Article Text

Abstract
Background Early identification and treatment of cardiovascular risk factors (CVRFs) is essential to prevent excess morbidity, mortality and healthcare-related costs. We sought to investigate whether an active screening programme at pharmacies could identify a significant proportion of patients with previously undetected CVRFs.
Methods and results Between April and July 2013, 184 pharmacies in Lower Austria enrolled a total of 6800 participants, in whom body mass index (BMI), blood pressure (BP), total cholesterol and blood glucose were measured. Mean age was 58±17 years and 67.8% were women. 21% of men and 16% of women had a BMI≥30 kg/m2. The crude prevalence of diabetes mellitus (DM) was 7%, hypercholesterolaemia was identified in 57%, and 44% had elevated BP. Among fasting individuals (n=1814), DM was found in 18%. In total, 30% were confronted with a CVRF they were previously unaware of, and pharmacists recommended 45% of all participants to actively consult a physician. A first-time diagnosis of a CVRF was most frequent in the age groups between 25 and 64 (32% of participants).
Conclusions This pharmacy-based approach for cardiovascular risk screening found similar overall prevalences of CVRFs as reported by national surveys, but revealed underdiagnoses, particularly in lower age groups. A previously unknown CVRF was identified in every third individual, frequently prompting the pharmacists to recommend the consultation of a physician. An active screening approach at pharmacies might therefore serve as an effective alternative to the public preventive medical examination, particularly in younger age groups.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Screening programmes for cardiovascular risk factors are poorly implemented into primary care, subsequently leading to a preventable excess in morbidity and mortality. Previous small studies not covering all major risk factors could show that pharmacies are feasible sites for screening.
What does this study add?
The present study is one of the largest covering all major cardiovascular risk factors by instrument-based tests. One of the three participants was confronted with a major cardiovascular risk factor they were previously unaware of. The feasibility of this pharmacy-based approach is also underlined by a large sample that could be included in a short period of time.
How might this impact on clinical practice?
A pharmacy-based screening approach might serve as an effective alternative to a public preventive medical examination in primary care, especially in younger age groups. Implementation into a national disease management programme would be required to achieve a population-based impact.
Introduction
The well established and potentially modifiable risk factors for cardiovascular (CV) morbidity hypertension (HTN), dyslipidaemia, diabetes mellitus (DM), obesity, improper diet and lack of regular physical activity account for 90% of population-attributable risk for both, stroke1 and myocardial infarction.2 In other words, a dramatic 90% reduction of these events would be observed if the population were entirely unexposed to the mentioned risk factors.
At present, these risk factors remain frequently unrecognised for years since screening programmes are poorly implemented into primary care, while screening for malignancies such as breast cancer, colorectal cancer or prostate cancer are widely accepted, actively offered and routinely performed in Western countries.2–4 In Austria, ∼13% of adults attend the annual, public and cost-free preventive medical examination.5 The transition from elevated CV risk to a manifest disease can be massively influenced by early identification and tight control of risk factors, which further underlines the relevance of active screening.6
Accordingly, we sought to investigate whether a standardised, active screening programme for CV risk factors (CVRFs) at pharmacies could identify a significant amount of previously unknown CVRFs.
Methods
Study design and participants
This cross-sectional study enrolled individuals who visited a participating pharmacy in Lower Austria between April and July 2013.
The Pharmacists College of Lower Austria, a province with a population of 1.6 million, invited all members (239 pharmacies) to participate.
There were no age-related or other inclusion/exclusion criteria prespecified. All participants provided informed consent, and only anonymised data were collected. In individuals below the age of 18, parental or guardian permission was obtained additionally.
All participating centres underwent investigator training where the study protocol, data collection as well as proper blood pressure (BP), glucose and cholesterol measurement were reviewed.
Using a standardised questionnaire, the following variables were assessed: age, gender, height, weight, waist circumference, fasting at the time of survey (8 hours without intake of food or liquids, except for water), tobacco use, seated BP, total cholesterol and capillary blood glucose. Individuals were surveyed whether a new CVRF was identified previously unknown to the participant (including conditions requiring an instrument-based test, thus, impaired fasting glucose (IFG), diabetes, elevated BP or hypercholesterolaemia; not including smoking and obesity). It was at the discretion of pharmacists to recommend the respective participant to actively consult a physician based on the detected CVRFs, and this decision was recorded in the survey.
