Article Text

Abstract
Objective The dual-therapy stent combines an abluminal biodegradable drug-eluting coating, with a ‘pro-healing’ luminal layer. This bioengineered layer attracts circulating endothelial progenitor cells that can differentiate into normal endothelium. Rapid endothelialisation of the stent might allow safe short dual antiplatelet therapy. We aim to assess clinical outcomes in patients treated with this novel device at 2-year follow-up.
Methods A total of 1000 patients were included in the REMEDEE Registry to evaluate clinical outcomes after treatment with the dual-therapy stent. This prospective, multicentre, European registry included all-comers patients, which resulted in a high-risk patient population. Target lesion failure (TLF), a combined endpoint consisting of cardiac death, target vessel myocardial infarction (tv-MI) and target lesion revascularisation (TLR), at 2-year follow-up was the primary focus of this analysis. Subgroup analyses were performed according to diabetes mellitus (DM), gender, age, acute coronary syndrome, smoking, hypertension, hypercholesterolaemia, previous stroke, peripheral vascular disease and chronic renal failure.
Results TLF at 2 years was observed in 84 patients (8.5%), with 3.0% cardiac death, 1.2% tv-MI and 5.9% TLR. Definite stent thrombosis at 2 years was 0.6%. In the presence of DM or chronic renal failure, a higher TLF was observed.
Conclusions The dual-therapy stent shows favourable clinical outcomes from 12 months onwards. Two years after stent placement, low TLF and very low stent thrombosis rates are observed in this large prospective all-comers cohort study.
Trial registration number NCT01874002; Results.
- Coronary Artery Disease
- Interventional Cardiology
- Coronary Intervention (pci)
- Coronary Stenting
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Preclinical research showed early endothelialisation with this dual-therapy stent technology. One-year clinical results of the 1000 patient registry have been reported with low event rates.
What does this study add?
There is a need for long-term clinical follow-up of novel coronary devices. This large prospective, investigator-initiated, all-comers cohort evaluates the real-world clinical performance of this dual-therapy COMBO stent at 2 years after stent placement. Low event rates are observed at 2-year follow-up.
How might this impact on clinical practice?
The dual-therapy stent shows good 2-year clinical results and might be the preferred treatment strategy in patients with coronary artery disease, and especially in patients with indication for short dual-antiplatelet therapy. Randomised trials are needed to support this hypothesis.
Introduction
Innovations in the field of drug-eluting coronary stent (DES) therapy are rapidly evolving. First-generation DES improved outcomes in terms of reduced rates of restenosis compared with bare metal stenting.1 2 Subsequently, second-generation DES, with thinner stent struts, limus analogue drugs and more biocompatible polymers, were designed to reduce the increased risk of late clinical events of DES.3–5 The controversial term ‘third-generation’ DES is attributed to DES with newer (fully) biodegradable polymers and polymer-free DES. These stents and also the bioabsorbable scaffolds try to minimise adverse outcomes.6–8 However, no device has been able to eliminate in-stent neointimal hyperplasia, neoatherosclerosis and/or (very) late stent thrombosis (ST).
