Article Text

Abstract
Objective The aim of this study is to assess the association between genetic ancestry, self-declared race and haemodynamic parameters in patients with chronic heart failure (HF).
Methods Observational, cross-sectional study. Eligible participants were aged between 18 and 80 years; ejection fraction was ≤50%. Patients underwent genetic analysis of ancestry informative markers, echocardiography and impedance cardiography (ICG). Race was determined by self-classification into two groups: white and non-white. Genomic ancestry was estimated using a panel of 101 348 polymorphic markers and three continental reference populations (European, African and Native American).
Results Our study included 362 patients with HF between August 2012 and August 2014. 123 patients with HF declared themselves as white and 234 patients declared themselves as non-white. No statistically significant differences were found regarding the ICG parameters according to self-declared race. The Amerindian ancestry was positively correlated with systolic time ratio (r=0.109, p<0.05). The thoracic fluid content index (r=0.124. p<0.05), E wave peak (r=0.127. p<0.05) and E/e′ ratio (r=0.197. p<0.01) were correlated positively with African ancestry. In multiple linear regression, African ancestry remained associated with the E/e′ ratio, even after adjustment to risk factors.
Conclusions The African genetic ancestry was associated with worse parameters of diastolic function; the Amerindian ancestry correlated with a worse pattern of ventricular contractility, while self-declared colour was not helpful to infer haemodynamic profiles in HF.
Trials registration number NTC02043431.
- HEART FAILURE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Incidence and prognosis in heart failure (HF) differ across ethnic groups. Mortality and hospitalisation rates for HF are higher among African-Americans than among their white counterparts.
What does this study add?
The African genetic ancestry was associated with worse parameters of diastolic function in patients with HF while the Amerindian ancestry was associated with higher values of systolic time ratio and raises the hypothesis of a possible explanation for the differences in prognosis between the ethnic groups.
How might this impact on clinical practice?
Genetic analysis, once their cost is reduced to a cost-effective level, should be incorporated into clinical practice to define high-risk groups and guide treatment in HF.
Introduction
Heart failure (HF) is a major cause of morbidity and mortality in the world, with a major impact on health systems.1 Despite the available therapies, this syndrome is now the leading cause of hospitalisation in persons aged over 65 years and is a major contributor to increased costs of healthcare.1 ,2
Previous studies have also shown that the incidence and prognosis of HF differ across ethnic groups. Mortality and hospitalisation rates for HF are higher among African-Americans than among their white counterparts.3 ,4
Disparity in the prevalence and outcomes of HF among blacks and whites has been attributed to a wide range of factors. Among them are racial/ethnic differences in the prevalence of underlying diseases, quality and availability of healthcare and disparities in socioeconomic factors.5 ,6 However, isolated ethnic differences in socioeconomic indicators cannot fully explain the high mortality among black patients.7 ,8 This finding has reinforced the idea that part of the ethnic differences in cardiovascular events is mediated by genetic factors that might determine disease severity and response to therapy in HF.9
Pathophysiological mechanisms that are aetiologically linked to the development of heart diseases tend to be disproportionately prevalent in selected racial/ethnic groups. African descents has been related to salt sensitivity, excessive renin-angiotensin system-dependent target-organ injury, endothelium-dependent and endothelium-independent vascular abnormal responses. These evidences suggest that this racial group can present a worse haemodynamics in HF leading to worse outcomes.10
Furthermore, studies have shown that, compared to European descendants, African-American patients have important differences in the frequencies of functionally significant alleles encoding important components of neurohormonal signalling cells in HF.11–15 Results are still controversial, and a clear association between different HF endophenotypes, including haemodynamic pattern and genetic ancestry, has not been previously explored. Therefore, the objective of this study is to assess the association of genetic ancestry with non-invasive haemodynamic parameters in patients with chronic HF and reduced ejection fraction from a multiethnic population.
Material and methods
GENIUS-HF is an observational, prospective cohort, single-centre study and it is still ongoing. The individuals invited to our study were consecutively selected from the Heart Institute—Clinical Hospital- University of São Paulo Medical School (InCor—HCFMUSP). Its methodology has been previously published.16 This analysis is a cross-sectional evaluation of the association between haemodynamic profile and genomic ancestry conducted between August 2012 and August 2014.
Eligibility criteria
The eligibility criteria are the same as in the GENIUS-HF study. We included patients between 18 and 80 years of age, with a history and physical examination compatible with HF, left ventricular ejection fraction (LVEF) ≤50% documented in transthoracic Doppler echocardiography in the past year. Exclusion criteria were advanced dementia or any other mental or psychiatric disorders that would limit the collection of information; patients who refused the provision of informed consent form and, for this analysis, patients who have not been evaluated by impedance cardiography (ICG) for any reason.