Diagnostic evaluations
In accordance with the 2003 European Society of Hypertension (ESH)/European Society of Cardiology (ESC) Guidelines for the management of arterial HTN pharmacists were instructed to allow participants to sit for 3–5 min before beginning BP measurements and to take repeated measurements in case of inconsistent values.7 All pharmacists were experienced in the measurement of BP. An oscillometric semiautomatic sphygmomanometer was used at all sites (Boso Medicus, Jungingen, Germany or Hartmann Tensoval, Wiener Neudorf, Austria).
Total cholesterol and capillary blood glucose were measured locally using point of care devices (Accuntrend plus and Accu Chek Performa, Roche Diagnostics, Austria).
Waist circumference was measured midway between the uppermost border of the iliac crest and the lower border of the costal margin, obtaining the greatest possible circumference in expiration.
Statistical analysis
Discrete characteristics are expressed as frequency counts and percentages, and differences between groups were determined by the χ2 test. Continuous, normally distributed variables were expressed as means with SDs, unless otherwise specified. Differences were examined using the Student’s t-test or the Mann-Whitney test, where appropriate. Correlations were reported as Spearman’s coefficient. The level of significance used for all tests was a two-sided p value of 0.05.
The Software Package for Social Sciences V.22 (SPSS, Chicago, Illinois) was used for all statistical calculations.
Outcome measures
Obtained outcomes are reported for the whole cohort as well as according to gender and the prespecified age groups <45, 45–64 and >64 years.8
In accordance with the 2013 ESH/ESC Guidelines for the management of arterial HTN, elevated office BP was reported at a threshold of ≥140 mm Hg systolic (SBP) and ≥90 mm Hg diastolic (DBP).9
On the basis of the 2011 ESC/European Atherosclerosis Society (EAS) guidelines, hypercholesterolaemia was reported at a threshold of ≥200 mg/dL (5.2 mmol/L).10
According to the 2013 ESC Guidelines on diabetes, pre-diabetes and CV diseases (CVD), fasting capillary glucose values ≥101 mg/dL (5.6 mmol/L) and ≥117 mg/dL (6.5 mmol/L) were indicative of IFG and manifest DM, respectively. In non-fasting patients, glucose levels ≥200 mg/dL (11.1 mmol/L) were regarded for the diagnosis of DM.11
Abdominal obesity was reported in the presence of a waist circumference ≥100 cm for men and ≥90 cm for women.
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in an approval by the Institution's Human Research Committee.12
Results
From 239 pharmacies in Lower Austria, 184 (77%) participated in the recruitment of patients. In total, 6800 patients were included between April and July 2013, reflecting a recruitment of 36.9±43.5 patients per site. The mean age was 58±17 years, 67.8% were women. Twenty-two per cent of participants were below 45 years of age.
The mean BP was 134±21/81±12 mm Hg, mean capillary glucose 112±29 mg/dL (not account for fasting status), and mean total cholesterol was 210±43, respectively (table 1).
Clinical characteristics of the cohort, stratified by gender
Obesity
As presented in table 2, 48% of women and 66% of men were overweight (body mass index (BMI) ≥25 kg/m2) or obese (BMI≥30 kg/m2). For both genders, the correlation between BMI and waist circumference was significant (rs=0.79, p<0.01 for women, rs=0.76, p<0.01 for men). By use of the aforementioned cut-off values, the prevalence of abdominal obesity was similar between the genders (49.3% vs 49.5%, p=0.89, waist circumference women 89.9±13.8, men 99.4±12.7).