The COMBO stent (OrbusNeich Medical, the Netherlands) is the first dual-therapy stent (DTS), which combines the ‘traditional’ drug-eluting therapy (sirolimus in a biodegradable polymer) with an immobilised CD34 antibody that captures endothelial progenitor cells (EPCs) from the circulation (figure 1). These EPCs can differentiate into endothelial cells on the luminal surface of the stent.9 The hypothesis of this ‘pro-healing’ technique is that it may offer not only improved clinical outcomes, but also safe short use of dual-antiplatelet therapy (DAPT).10 11
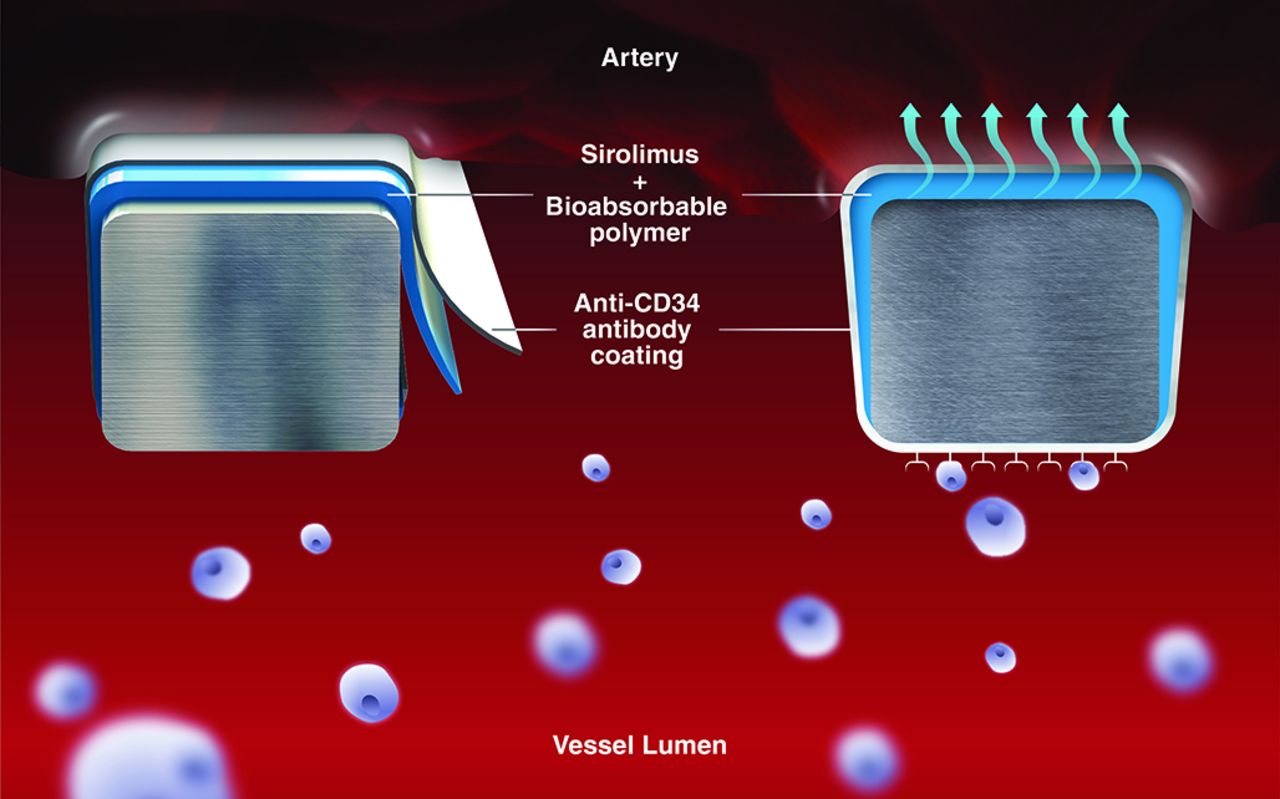
The COMBO stent design, illustration of the dual-therapy stent technology.
The REMEDEE Registry (all acronyms are presented in the online supplementary file 1) aims to provide more insight into the clinical outcomes with the COMBO stent in routine clinical practice and in an all-comer setting. Currently only limited long-term data are available on clinical results with the COMBO DTS exceeding 1 year.12 In this paper, we evaluate 2-year clinical results of the REMEDEE Registry and analyse outcomes in different patient subgroups.
Supplementary file 1
Methods
Registry design and patient population
The study design of the REMEDEE Registry (NCT01874002) has been previously published.13 In brief, the REMEDEE Registry is an investigator-initiated, prospective, European registry evaluating the first DTS, the COMBO stent. A total of 1000 patients, in whom treatment with a COMBO stent in the setting of routine clinical care was attempted, were enrolled. DAPT was prescribed according to local guidelines. With only few exclusion criteria, a true all-comers patient population was targeted. At 30 days, 180 days, 1-year and 2-year follow-up, all patients were contacted for clinical follow-up by telephone call or during a scheduled outpatient clinic visit. All event documentation was collected and all events were adjudicated by an independent clinical event committee.