Ethical aspects
The Ethics Committee for Medical Research in Human of the Clinical Hospital of the School of Medicine, University of São Paulo approved the study protocol (Protocol number 0398/04—SDC 2368/03/162) and all individuals signed an informed consent form. This study was registered at Clinical Trials.gov under number NTC02043431.
Study procedures
Once eligible, patients underwent clinical evaluation and laboratory testing, including transthoracic Doppler echocardiography, ICG and blood collection. Patients were interviewed at a medical appointment for knowledge about medical history, symptoms, medication use, HF aetiology and socioeconomic measures.
Race was self-identified according to the Brazilian Institute of Geography and Statistics (IBGE) for race classification: white, black, ‘pardo’ (an intermediate colour category—brown), yellow or indigenous.17 For the purposes of this analysis, we categorised them into two groups: white (self-declared white) and non-white (other self-declared race).17
Echocardiogram and haemodynamic evaluation
Haemodynamic data were obtained in a non-invasive manner using the CardioScreen 2000 haemodynamic measurement system (Medis-Ilmenau, Germany). The parameters, definitions and normal values for each variable can be found in online supplementary material 1. Doppler echocardiography was performed simultaneously with the ICG in an Acuson Sequoia S512 system (Siemens, Pennsylvania, USA). The following parameters were assessed: left ventricular (LV) cavity diameters and left atrial volume index; thickness of the posterior wall and interventricular septum; LVEF, the peak Doppler velocities of early (E) and late diastolic flow (A), the deceleration time and the E/A ratio. The ratio of mitral velocity to early diastolic velocity of the mitral annulus (E/E′) was also measured.
Supplementary material
Genetic molecular analysis
Genotyping data
Individuals from the GENIUS-HF study were genotyped on the Axiom assay from genomic DNA on the AxiomTM Genome-Wide InCor_BB Array, a custom chip that genotypes ∼800 000 single nucleotide polymorphisms (SNPs). To analyse genetic ancestry, we used the shared SNPs between the reference populations and GENIUS-HF samples, totalling 101 348 common SNPs.
Data cleaning
We applied two filters for SNP cleaning: (1) missing genotype rate per marker, where no markers containing genotype missing rates above 10% were identified; (2) Hardy-Weinberg equilibrium (HWE), where 10 201 markers were excluded from our sample based on the HWE test (p≤0.0001). We did not apply a filter for minor allele frequency (MAF <0.01) since markers in the genotyping platform were rare.
Three exploratory tools were applied to evaluate sample quality: (1) missing genotype rate, where no samples demonstrated more than 10% of missing genotypes; (2) Identity by descent (IBD) analysis, where we identified 13 pairs of duplicate individuals and (3) a sex analysis check, where we verified any incompatibility between informed and genotypically evaluated gender. All data cleaning procedures were performed using the PLINK package.18
Genomic ancestry
The evaluation of genomic ancestry was conducted using the Admixture program.19 Admixture is a software tool for maximum likelihood estimation of individual ancestries from multilocus SNP genotype data sets. Since the contributions of different ancestral genomes have previously been described by our group, as well as others, we used a supervised approach for ancestry determination.20 Parameters were set at 200 bootstrap replicates (default) and three populations were assumed for the analysis.
This analysis was performed using all 101 348 common autosomal SNPs between the study and reference populations.21 We assumed as reference ancestral populations all individuals from the Human Genome Diversity Project (HGDP):22 Pima, Maya as Amerindians and from the HapMap project:23 Africans—YRI (Yoruba in Ibadan, Nigeria), LWK (Luhya in Webuye, Kenya), ASW (Americans of African Ancestry in SW, USA); European—CEU (Utah Residents (CEPH) with Northern and Western European ancestry) and TSI (Tuscan in Italia).24 ,25
Data collection system
Study data were collected and managed using the electronic data capture application REDCap (Research Electronic Data Capture), hosted at the Hospital das Clinicas of the School of Medicine, University of São Paulo. REDCap is an application designed to have security compliant with common requirements.26
Statistical analysis
We used the χ2 or Fisher’s exact tests to compare categorical variables between white and non-white groups. The parameters of ICG and the variables of ancestry were normally distributed, except for the variable O/C ratio. This variable was therefore log-transformed. Genetic ancestry variables were used as continuous variables. Correlation between numerical variables was analysed using Pearson’s correlation coefficient. Student's t-test was used to determine differences between the means of ICG and echocardiographic variables by gender and self-declared race (white and non-white). Multiple linear regression analysis using as the dependent variable lateral E/e′ ratio was built in two models (table 5). The first model included the African ancestry while the second model used the non-white self-reported race. Both models also estimated the interaction between age and chronic renal failure and the variables associated with the lateral E/e′ ratio in the univariate analysis (see online supplementary material 2). Owing to the high penetration of Chagas disease in this study, which could confuse the interpretation of results, we performed a sensitivity analysis on the sample of patients without Chagas disease (see online supplementary material 3). Additionally, we used a generalised linear model with a Gaussian family distribution to estimate predicted mean of lateral E/e′ with 95% CIs for each 10% of genomic ancestry and for self-reported race (white and non-white). Estimates were adjusted for the same variables of the model. The tests, although multiple, are correlated and our sample size is not powered for conservative multiple testing correction approaches.