The prevalence of CVRFs, stratified by gender
Diabetes mellitus
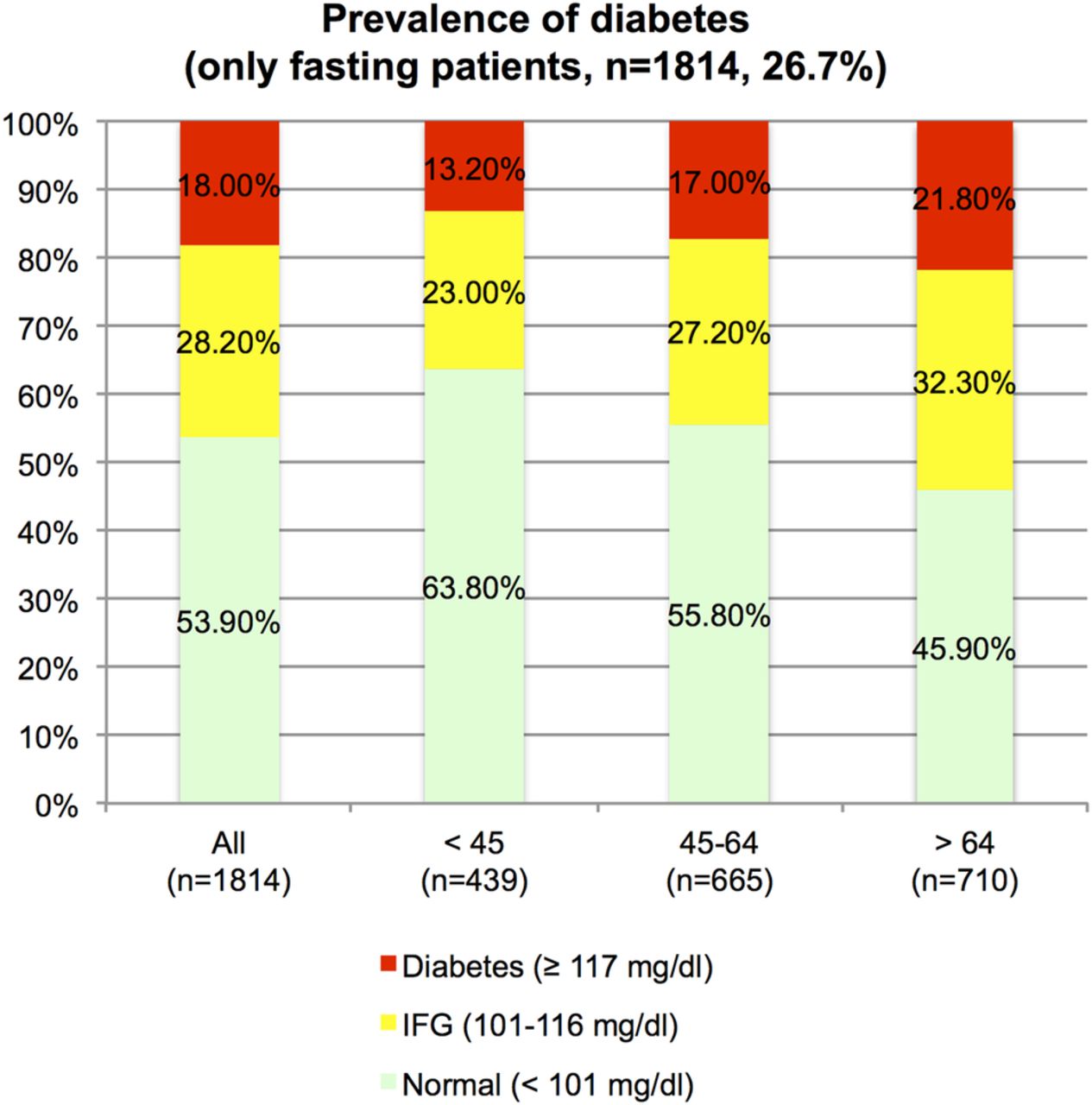
Fasting and non-fasting participants were similar regarding age (57.3±17.2 vs 58.2±17.4, p=0.06), gender (p=0.29), BMI (p=0.49), waist circumference (p=0.17 for men, p=0.59 for women), total cholesterol (p=0.13), and DBP (p=0.41), but not SBP (136.9±22.3 vs 133.6±20.4, p<0.01). Mean capillary glucose was 114.4±30.1 vs 103.7±22.1 mg/dL in non-fasting and fasting participants, respectively. Considering only fasting individuals (n=1814), IFG and manifest DM were found in 28% and 18% of participants, respectively.
