Article Text

Abstract
Objective To assess the relationship between serum tryptase and the occurrence of major cardiovascular and cerebrovascular events (MACCE) at 2-year follow-up in patients admitted with acute coronary syndrome (ACS). To compare serum tryptase to other validated prognostic markers (maximum high-sensitivity troponin (hs-Tn), C reactive protein (CRP) levels at admission, Synergy between percutaneous coronary intervention with Taxus and Cardiac Surgery (SYNTAX) score).
Methods We measured serum tryptase at admission in 140 consecutive patients with ACS and in 50 healthy controls. The patients’ follow-up was maintained for 2 years after discharge. The predictive accuracy of serum tryptase for 2-year MACCE was assessed and compared with hs-Tn, CRP and SYNTAX score.
Results Serum tryptase levels at admission were significantly higher in patients with ACS compared with the control group (p=0.0351). 2 years after discharge, 28/140 patients (20%) experienced MACCE. Serum tryptase levels, maximum hs-Tn measurements and SYNTAX score were higher in patients who experienced MACCE compared with those without (p<0.0001). Conversely, we found no significant association between MACCE and CRP. The predictive accuracy of serum tryptase for MACCE was set at the cut-off point of 6.7 ng/mL (sensitivity 46%, specificity 84%).
Conclusions In patients with ACS, serum tryptase measured during index admission is significantly correlated to the development of MACCE up to 2 years, demonstrating a possible long-term prognostic role of this biomarker.
- CORONARY ARTERY DISEASE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Inflammation exerts a pivotal role in the coronary artery plaque instabilisation. Among different mediators, mast cells and their neutral proteases have gained interest because of their proatherogenic role. Our group's preliminary experiences have suggested a prognostic role of serum tryptase measured at admission in patients with acute coronary syndrome (ACS).
What does this study add?
This study confirms the role of serum tryptase for stratification and prognostication in patients with ACS in a larger population sample. A cut-off point of 6.7 ng/mL measured at admission could have the best predictive accuracy for 2-year follow-up cardiovascular events.
How might this impact on clinical practice?
Serum tryptase measured at admission in patients with suspected ACS, negative troponin and not diagnostic ECG could help to early rule out.
Introduction
Although atherosclerosis is currently considered a multifactorial disease, data linking the pathogenesis of acute coronary syndromes (ACS) to systemic markers of inflammation have burgeoned in the past decades.1–4 Inflammation is an important triggering event leading to atherothrombotic clinical manifestations and may exert a pivotal role on long-term risk stratification.3 Many types of inflammation markers are able to guide leucocytes and platelet adhesion and have been shown to be predictive of death and myocardial infarction (MI) in patients with coronary artery disease.5 Several studies have documented the high sensitivity and specificity of acute phase response indicators, such as C reactive protein (CRP), interleukin-1 receptor antagonist (IL-1Ra) and IL-6, evaluated on admission, in predicting the recurrence of adverse events during both hospitalisation and follow-up.6 ,7 Furthermore, histological analyses of atherosclerotic plaques have revealed an acute inflammatory cell infiltrate at the site of plaque rupture1 ,8 and documented its involvement in localised destabilisation processes of fibrous cap tissues,1 therefore enhancing the risk of coronary thrombosis. These findings raise the chance of both improving patients’ risk stratification and assessing the response to new and more specific treatments. Accordingly, a renewed interest for the shoulder regions of atheromas and its dynamic changes during atherothrombotic events has been provided. This is an intimal area characterised by high circumferential stress.9 ,10 Pathological studies of coronary arteries of patients suffering MI have demonstrated that atheromas typically rupture in this region. Previous studies have revealed that this area is heavily populated with activated macrophages which may synthesise and secrete several proteases capable of degrading various components of the extracellular matrix. Moreover, this region is also populated by mast cells. Mast cells originate from precursors that arise in the bone marrow. They are released in the bloodstream and migrate to specific tissue sites, where they differentiate locally into mast cells under the influence of cytokines.11 Depending on the stimuli within the surrounding milieu, mast cells release numerous products with the ability to modulate a wide range of biological activities ranging from inflammation to vascular permeability. These cells have a 10-fold higher amount of neutral proteases compared with polymorphonuclear leucocytes and, through them, they may activate the metalloproteinases synthesised by the macrophages present in human atherosclerotic plaques and participate in the development of macrophage foam cells.12 ,13 Furthermore, mast cells release cytokines that may induce angiogenesis and vascular apoptosis.14 All evidences point towards the proatherogenic role of mast cells and their neutral proteases, chymase and tryptase, affecting atherosclerosis lesion formation, progression and destabilisation.15 ,16