Endpoints and definitions
In this 2-year follow-up analysis of the REMEDEE Registry, we evaluate target lesion failure (TLF), which is defined as the composite of cardiac death, target vessel myocardial infarction (tv-MI) or target lesion revascularisation (TLR). Tv-MI was defined as all myocardial infarctions (MIs) unless in the presence of documented proof that the infarction arose from a non-treated coronary vessel. TLR was defined as any repeat revascularisation by percutaneous intervention of the treated lesion or coronary artery bypass grafting (CABG) of the treated vessel. Secondary endpoints were the individual components of the primary endpoint, target vessel failure (TVF) and ST at 2-year follow-up. TVF was defined the composite of cardiac death, tv-MI and target vessel revascularisation (TVR). TVR was defined as target vessel revascularisation (any revascularisation of the treated vessel by percutaneous coronary intervention (PCI) or CABG). ST was defined according to the Academic Research Consortium criteria.14
Statistical analysis
Categorical data are shown with counts and percentages, continuous variables are in mean ± SD, unless otherwise mentioned. For time-to-event data, Kaplan-Meier estimates were used for all endpoint analyses. Follow-up was censored at the last known date of follow-up, or at 24 months, whichever came first. A lost to follow-up rate of <2% a year was deemed acceptable. All endpoints were evaluated in the unselected patient population, which consisted of all patients who were enrolled after signing an informed consent and in whom placement of a COMBO stent was attempted. Cox regression analysis was done to calculate HRs for diabetes mellitus (DM) status, gender, age, acute coronary syndrome (ACS), smoking, hypertension, hypercholesterolaemia, past stroke, peripheral vascular disease and chronic renal failure. Statistical analyses were performed using SPSS V.23.0.
Results
Baseline characteristics
Between June 2013 and March 2014, 1000 patients were enrolled in nine European sites. The baseline characteristics are presented in table 1. The mean age during baseline procedure was 65±11 years and 26.1% of patients were female. At baseline, 58.0% of the patients had a history of hypertension and 18.4% were diabetic. The registry included 30.4% of patients with an urgent indication for PCI. TIMI flow 0 was observed in 14.5% of patients and thrombus was present in 15.0% of the cases. In two patients, the COMBO stent could not be placed. Mean stent length was 21.4±10.5 mm and mean diameter 3.2±0.5 mm.
Baseline characteristics
Clinical outcomes
Two-year follow-up was obtained for 981 patients (98.1%). Events observed at 2 years after COMBO stent placement are listed in table 2. TLF occurred in 84 patients (8.5%), as illustrated in the Kaplan-Meier curve of events found in figure 2. Cardiac death was observed in 3.0% of patients (n=30), tv-MI in 1.2% (n=12) and TLR in 5.9% (n=58) (figure 3). In four of the five cases of very late tv-MI, angiography was performed which did not show ST of COMBO, the fifth tv-MI was in a patient presenting with dyspnoea and decompensatio cordis, without chest pain but classified as non-ST-segment elevation MI. Echocardiography showed diffuse impaired LV function. Regional wall abnormalities could not discriminate location of MI; therefore, the CEC classified as tv-MI. Due to absence of ST-segment elevation on inferior leads (COMBO in right coronary artery), the possibility of an ST was found less likely by the CEC.
Clinical endpoints at 1-year and 2-year follow-up

Cumulative event rate of target lesion failure by Kaplan-Meier method.

Cardiac death, target vessel myocardial infarction (MI), target lesion revascularisation (TLR) by Kaplan-Meier method. (A) Cumulative event rate of the individual endpoint cardiac death. (B) Cumulative event rate of the individual endpoint target vessel-related MI. (c) Cumulative event rate of the individual endpoint TLR.
A total of 70 patients underwent TVR (7.1%), resulting in a 9.7% TVF at 2 years. Definite ST at 2 years occurred in six patients (0.6%). Five patients had ST within the first nine days post procedure, one patient with ACS had a very late ST at 380 days, shortly after DAPT cessation.