As indicated in figure 1, there was a stepwise increase in the prevalence of DM with each age group, reaching 22% for fasting participants aged 65 and above (p for trend <0.01).

The prevalence of impaired fasting glucose (IFG) and diabetes mellitus in fasting participants (capillary glucose values).
When taking the full cohort in to account, manifest DM (capillary glucose ≥200 mg/dL (11.1 mmol/L) in non-fasting participants) was observed in 6–8% of individuals (table 3).
The prevalence of CVRFs according to prespecified age groups
Elevated BP
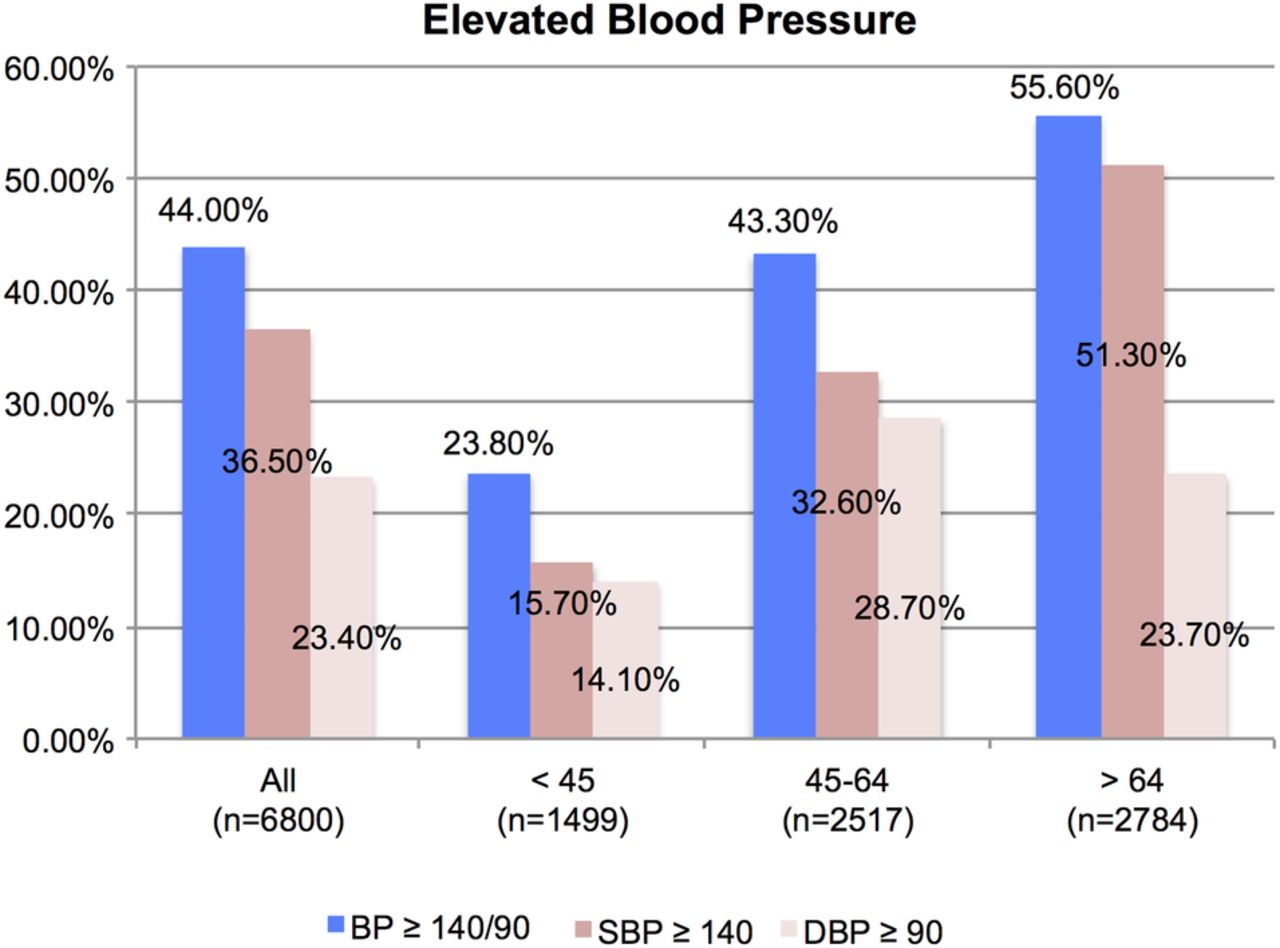
Elevated BP was infrequent below the age of 25, and absolute BP values were only modestly increased in individuals exceeding the BP threshold in this age group (144±19/87±12 mm Hg, figure 2). Thereafter we observed a steep increase in the prevalence of uncontrolled HTN, affecting every second patient ≥45 years of age. In these uncontrolled patients, mean BP values were 153±16/89±12. Two-thirds remained in HTN grade 1, that is, below 160/100 mm Hg. The increase in pulse pressure, that is, decline of DBP was observed starting at an age of 63 (p for trend <0.01).