Previous experiments have shown that mast cells concentration in the shoulder region of atheromas is 50-fold higher than in normal intima. These mast cells mostly contain tryptase, whereas the presence of the other neutral protease, chymase, is highly variable.15
It follows that mast cell-mediated mechanisms may have a leading role in ACS and their protease tryptase might be considered a target for diagnostic, prognostic and therapeutic purposes in this setting. However, previous studies exploring the role of serum tryptase in the clinical setting of ACS have reported conflicting results.17–21 Furthermore, none of them have specifically addressed the comparison between the levels of tryptase and those of the other markers considered as the reference standards for diagnostic and prognostic classification of ACS. Finally, none of them have linked tryptase levels to the extension and severity of coronary artery disease, evaluated according to accurate and validated tools. In a previous pilot study performed by our group, serum tryptase has shown a good performance both as a diagnostic and prognostic tool and has been correlated with the extension and severity of coronary artery disease as defined by the SYNTAX (Synergy between percutaneous coronary intervention with Taxus and Cardiac Surgery) score.22 ,23
The aim of our paper was to prospectively study a consecutive and wider sample of patients with ACS, to measure serum tryptase levels during hospitalisation, to evaluate its performance as a diagnostic and prognostic tool in comparison to maximum troponin measurements and to correlate it with the extension and severity of coronary artery disease as defined by the SYNTAX score.
Methods
Patients selection
We prospectively enrolled 140 consecutive patients with ACS admitted to the cardiovascular department of the ‘ASST Grande Ospedale Metropolitano Niguarda’ (Milan, Italy) from January 2013 to December 2014. Furthermore, we included in the study 50 participants without heart diseases and allergic disorders at the time of recruitment, enrolled as volunteers in our hospital, who were considered as the healthy control group. Exclusion criteria included a history of concomitant autoimmunity diseases, severe allergies, cancer, renal failure, mastocytosis, refractory anaemias, myelodysplastic syndromes, hypereosinophilic syndrome and patients receiving recombinant human stem cell. For the purpose of this study, patients were divided according to the ACS type (ST-elevation ACS (STEACS) and non-ST-elevation ACS (NSTEACS)).
Traditional cardiovascular risk factors, such as diabetes mellitus, hypertension and dyslipidaemia, were defined when patients were known to have the given risk factors prior to the index admission and were already on treatment. MI was defined in accordance with the universal definition proposed in 2012.24 Chronic obstructive pulmonary disease (COPD) was defined based on the presence of chronic airflow limitation, as assessed by postbronchodilator spirometry.
The Institutional Review Board approved the protocol, and all patients signed a written informed consent form. The study was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans.
Procedures
All study patients underwent invasive coronary arteriography and SYNTAX score was computed using the SYNTAX score algorithm, which is described in detail elsewhere25 ,26 and is available on the SYNTAX score website.27 For patients with STEACS, SYNTAX score was calculated using the angiographic views of the infarct-related artery before any intervention.28 Blood for the evaluation of serum tryptase levels was sampled at admission (acute phase). The serum was stored at −80°C before final evaluation. Blood samples were also taken in the same time window from participants in the control group. Total tryptase levels were determined by using an ImmunoCAPtryptase in vitro fluoro-enzyme-immunoassay test (Phadia, now Thermo Fisher Scientific, Uppsala, Sweden), according to the manufacturer's instructions. This laboratory method measures the total tryptase levels of all proforms of α-tryptase and β-tryptase as well as mature β-tryptase. A normal tryptase level is considered <5 ng/mL. Furthermore, maximum high-sensitivity troponin (hs-Tn) and CRP measurements obtained at admission were also taken into account for statistical analysis. Hs-Tn quantitative measurements were performed using an immunoassay test in electrochemiluminescence (ROCHE Diagnostics GmbH, Mannheim, Germany) according to the manufacturer's instructions. The 99th centile of a healthy reference population is 14 ng/L. CRP measurement was performed at admission using the particle-enhanced turbid-metric immunoassay test (ROCHE Diagnostics GmbH, Mannheim, Germany) according to the manufacturer's instructions. The reference cut-off used to rule out pathological findings is considered below 0.5 mg/dL.