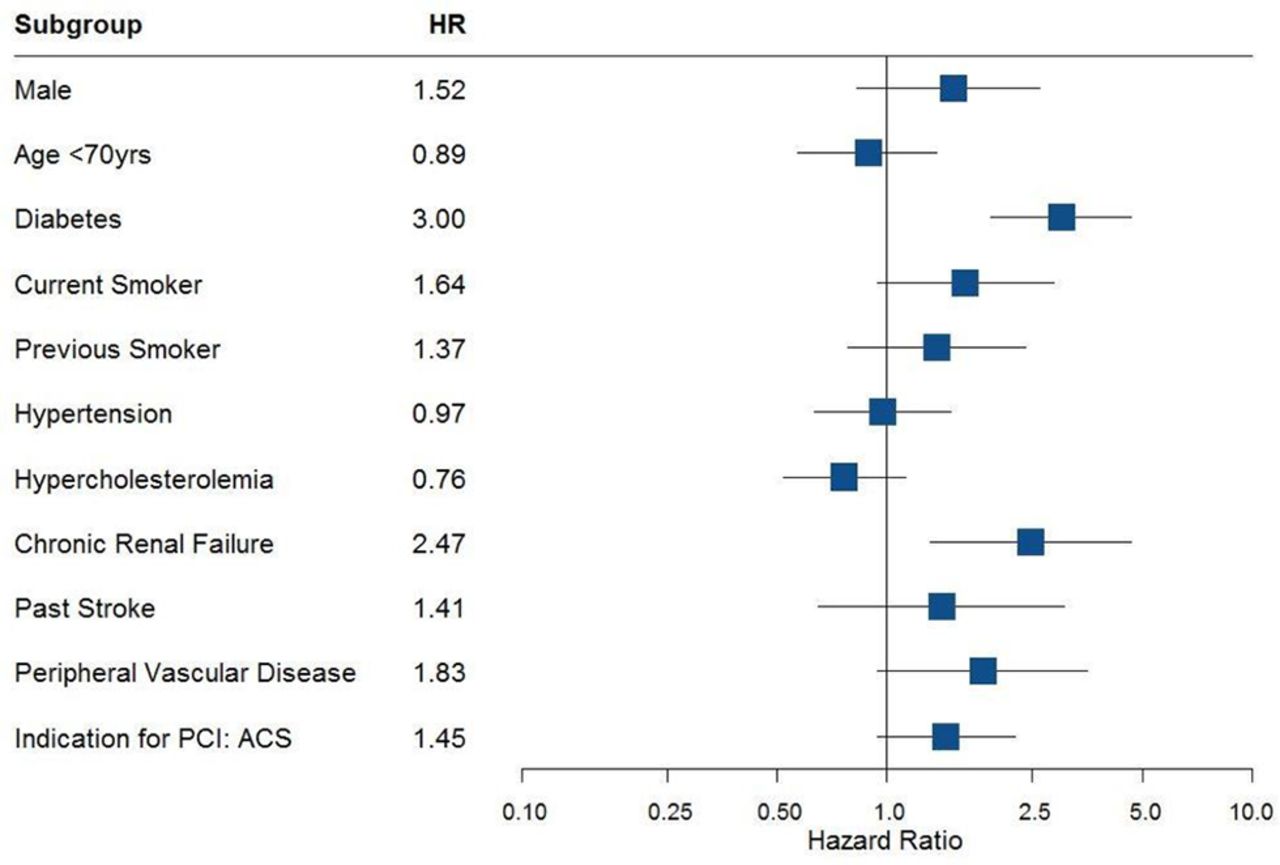
The influence of baseline patient characteristics (gender, age, cardiovascular risk factors, ACS, peripheral vascular disease and chronic renal failure) on 2-year clinical outcome is shown in figure 4. The only significant univariate predictors of TLF were diabetes HR 3.00 (95% CI 1.93 to 4.66) and chronic renal failure HR 2.47 (95% CI 1.31 to 4.67), although trends were seen with current smokers, ACS and peripheral vascular disease.