The proportion of participants with elevated BP values at a threshold of ≥140/90 mm Hg. BP, blood pressure; DBP, diastolic blood pressure; SBP, systolic blood pressure.
Hypercholesterolaemia
The crude prevalence of hypercholesterolaemia was 57%.
Seventeen per cent of predominantly non-obese participants below the age of 25 had total cholesterol levels above 200 mg/dL (5.2 mmol/L).
The peak prevalence of 65% was seen in the age group between 45 and 64 years (mean total cholesterol 217±42 mg/dL), declining thereafter (figure 3). Data on cholesterol-lowering treatment in the respective subgroups were not available.
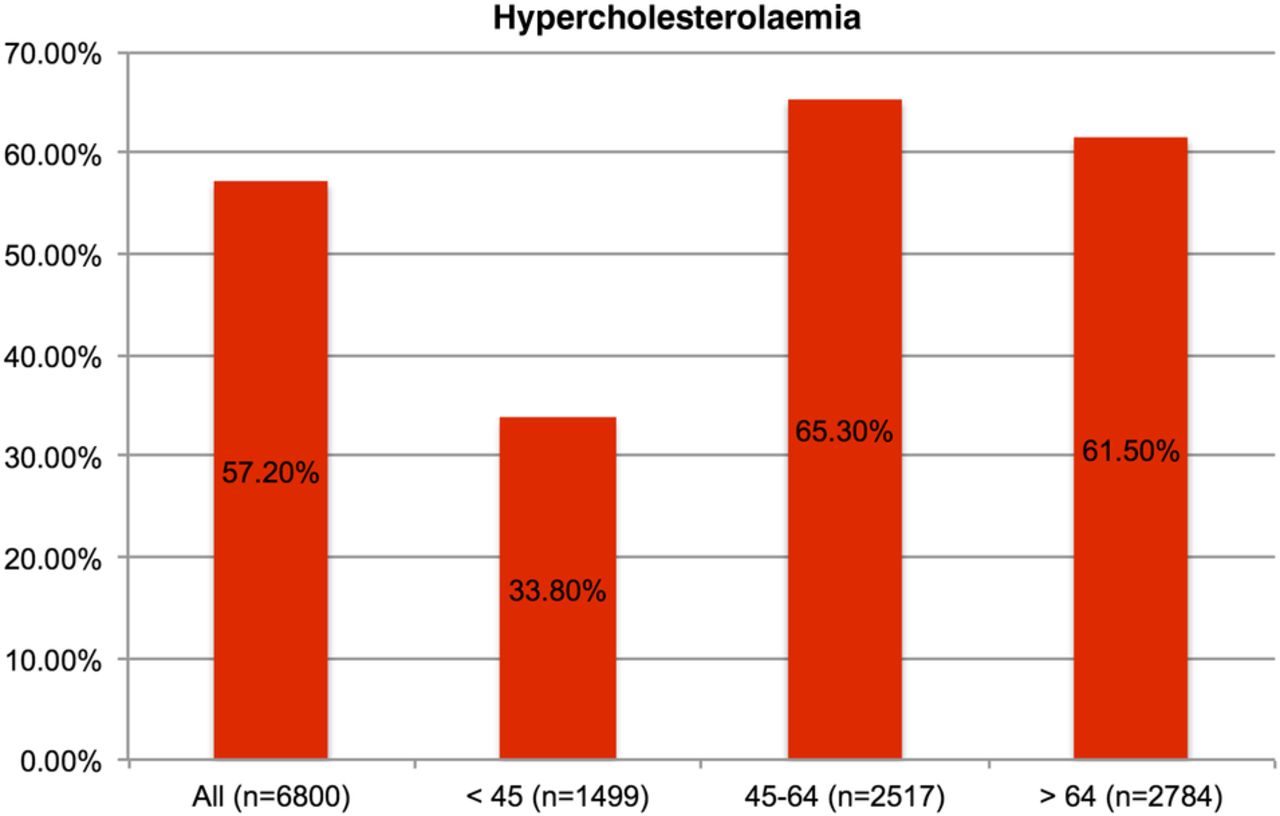
The prevalence of hypercholesterolaemia at a threshold of 200 mg/dL (5.2 mmol/L).