Outcome definition
Follow-up of patients lasted 2 years. Outcomes include major adverse cardiovascular and cerebrovascular events (MACCE) defined as the composite of overall mortality, recurrent MI and stroke.
Statistical analysis
All data were analysed with the usual descriptive techniques: categorical data were given as frequency tables, whereas continuous data were given as mean±SD or as median and range, according to their distribution, checked by visual inspection and, when needed, also by the Shapiro-Wilk test.
Statistical significance for categorical variables was determined with Fisher’s exact test, while that of continuous variables was calculated with either the Mann-Whitney U test or Student's t-test (comparison among ACS type), one-way analysis of variance between groups or Kruskal-Wallis test (comparison among patients with MACCE, without MACCE and healthy controls), followed by post hoc tests according to Sheffé or Conover. Logistic regression was used to search for statistical significance of continuous and categorical independent variables with respect to a dependent dichotomous one: the whole model was checked with the likelihood ratio test, while any single regressor was checked with Wald’s test.
Receiver operating characteristic (ROC) analysis was performed to search for any possible optimal cut-point by means of the usual Youden's J statistics. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated for each of these cut-off values.
All statistical analyses were conducted with Stata/SE V.14.1 (StataCorp LP, College Station, Texas, USA).
Results
Patients
One hundred and fourteen patients among the total population were admitted with a diagnosis of ACS: 62 STEACS and 78 NSTEACS. Baseline characteristics of the enrolled population, as well as pharmacological treatment during hospitalisation, stratified according to the ACS type, are detailed in table 1, whereas angiographic and procedural characteristics are described in table 2.