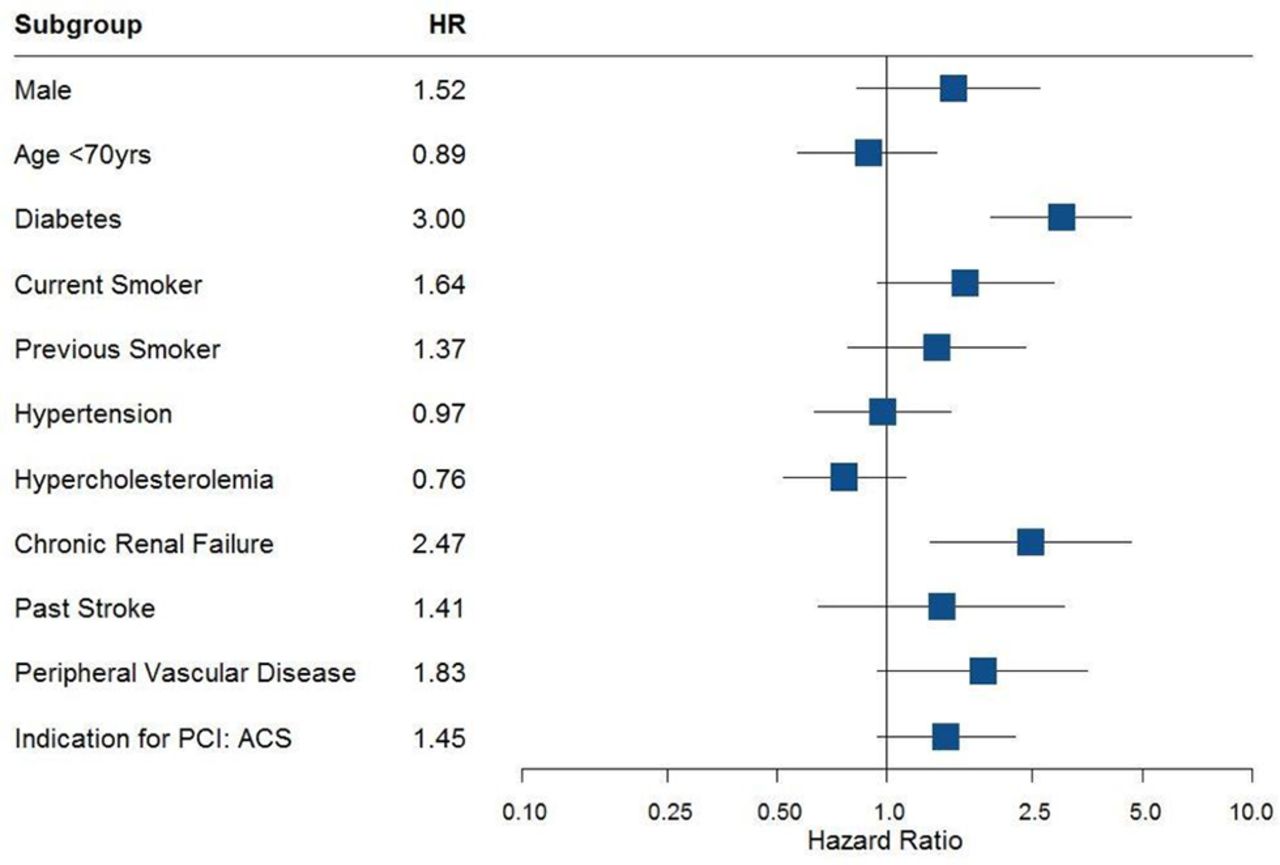
Subgroups. HR of gender, age, diabetic status, smoking (current and previous), hypertension, hypercholesterolaemia, chronic renal failure, previous stroke, peripheral vascular disease and acute coronary syndrome (ACS) on target lesion failure at 2-year follow-up. PCI, percutaneous coronary intervention
Discussion and limitations
Key findings
This study reports the clinical outcomes up to 2-year follow-up in a large prospective, all-comers cohort of patients treated with the COMBO stent. We found (1) low rates of clinical events observed at 2 years after COMBO DTS implantation with an overall low percentage of the primary endpoint TLF of 8.5% and very late ST in only one patient (0.1%), (2) our subgroup analyses found that the COMBO DTS gave favourable results in several high-risk patient groups although higher rates of TLF were observed at 2 years in patients with DM and chronic renal failure higher rates of TLF,and (3) the rate of TLR between 1 and 2 years follow-up was very low.
