9 10 24–26
Baseline ECM biomarkers concentrations between responders versus non-responders and their predictive value within included studies
Responder versus non-responders
Response status (responders vs non-responders (RvsNR)) was presented in four of the included studies.9 10 24 26 Truong et al25 did not provide characteristics of those defined by response. Lopez-Andres et al8 outlined characteristics by allocation to CRT-p versus OMT, however, not by response. There were some baseline characteristic differences between the four studies for RvsNR9 10 24 26; Dong et al26 demonstrated differences between RvsNR for LBBB status (15 (68.3%) vs 9 (39.1%), p=0.05) and ischaemic aetiology (9 (40.9%) vs 17 (73.9%], p=0.03). Tolosana et al24 reported lower creatinine levels in RvsNR (1.25±0.3 mg/dL vs 1.76±0.8 mg/dL, p=0.01). Umar et al10 reported that responders were older and had longer QRS duration than non-responders (age: 66±10 years vs 60±11 years, p=0.03; mean± standarderror QRS: 165±3 ms vs 135±8 ms, p=0.001). Notably, Hessel et al published a study using the same cohort as Umar et al and reported no difference in QRS duration for RvsNR (165±2 ms vs 153±3 ms, p=NS), suggesting one of these studies has recorded it incorrectly.10 27
ECM biomarkers
All ECM biomarker baseline concentrations and magnitude of association (if tested) are summarised in table 3. Lopez-Andres et al8 did not provide baseline concentrations by response status, but comparison was made with the control group. Umar et al10 showed baseline results for expression of ECM biomarkers studied. However, for PIIINP non-responders no baseline concentration was reported in the article, however no statistical significance is reported RvsNR.10
PINP/PICP
PINP and PICP share a 1:1 stoichiometric relationship with the collagen molecule; therefore, they were considered together. Umar et al10 reported similar total cohort means values to Lopez-Andres et al8 median values (the skew of this data is unknown). Umar et al10 observed higher PINP baseline level predicted poor response. Garcia-Balao et al9 reported the opposite for PICP. Lopez-Andres et al8 observed no significant association of baseline PINP with CRT response or other outcomes. Variation in the pattern of reported levels between the three studies were likely due to differences in response definitions and baseline characteristics. Garcia-Balao et al9 utilised a clinical definition of response, whereas the other two studies used echocardiographic criteria.8 10 All studies varied in duration of follow-up. Umar et al10 had a higher proportion of men with ischaemic aetiology than the other studies. Lopez-Andres et al8 excluded AF, whereas within the Garcia-Balao et al9 cohort it was present in 18.6% of participants. Garcia-Balao et al9 tested the predictive value of type I collagen turnover with the PICP:CITP ratio with a ratio ≥14.4 predicting response.
PIIINP
Variation was reported in trends of PIIINP levels at baseline. Dong et al26 reported logarithmic figures making absolute figure comparison challenging. Geometric means could be calculated, but given small numbers of participants this was likely to underestimate the true mean.26 Higher PIIINP levels in HF versus healthy controls (0.88±0.21 ug/L vs 0.71±0.14 ug/L, p=0.01) were observed.26 Responders had significantly lower PIIINP baseline levels than non-responders (p=0.03).26 Umar et al10 demonstrated no difference in baseline levels between RvsNR. Lopez-Andres et al8 reported similar baseline levels between CRT-p and OMT, but did observe PIIINP (>4.7 ug/L) in univariate analysis predicted cardiovascular outcomes (death or HF hospitalisation at 18 months) (OR 1.80, 95% CI 1.06 to 3.06, p=0.03).8
ICTP or CITP
Both ICTP and CITP were used to represent carboxyl-terminal peptides of type I collagen in three included studies. Umar et al13 and Garcia-Balao et al12 demonstrated similar baseline means for ICTP/CITP for the entire cohort. Neither identified independent predictors of CRT response.9 10 Garcia-Bolao et al9 identified that the PICP:CITP ratio strongly predicted response but was driven by PICP. Lopez-Andres et al8 observed similar expression between CRT-p and OMT groups and showed no predictive value.