Baseline characteristics stratified according to admission diagnosis
Angiographic and procedural characteristics stratified according to admission diagnosis
Two years after discharge, 28 patients (20%) had experienced MACCE, 25 patients had recurrent MI (17.8%), 2 patients died (1.4%) and 1 patient (0.7%) died after experiencing a recurrent MI. None of the patients included experienced stroke during the follow-up period.
Relationships between different clinical and biochemical parameters
Tryptase/MACCE
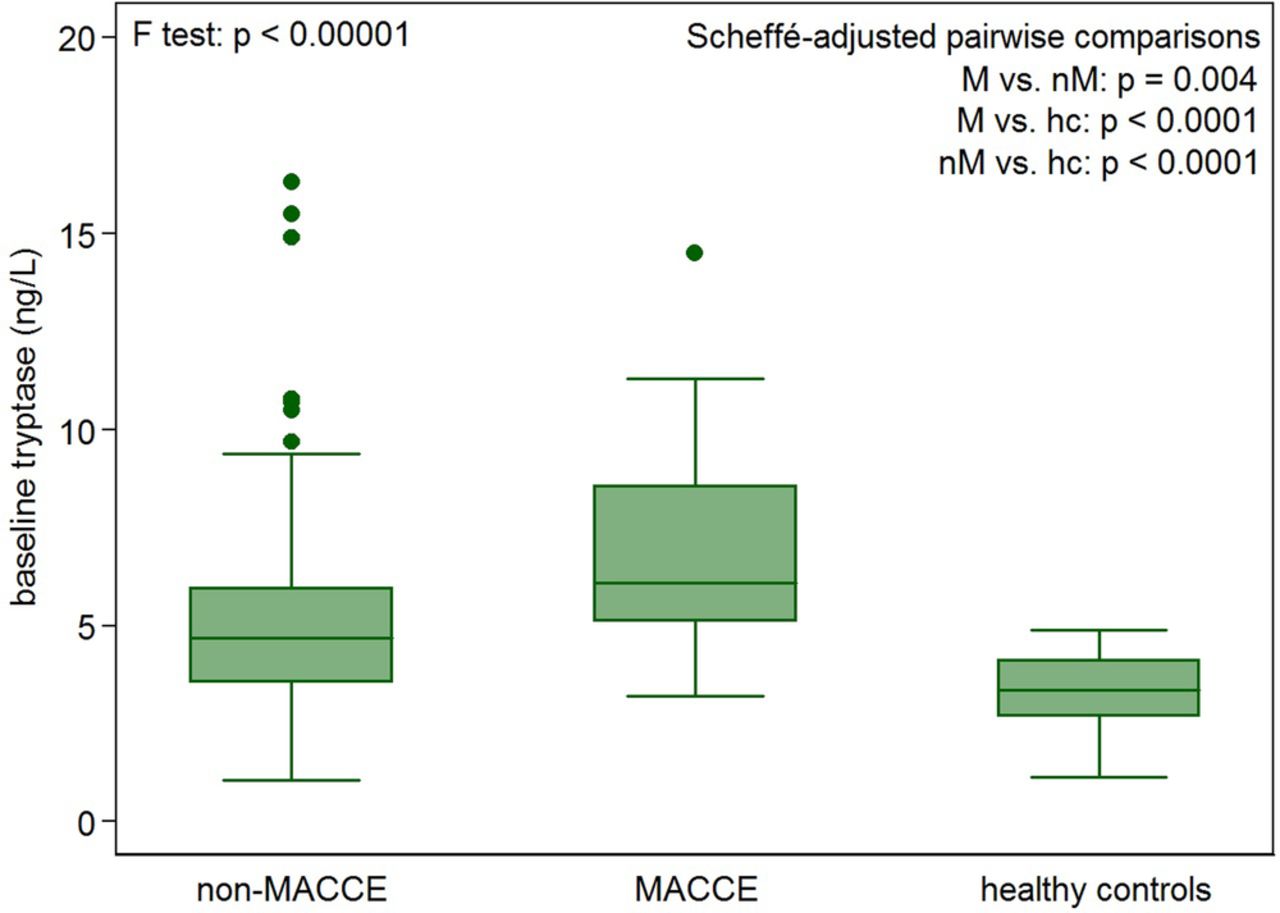
Tryptase levels at admission were significantly different in the three groups (patients with MACCE, patients without MACCE and healthy controls; p<0.0001). Pairwise comparisons showed higher tryptase levels in patients experiencing MACCE during the follow-up, compared both to patients without MACCE (6.86±2.68 vs 5.19±2.65; p=0.004) and healthy controls (3.38±0.94; p<0.001); patients without MACCE had significantly higher tryptase levels at admission compared with healthy controls (p<0.001; figure 1).
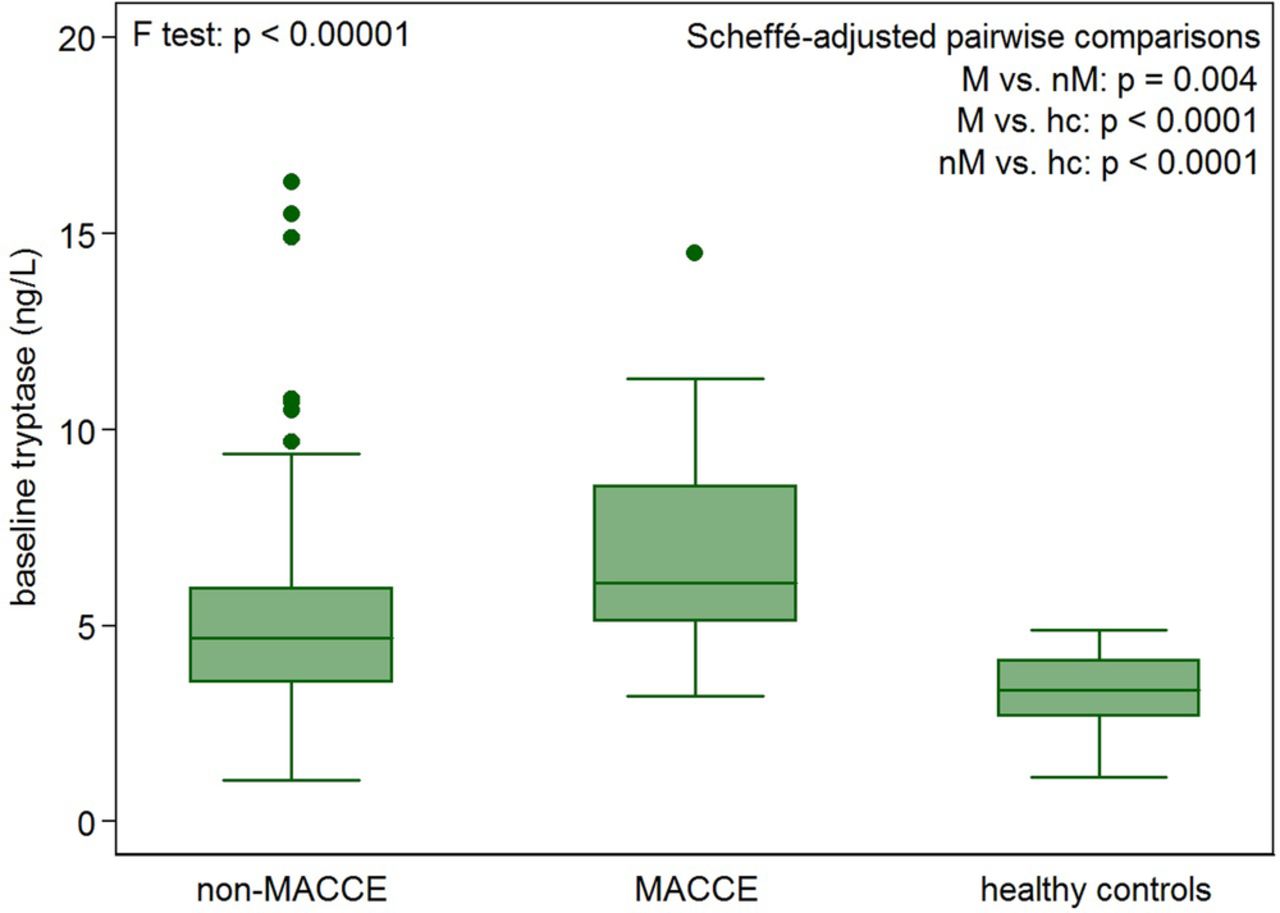
Box plots show Sheffé-adjusted pairwise comparisons between patients with MACCE, patients without MACCE and healthy controls. MACCE, major adverse cardiovascular and cerebrovascular events.
Univariate regression analysis showed that a unit increase in tryptase levels was associated with a 22% increase in the odds of experiencing an event (Wald's test p=0.007).
We searched for a possible cut-off value for tryptase levels as a predictor of MACCE. The optimal cut-off was set at 6.7 ng/mL, with 42% PPV (95% CI 25% to 61%), 86% NPV (95% CI 78% to 92%), 46% sensitivity (95% CI 28% to 66%) and 84% specificity (95% CI 75% to 90%; figure 2A). Tryptase ≥6.7 ng/mL was associated with a 343% increase in the odds of MACCE development with an OR of 4.43 (p=0.0007).