Supplementary material
Supplementary material
Statistical analyses were conducted using the SPSS V.16.0 software (SPSS, Illinois, USA) and statistical significance was set at the 0.05 level.
Results
We included 500 patients between August 2012 and August 2014, all meeting the eligibility criteria and consenting to participate in this study. Of these, 2 withdrew informed consent, 364 underwent ICG and 317 transthoracic echocardiography. Data from 2 participants of 364 undergoing ICG on admission visit had incomplete information and were therefore discarded from our analysis. Of the 362 remaining patients considered for this subanalysis, genetic evaluations from 14 patients were excluded for not meeting our quality criteria. Our overall study workflow is depicted in figure 1.
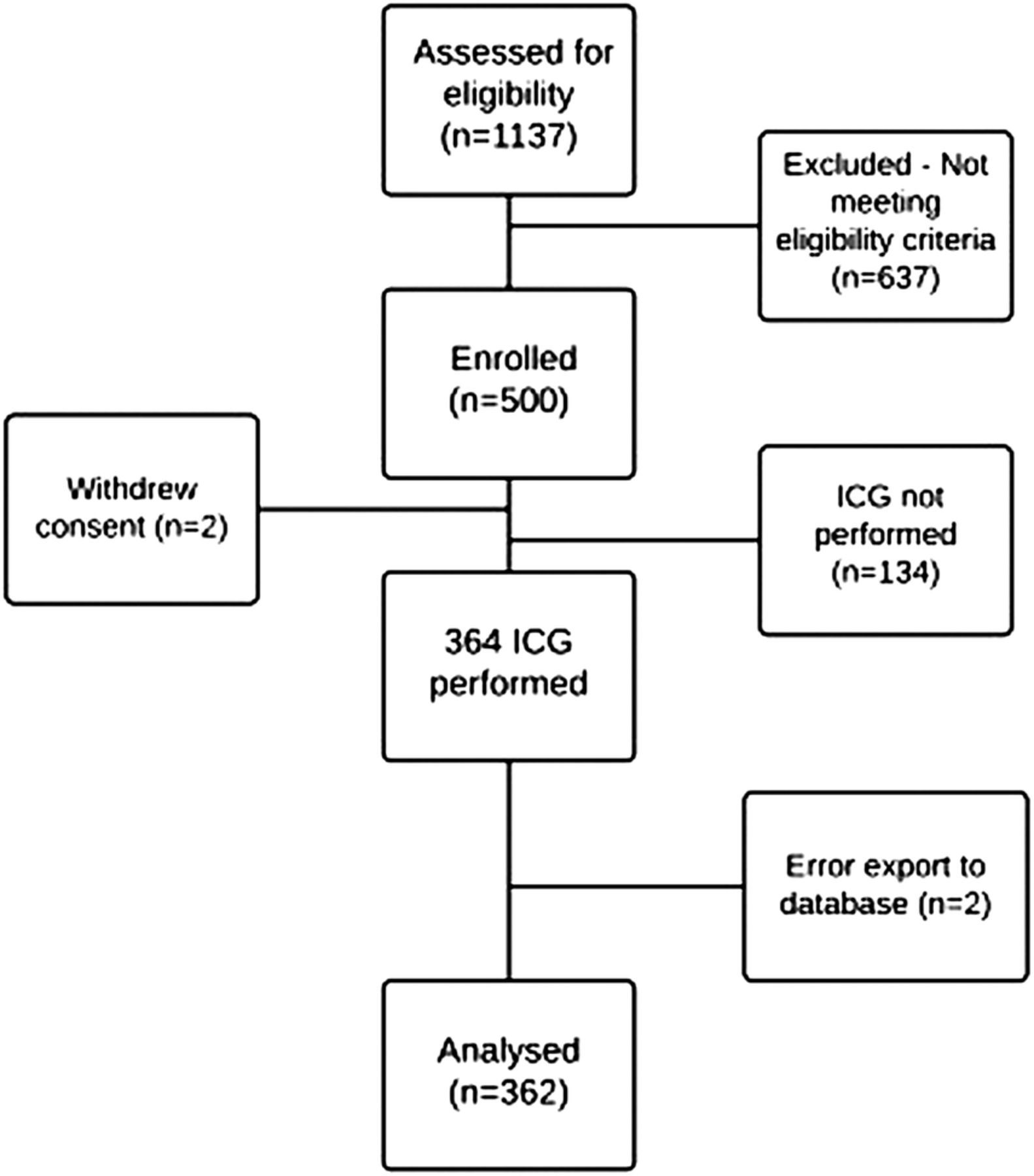
GENIUS-HF study flow chart. ICG, impedance cardiography.