Clinical implications
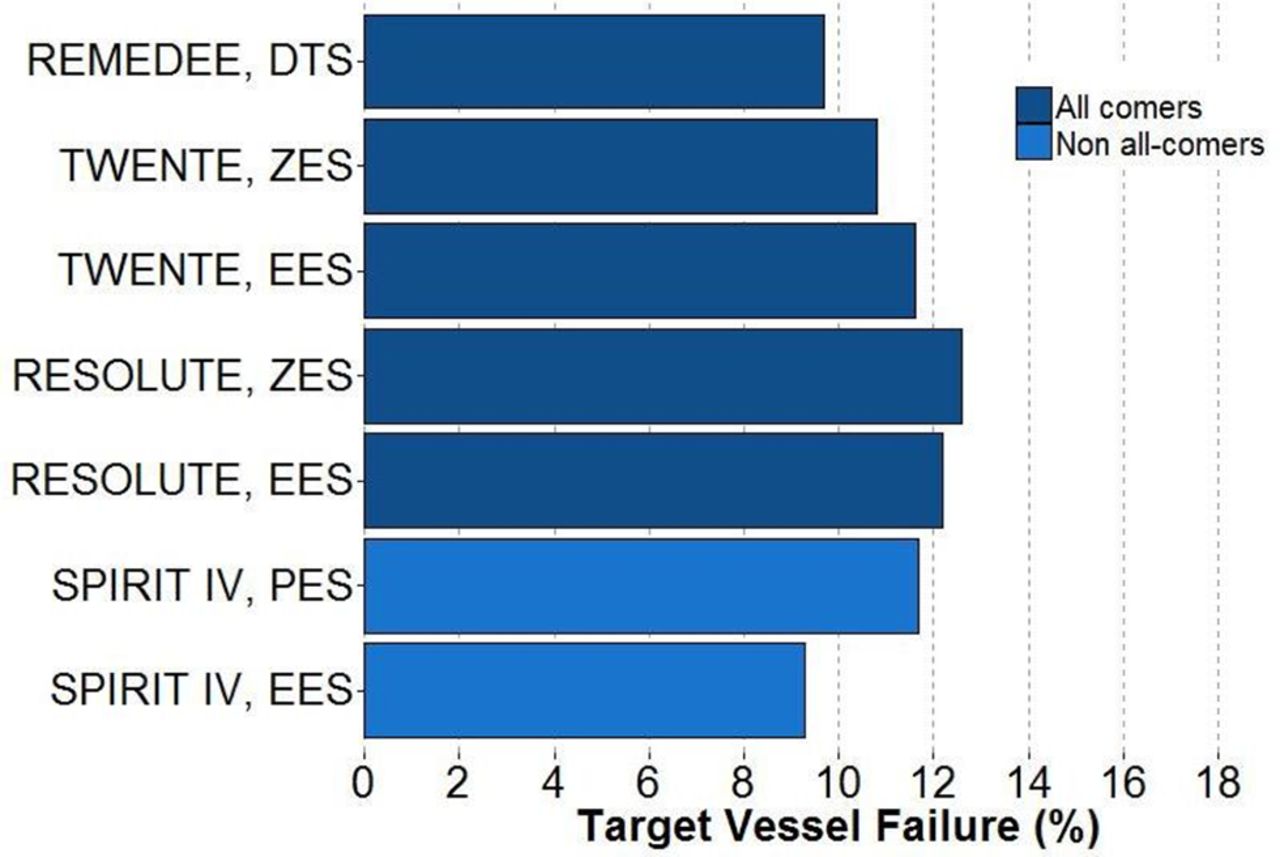
Currently only limited data are available on clinical outcomes with the COMBO DTS exceeding 1-year follow-up.12 The results presented in this study are in line with other newer-generation DES (see figure 5) such as the all-comers TWENTE15 and RESOLUTE (see online supplementary file 1)16 trials which compared a zotarolimus-eluting stent (ZES) (RESOLUTE, Medtronic, USA) with an everolimus-eluting stent (EES) (XIENCE V, Abbott Vascular, USA). In addition, compared with the 2-year outcomes of the more selected patient population SPIRIT IV trial, comparing a paclitaxel-eluting stent (PES) (TAXUS, Boston Scientific, USA) with an EES (XIENCE, Abbott Vascular, USA), reported similar outcomes.17
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of target vessel failure at 2-year follow-up with other drug eluting stents (DES). DTS, dual-therapy stent; EES, everolimus-eluting stent; PES, paclitaxel-eluting stent; ZES, zotarolimus-eluting stent.