{kind=link}
{kind=link}
ROC analysis for tryptase, hs-troponin, SYNTAX score and CRP. CRP, C reactive protein; hs, high-sensitive; ROC, receiver operating characteristic; SYNTAX, Synergy between percutaneous coronary intervention with Taxus and Cardiac Surgery.
Tryptase/other variables
We evaluated the possible association between tryptase levels and other risk factors for coronary artery disease as well as known prognostic markers among patients with ACS. Tryptase levels showed positive associations with dyslipidaemia (p=0.002), COPD (p=0.025), diabetes (p=0.021) and previous MI (p=0.0001) but not with age (p=0.178), systolic hypertension (p=0.200) and current smoking habits (p=0.1434). No significant correlations between tryptase and hs-Tn p values (p>0.999), as well as between tryptase and SX-score (p>0.999) or CRP values (p=0.317), were found.
Maximum hs-Tn/MACCE
The optimal cut-off for maximum hs-Tn value as a prognostic tool for MACCE was 8890 ng/L, with 86% PPV (95% CI 42% to 100%), 84% NPV (95% CI 76% to 89%), 21% sensitivity (95% CI 8% to 41%) and 99% specificity (95% CI 95% to 100%; Figure 2B). Patients with maximum hs-Tn level ≥8890 ng/L showed a 2927% increase in the odds of MACCE with an OR of 30.272 (p<0.00001).
SYNTAX score/MACCE
Univariate analysis showed that any increase in SYNTAX score was associated with a 10% increase in the risk of MACCE. The optimal cut-off value for SYNTAX score in order to predict MACCE was 22 with 52% PPV (95% CI 32% to 72%), 89% NPV (95% CI 80% to 94%), 56% sensitivity (95% CI 35% to 76%) and 87% specificity (95% CI 78% to 93%; figure 2C). SYNTAX score ≥22 was associated with a 730% increase in the odds of MACCE with an OR of 8.32 (p<0.00001).