MMP-1, MMP-2 and MMP-9
There were variations in reported baseline concentrations for MMP-1. The mean for MMP-1 in Garcia-Bolao et al9 was higher than median observed in CRT-p and OMT groups in Lopez-Andres et al,8 though the data skew is unknown. Garcia-Bolao et al9 examined the predictive value of MMP-1:TIMP-1, given their intrinsic regulatory role in collagen turnover,5 but showed no statistical significance. Lopez-Andres et al8 observed with a baseline MMP-1 ≤3 ug/L an adjusted threefold increased risk of CRT non-response and an increased risk of death or N-terminal pro B-type natriuretic peptide >1000 ng/L (OR 2.23, 95% CI 1.00 to 5.00, p=0.051/0.073 adjusted with/without renal function).8 A precursor to MMP-1 called pro-MMP-1 (pro-MMP-1) was studied by Umar et al.10 They observed no difference in baseline pro-MMP-1 expression between RvsNR.10
Two studies reported cohort means for MMP-2 baseline concentration with large differences (table 3). Responders had lower MMP-2 baseline concentrations in both studies. Tolosana et al24 reported a significant difference between RvsNR (p=0.02), whereas Garcia-Bolao et al9 demonstrated no difference. The differences are not fully explained by study design, response definition or cohort characteristics as they showed similarities (tables 1 and 2). Variation in levels may be due to Tolosana et al24 using plasma and Garcia-Bolao et al9 using serum in their sandwich ELISAs. MMP-9 was reported by Garcia-Bolao et al,9 who observed a trend towards lower baseline MMP-9 concentration for Responders. Baseline MMP-9 did not predict CRT response.9
TIMP-1
Tolosana et al24 observed that responders had significantly lower concentrations at baseline of TIMP-1 than non-responders. Neither Umar et al10 nor Garcia-Bolao et al9 observed a significant difference in baseline TIMP-1 concentration between RvsNR. Higher peripheral TIMP-1 was identified as an independent predictor of non-response by Tolosana et al24 in multivariable analysis; a concentration of ≥248 ug/L had a 71% sensitivity and 72% specificity for predicting non-response. However, Umar et al10 did not identify TIMP-1 as a predictor. Garcia-Bolao et al9 tested TIMP-1 in the MMP-1:TIMP-1 ratio and did not identify TIMP-1 as a significant predictor of RvsNR.
Gal-3
Lopez-Andres et al8 reported higher baseline levels of Gal-3 than Truong et al,25 due to different response definitions and variation in cohort characteristics. Lopez et al8 used an echocardiographic definition at 18 months and Truong et al25 utilised HF clinical composite score at 6 months. Truong et al25 has higher ischaemic aetiology (53.4% vs 40.2%) and included patients with AF. Neither study reported baseline concentrations for RvsNR.8 25 Truong et al25 observed that peripheral baseline Gal-3 above a preset concentration (>25.9 ug/L) had low sensitivity and high specificity for predicting CRT response.
Discussion
The ECM is a highly dynamic structure that is integral to myocardial structure and function which detrimentally remodels following cardiac injury leading to the altered turnover, replacing contractile tissue with collagen rich connective tissue and ultimately the development of myocardial fibrosis.5 Myocardial fibrosis is characterised by adverse remodelling which contributes to systolic and diastolic HF.5 28 PINP, PICP and PIIINP are released into the circulation during conversion and deposition of procollagen to collagen and are upregulated during myocardial fibrosis and associated with adverse HF outcomes.5 7 15 28 Mechanistically, higher upregulation of collagen would challenge a CRT’s ability to reverse remodel and for the patient to respond. Umar et al10 supported this hypothesis observing significantly lower baseline PINP expression predicted echocardiographic response. Dong et al26 did observe lower baseline PIIINP predicted echocardiographic response on univariate analysis, but not multivariable analysis. In contrast, Garcia-Balao et al9 observed higher baseline expression of PICP in responders and PICP:CITP ratio (type I collagen turnover) of ≥14.4 had greater than twofold increased chance of predicting functional response, driven by PICP. Critically, echocardiographic and clinical/functional response criteria correlate poorly,18 so could not be contrasted. Importantly, Lopez-Andres et al,8 the largest study included in the review, did not observe upregulation of collagen synthesis predicting echocardiographic non-response, which does challenge the Umar et al10 and Dong et al26 observations; however, the cohort characteristics and study designs were different. The observations of collagen synthesis following CRT implantation conflict with each other. Umar et al10 reported a significant increase in PINP and decrease in PIIINP expression in responders at 6 months; both would mechanistically be expected to be lower at follow-up. In contrast Garcia-Bolao et al9 observed PICP levels decreased for responders and increased for non-responders at 1 year, which would be expected, but is based on a functional response definition. In contrast to collagen synthesis, degradation biomarkers (ICTP or CITP) did not predict CRT response.8–10 Furthermore, no significant change in ICTP or CITP expression was observed at follow-up across all three studies.8–10 Alteration in collagen synthesis rate is observed to be more powerful at predicting response than collagen degradation. Different patterns of collagen synthesis biomarkers predicting response have been observed; lower expression predicted LV reverse remodelling,10 26 whereas higher rates predicted functional response.9 The variation in these patterns is explained by the different response definitions and cohort characteristics. The study cohort for Umar et al10 had a higher proportion of men and ischaemic cardiomyopathy than Garcia-Bolao et al.9 The heterogeneities between these studies make drawing conclusions difficult. Lopez-Andres et al8 also challenge any observations due to size of cohort and no prediction value to collagen turnover observed. Overall, collagen synthesis is observed to be important in predicting CRT response, especially LV reverse remodelling, with results replicated in two studies that lower rates predict LV reverse remodelling.10 26
MMP-1, MMP-2 and MMP-9 perform a critical role in myocardial collagen degradation and have been identified as being important prognostic markers in HF.11 13 27 Predictive value for CRT non-response (death or LVEF ≤35% at 18 months) was only demonstrated in baseline MMP-1 expression ≤3 ug/l8 supporting an observation by Jordan et al11 that lower MMP-1 inferred worse HF prognosis. MMP-2 had large variations observed between the included studies,8 24 but was not demonstrated to predict response. MMP-9 was only observed in one included study showing no predictive value9; however, recently Dini et al13 demonstrated raised levels (>238 ng/mL) and predicted worse HF outcomes. MMP activity was not considered in any of these studies as a predictor but would be important to consider in the future. Current evidence suggests that MMPs, especially MMP-2 and MMP-9, have not yet had their potential fully evaluated.