ST in the REMEDEE Registry was reassuringly low despite the all-comers design. In particular, very late ST (between 12 and 24 months) occurred in only 0.1% of patients receiving the COMBO stent (which is lower than with the other devices above; EES varies 0.1–0.3, ZES 0.3% and PES 0.2%).15–17 A recent meta-analysis by Nairooz et al reports a 2-year ST rate of the bioresorbable vascular scaffold of 2.1%.18 The low ST rate at 2 years with the COMBO stent is a significant finding supporting the DTS technology hypothesis of low ST risk due to early endothelialisation of the stent, but caution should be taken and randomised data are needed to confirm these findings.
Neointimal regression
A recent study evaluating the healing pattern of the COMBO stent at 4-monthly groups (1:2:2:1 ratio from 2 to 5 months), 9 months and 24 months showed a new phenomenon not described earlier with any other DES: neointimal regression visualised by optical coherence tomography between 9 and 24 months.12 This intimal hyperplasia regression has also been assessed by quantitative coronary analyses previously in the Genous stent (OrbusNeich, a BMS with EPC capturing layer).19 These consistent findings may support the hypothesis of the beneficial effect of rapid endothelialisation and healthy maturation of the endothelial layer by means of EPC capture by the immobilised CD34 antibody at the stent surface. This study showed low TLR rate between 1 and 2 years (from 4.3% to 5.9%; a 1.6% increase). Moreover, these results emphasise the need for evaluation of long-term clinical results, exceeding 1-year follow-up, to make the true comparison of performance of the DES.
Subgroups
DM is a known risk factor for higher adverse outcome after PCI.20 21 We published 1-year clinical outcomes after COMBO stent placement of insulin-treated DM, non-insulin-treated DM and non-DM patients, with a clear signal of higher TLF in insulin-treated DM.22 Although patients with chronic kidney disease (CKD) often have DM, after multiple regression analyses in the DM group at 1 year, CKD was also independently associated with higher TLF. Clinical outcomes of patients with CKD and stent placement should further be explored.
Future perspectives
The REMEDEE Registry will evaluate patients up to 5 years after COMBO stent placement, and thereby, will give further insight into the long-term treatment effect of DTS technology with COMBO. Currently the US–Japan randomised HARMONEE trial (see online supplementary file 1), which evaluates clinical outcomes between EES (XIENCE family, Abbott Vascular) versus COMBO, awaits completion of 1-year follow-up. This study will also obtain clinical follow-up up to 5 years too.
Limitations
The main limitation of the REMEDEE Registry was the single-arm design. However, data collection was undertaken with great care to ensure optimum data quality. On-site monitoring and full-event documentation were collected for independent adjudication by the clinical event committee. Another limitation of the registry design is that the DAPT duration was not mandated by the registry’s protocol; therefore, the majority of patients received DAPT for 1 year. A potential benefit of the COMBO DTS would be illustrated more clearly if a short duration of DAPT (eg, <6 months) after COMBO stent placement would show the same low ST rates. However, this study is the first large cohort to report on long-term results after COMBO stent in an all-comer patient population and provides new insight into the performance of DTS.
Conclusion
Two-year clinical results with the COMBO stent in the 1000 subject REMEDEE Registry have shown low rates of TLF, TVF and ST. These results confirm the long-term clinical effectiveness of DTS technology in an all-comers patient population.
Acknowledgments
All patients, catheterisation laboratory nurses and interventional cardiologists are greatly acknowledged for their participation and efforts regarding the REMEDEE Registry. The authors especially acknowledge Margriet Klees for all her efforts regarding the REMEDEE Registry.
References
Footnotes
Contributors DNK and PW contributed to the conception, design, analysis and interpretation of data and drafting of the manuscript and final approval of the manuscript submitted. IBAM, PdH, AWJvH, AE, HS, KEA, AI, PM, and MAMB contributed to the conception and design of data and revising manuscript critically for important intellectual content and final approval of the manuscript submitted. JGT and RJdW contributed to the conception, design, analysis and interpretation of data and drafting of the manuscript and revising manuscript critically for important intellectual content and final approval of the manuscript submitted.
Funding The Academic Medical Center, University of Amsterdam received an unrestricted research grant from OrbusNeich Medical B.V., the Netherlands.
Competing interests None declared.
Patient consent Obtained.
Ethics approval A waiver was obtained from the ethics committee of the Academic Medical Center, University of Amsterdam.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The relevant anonymised patient-level data are available on reasonable request to the corresponding author.