CRP/MACCE
The curve and the corresponding area under curve showed that CRP does not have a predictive ability in discriminating patients with MACCE from patients without events (figure 2D).
Multivariable analysis
According to multivariable analysis, tryptase levels at admission remain an independent predictor of MACCE: OR 1.242413 (95% CI 1.021336 to 1.51344; p=0.03). Other independent predictors were hs-Tn ((100 units increase): OR 1.0207 (95% CI 1.0061 to 1.0353, p=0.005)) and SYNTAX score (OR 1.087078 (95% CI 1.034984 to 1.141793, p=0.001)). The explained variability of the model was 32%.
Discussion
The major findings of the present study are the following: (1) tryptase values measured at admission may be a useful early diagnostic and prognostic tool in patients with suspected ACS; (2) in patients with confirmed ACS, tryptase measurement might further improve risk stratification when added to a conventional and well-known validated biomarker such as hs-Tn and angiographic score system such as SYNTAX-score; (3) a tryptase value >6.7 ng/mL is the optimal cut-off associated with the worst long-term outcome; therefore, it might be a safe, cost-effective and efficient method of instant risk stratification at admission in this setting; (4) generic markers of inflammation, such as CRP, are not associated with the follow-up outcome.
The early diagnostic ability of hs-Tn as well as its prognostic value concerning mortality and myocardial reinfarctions in patients with unstable coronary artery disease is well validated.29 ,30 However, clinicians are often unsure about the prognostic clinical relevance of slight increases of hs-Tn, especially in patients with other ongoing disease processes, and are inclined to ascribe them to patients’ comorbidities. Therefore, an early and accurate diagnosis and risk stratification of patients with acute chest pain admitted to the emergency room remains a clinical challenge. Inflammation has a leading role in the atherosclerotic process and may be an early marker of plaque instability. Among patients with atherosclerotic diseases, mast cells have been shown to be involved in vascular inflammation/remodelling. Throughout the release of their products, these cells may affect all the steps of the atherosclerotic process.31 On activation by different mechanisms, mostly driven by the main receptor for oxidised low-density lipoprotein (ox-LDL) on the cell surface, the Toll-like receptor 4, mast cells release histamine that increases endothelial permeability to LDL and high-density lipoprotein (HDL).32 They also release different mediators that determine proteolysis of HDL. This causes their inactivation and, as a consequence, the loss of their useful promotional activity on cholesterol efflux from macrophage foam cells.33 Moreover, since ox-LDL activates both mast cells and macrophages, these cells synergistically further increase endothelial permeability through the release of TNF-α, and aggravate the inflammatory process due to the adhesion and passage of more inflammatory cells.34 The increasing concentration of activated mast cells leads to a further massive release of tryptase and chymase that can degrade collagen of extracellular matrices and many proteins of the fibrous cap of the atherosclerotic plaques, promoting plaque destabilisation and its consequential rupture. The wide vessel remodelling associated with mast cells and their mediators may explain the worst prognosis of patients presenting with ACS and higher tryptase levels. The observation that a high tryptase level identified the patients presenting with MACCE after 2 years from ACS is an in vivo demonstration of tryptase major role as a marker of the inflammatory and atherosclerotic process. An optimal cut-off level of 6.7 ng/mL for tryptase measurements may identify patients with a higher risk of vascular events and differentiate them from other aspecific inflammatory processes. Moreover, the significant association between a positive history of dyslipidaemic alterations and higher tryptase levels could further support the relationship between mast cell activation and atherosclerosis.
Finally, it is important to point out how the role of serum tryptase remains relevant even after adjustment for well-known markers of cardiovascular events in the ACS setting. It is well known that a gradient of risk for future cardiovascular events starts at hs-Tn concentrations close to the limit of detection.35 Interestingly, tryptase values measured at admission remained an independent predictor of events even adjusting for this validated and extremely sensible biomarker, taken at its maximum concentration during index admission.
This holds true even considering the severity and extension of coronary artery disease, as evaluated by the SX-score. SX-score allows an assessment of overall coronary lesion complexity, with lower scores representing less complex coronary disease (a low score is defined as <22).36 Not surprisingly, 22 was even the optimal cut-off associated with the worst long-term outcome in the present analysis.
Conclusions
In conclusion, serum tryptase might be a further tool to early identify patients with high risk of ACS and long-term recurrent events. Its evaluation does not substitute well validated markers and scores, but might have an incremental value in more complex settings.
References
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.