TIMP-1 regulates the endogenous proteolytic MMP system involving discordant inhibition and in chronic inflammatory states stimulating collagen synthesis and myocardial fibrosis.5 24 Tolosana et al24 observed a significant baseline difference in RvsNR expression with lower TIMP-1 in responders. Tolosana et al24 demonstrated that baseline TIMP-1 (≥248 ug/L) predicted CRT non-response. Trucco et al29 in long-term follow-up of the same cohort demonstrated that the same threshold independently predicted mortality at 60±34 months (sensitivity 80% and specificity 71%). Tolosana et al24 also demonstrated that statistically significant lower TIMP-1 is found in participants that do LV reverse remodel (LVESV reduction ≥10%). Umar et al10 and Garcia-Bolao et al9 observed no difference statistically at baseline. Variation between the reported literature in the magnitude of association of TIMP-1 exists; however, Tolosana et al24 offers a well-designed prospective observational study which is powered giving strength to the conclusions drawn.
Gal-3 stimulates fibroblasts to release TIMPs and MMPs that regulate collagen turnover, resulting in myocardial fibrosis.14 Elevated levels are independent predictors of adverse outcomes in HF.14 Evaluation of Gal-3 as a predictor of response was limited, as RvsNR was not reported in either of the two studies.8 25 Truong et al25 demonstrated peripheral baseline Gal-3 ≥25.9 ug/L had specificity for predicting CRT response. Lopez-Andres et al8 observed Gal-3 baseline expression ≥30 ng/L had nearly threefold increased risk of death or hospitalisation for worsening HF following CRT. Though not demonstrated to be a strong predictor, the evidence suggests that Gal-3 is a good biomarker for predicting poor outcomes in HF and needs further evaluation.
The greatest challenge for research into CRT response and one this review demonstrated is lack of an accepted response definition. Differing definitions rarely correlate,18 which our review clearly demonstrates. Echocardiographic and clinical/functional definitions correlate very poorly and should never be compared or applied in a composite definition18; LV reverse remodelling should be considered separately.18 30
Study limitations
Heterogeneity among included studies was widespread despite a rigorous eligibility and screening criteria. The variations in study design, cohort characteristics and response definitions made pooling data in a meta-analysis impractical. CRT implantation techniques and indications have evolved over the last 15 years and offer another source of heterogeneity. Furthermore differences in laboratory techniques account for some variation among biomarker results. These limitations are particularly important to consider in future research studies.
Conclusions
Collagen synthesis biomarkers have shown the most potential, particularly PINP and PIIINP, but will require further study. MMP-2 and MMP-9 have no conclusive predictive value and need further investigation. Heterogeneity is the greatest challenge for research in this field and needs to be minimised in future studies. The most important initial step is for a universal response definition to be adopted and applied.
Acknowledgments
We would like to acknowledge the Research, Development and Innovation department for their support, Medical and Life Science Fund (charity no. 1139383) for their kind support of Dr C McAloon, Petra Meeson and the University Hospital Coventry and Warwickshire library services for their assistance with the literature search, Professor Norman Waugh in Warwick Evidence for reviewing and offering his expert advice.
References
Footnotes
Contributors CJM had the original concept, designed methodology, performed literature search, article screening, data extraction, quality assessment, results analysis and drafted the manuscript. DA performed article screening, data extraction and quality assessment. TH reviewed statistical interpretation. PB, POH and HR reviewed methodology and critically edited manuscript. FO reviewed methodology, eligibility and critically edited manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.