Smoking
Ten per cent of minors reported to be active smokers; however, the sample size was non-representative (n=70) in this age group. The prevalence of tobacco use was stable at a high level (35%) in participants between 18 and 44 years of age, and men were somewhat more likely to report smoking compared with women (tables 2 and 3, 39% vs 33%, p=0.03). This trend continued in participants ≥45 years at a lower overall prevalence (15% vs 13%, p=0.02).
Total CV risk and identification of previously unknown risk factors
The survey question regarding newly identified CVRFs related to the instrument-based parameters BP, glucose and cholesterol levels, but excluded smoking and obesity, since the latter did not require a specific screening test performed by a healthcare professional for diagnosis.
At least one of these four major CVRFs (IFG, DM, elevated BP or hypercholesterolaemia) was present in 75% of individuals, similarly frequent in men and women (p=0.54, table 2). Excluding IFG, a CVRF was present in 73.1% of participants.
Therefore, a new CVRF previously unknown to the participants was identified in 30% of cases and 45% of the cohort subsequently received a recommendation to actively consult their physician (figure 4, tables 2 and 3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The proportion of patients confronted with a cardiovascular risk factor (CVRF) they were previously unaware of, referring to the instrument based tests (impaired fasting glucose, diabetes, elevated blood pressure and hypercholesterolaemia).
When only considering the three CVRF likely requiring pharmacological treatment, hence, excluding IFG, a new diagnosis was established in 28%.
A first-time diagnosis of a CVRF was numerically most likely in the age groups between 25 and 64 (32% of participants), but still frequent above 64 years (27% of participants).
Discussion
The main finding of our study is that, first, this pharmacy-based approach was able to include a broad population sample in order to identify individuals with previously undiagnosed CVRFs. Overall 30% of participants were confronted with a CVRF they were previously unaware of, which frequently prompted the pharmacists to recommend an active consultation of a physician. In particular, participants aged between 25 and 64 years gained the greatest benefit in terms of a newly diagnosed CVRF.
Second, this is one of the largest studies assessing all major CVRFs by instrument-based tests at pharmacies, and the first one in Austria.13
Previous studies included mostly <600 individuals, with heterogeneous results regarding referrals and uptake of referrals, ranging between 6–73% and 13–83%, respectively.13 Overall, the pharmacy-based screening approach was found to be feasible.13 In line with our results, the strategy might serve as an easily accessible alternative to the voluntary public preventive medical examination, undertaken by 13% of adults annually in Austria.5 Very recently, the RxEACH study recruited 723 patients at high risk for CVD at pharmacies and randomly allocated them to usual care or an intervention, including diagnostic (laboratory) and therapeutic measures. After 3 months, there was a significant 21% reduction in risk for CVD events through improvements in cholesterol, BP and glycated haemoglobin. The authors concluded that expanding the pharmacists’ scope of practice could have significant public health implications.14
The crude prevalence of CVRFs was similar to those reported by national surveys, but we observed a substantial likelihood for underdiagnosis in lower age groups.5 ,15 ,16
In the Austrian Health Interview Survey (ATHIS) the prevalence of diabetes was indirectly assessed by the question ‘Have you been suffering from diabetes in the past 12 months?’. In the age groups between 45 and 59 years 5% (17% in our study, fasting patients), and in the age group ≥60 years 12% (20% in our study, fasting patients) responded positively to this question.15 The mismatch between diagnosed and undiagnosed diabetes was previously outlined by the National Health and Nutrition Examination Survey (NHANES), where, almost identical to our results, DM was identified in 20.9% above the age of 60.17
Also, our study underlines the striking difference between the self-reported (4%) versus directly assessed (24%) prevalence of elevated BP below 45 years of age, thus, the likelihood of underdiagnosis of HTN particularly in lower age groups.15 We could recently show that in diagnosed, treated and adherent patients approaching a pharmacy in order to obtain their antihypertensive medication, optimal BP control was achieved in only 41% of patients.18 Accordingly, underdiagnosis in affected individuals at a lower age, in addition with inadequate treatment once the condition is diagnosed, inevitably results in an excess of preventable strokes and stroke-related deaths in Austria.19
The prevalence of hypercholesterolaemia was comparable to European data obtained by the WHO.20 Although recent European guidelines recommend using low-density lipoprotein cholesterol as target for treatment, total cholesterol is recommended for the estimation of CV risk (class I, level of evidence C).10 Accordingly, in the setting of pharmacies, the possibility to conveniently obtain total cholesterol levels using a point of care device seems a feasible approach for CV risk screening and referral for further evaluation, if indicated.
Austria is one of the last European countries where the minimum age for purchasing tobacco is 16 years, in turn leading to one of the highest rates of 15-year-olds who smoke at least once a week (29% of women, 25% of men).21 This was awarded with a Guinness World Record title in 2008.22 As a response, the Austrian government passed a bill on a complete smoking ban at public places where food and drinks are served, however, coming only into effect with an inadequately long delay in May 2018.23
Limitations
Although our study is currently the largest and most recent survey directly assessing CVRFs through instrument-based tests, a selection bias due to refusal of consent cannot be excluded. Since screening is usually opportunistic, we did not aim to include a randomly chosen population sample. This might affect the observed crude prevalences of CVRFs.
Owing to time constraints of our survey, prior or current treatment for the investigated conditions was not recorded. Therefore, we might have missed patients with well-controlled risk factors, underestimating the true population-based prevalence of the respective diseases. The assessment of DM might have been biased by a low proportion (27%) of fasting participants and was potentially overestimated when using capillary glucose, point of care devices and a cut-off value of 117 mg/dL as suggested by recent European guidelines.10 The assessment of previously unknown CVRFs relied on self-reporting by participants, which is less accurate than extraction from medical reports. In a recent study conducted in pharmacies in Lower Austria we found high awareness for HTN (93%), thus, the potential bias might be mild in extent.18
Conclusion
This pharmacy-based approach for CV risk screening was able to include 6800 individuals within a 4 months survey period. We found similar overall prevalences of CVRFs as reported by nationwide registries, whereas underdiagnosis was substantial, particularly in the lower age groups. One of the three participants was confronted with a CVRF they were previously unaware of and subsequently, 45% of the cohort received a recommendation to actively consult a physician. An active screening approach at pharmacies might therefore serve as an alternative to the public preventive medical examination, particularly in younger age groups favouring the convenience and accessibility of such a pharmacy-based programme.
Acknowledgments
The authors would like to acknowledge Jan Pazourek from the Health Insurance Fund of Lower Austria, and all participating pharmacists of Lower Austria, who willingly agreed to support their research. This work was also supported by the Association for the Promotion of Research in Atherosclerosis, Thrombosis and Vascular Biology and by the Ludwig Boltzmann Foundation for Cardiovascular Research.
References
Footnotes
Contributors MR was responsible for data acquisition, statistical analysis and the primary manuscript draft. HH, HS and HK are grant holders, drafted the study protocol and recruited study centres. MT assisted with database handling, and the manuscript draft. MF, KH and TWW provided expertise for statistical analysis, interpretation of data and revised the final manuscript draft. All the authors contributed to and approved the final version of the manuscript.
Funding The study was funded by the Pharmacists College of Lower Austria (Apothekerkammer Niederösterreich) and the Health Insurance Fund of Lower Austria (Niederösterreichische Gebietskrankenkasse, NÖGKK).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics Committee of Lower Austria, Austria.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.