Self-declared race, clinical characteristics and treatment
The clinical characteristics and treatment according to the self-declared ethnicity (white and non-white) are in table 1. Self-declared ‘yellow’ and native patients represented a small portion (5 patients) of the overall studied population.
Clinical features and treatment according to the self-declared race
Ischaemic aetiology was significantly more prevalent in the self-declared white group (30.9% vs 20.1%, p=0.032), whereas Chagas disease was more prevalent in self-declared non-white patients (23.5% vs 13.0%, p=0.026). Patients in the self-declared non-white group more commonly had an educational level only up to elementary school (78.2% vs 60.7%, p=0.001). Age, gender, comorbidities, body mass index, functional class, LVEF, socioeconomic status and use of ACE inhibitors/angiotensin-receptor blocker or β-blockers did not significantly differ by self-declared race.
Comparison between self-declared race and genomic ancestry
When evaluating our study sample, the distribution of average European, African and Amerindian ancestry was, respectively, 61%, 29% and 6%. Self-reported ethnicity was represented as follows: 123 white patients (34.5%); 179 brown patients (50.1%); 55 black patients (15.4%); 5 patients classified as other (1.4%).
Patients self-reported as white presented an average of 80% European ancestry, 12% of African ancestry and 8% of Amerindian ancestry. Among self-declared brown patients, genetic ancestry was 58% European, 31% African and 11% Amerindian. Self-declared black patients had on average 32% European ancestry, 61% African ancestry and 7% Amerindian ancestry.
In figure 2, we observed that self-identified white patients have a higher percentage of European descent when compared to self-declared non-white patients. Self-identified non-white patients showed higher African descent compared to self-identified white patients. The occurrence of Amerindian ancestry was below 40% in groups (white and non-white).

Comparison of genomic ancestry with self-declared race.
As expected, mean genetic ancestry (European, African and Amerindian) demonstrated statistically significant differences in relation to self-declared race (white, brown and black) (p<0.001; table 2).
Comparison of self-declared race with the genetic ancestry
Haemodynamic parameters and self-declared race
The adjusted association between ICG parameters and self-declared race did not demonstrate any statistically significant differences between the white and non-white groups (table 3).
ICG and echocardiographic parameters in HF according to the self-declared ethnicity
Comparing adjusted mean values from the Doppler echocardiography evaluation between white and non-white groups, the averages of the interventricular septum (9.4 mm vs 8,8 mm, p=0.004), posterior wall of the left ventricle (9.5 mm vs 9,2 mm, p=0.046), LV mass index (149 g/m2 vs 136 g/m2, p=0.023) and the medial E/e′ ratio (9 vs 7, p=0.016) were higher for the non-white group (table 3).
Haemodynamic parameters and genomic ancestry
Correlation between ICG parameters and Doppler echocardiography with the European, Amerindian and African ancestry showed a weak positive correlation to the systolic time ratio with Amerindian ancestry (r=0.109, p<0.05). The thoracic fluid content (r=0.124, p<0.05), the wave E peak (r=0.127, p<0.05) and the medial E/e′ ratio (r=0.142, p<0.05) and lateral E/e′ ratio (r=0.197, p<0.01) correlated positively with African ancestry, while European ancestry was negatively correlated with the wave E peak (r=−0.118, p<0.05) and medial E/e′ ratio (r=−0.120, p<0.05) (table 4).
Correlation of ICG and echocardiographic parameters with genetic ancestry
Table 5 shows the results of multiple linear regression analysis.
Multiple linear regression of medial E/e′ ratio as the dependent variable
In model 1, African ancestry (p=0.005), chronic renal failure (p=0.005), mean arterial pressure (p=0.001), functional class (p=0.002) and LVEF (p=0.001) were associated with measures of the lateral E/e′ ratio (R²=18.3%; AIC=1461.5). Model 2 presents the chronic renal failure (p=0.008), mean arterial pressure (p<0.001), functional class (p=0.004) and LVEF (p=0.001) associated with the lateral E/e′ ratio (R²=16.5%; AIC=1467 8). The self-declared race was not associated with this variable (p=0.165).
A positive association between the E/e′ lateral ratio and African ancestry remained positive even after performing a sensitivity analysis where (1) patients with Chagas disease were excluded (see online supplementary material 3) or (2) disease duration and use of diuretics were included in the models.
Estimations of lateral E/e′ for differences in the African ancestry of 10% and in self-declared race are found in online supplementary material 4.
Supplementary material
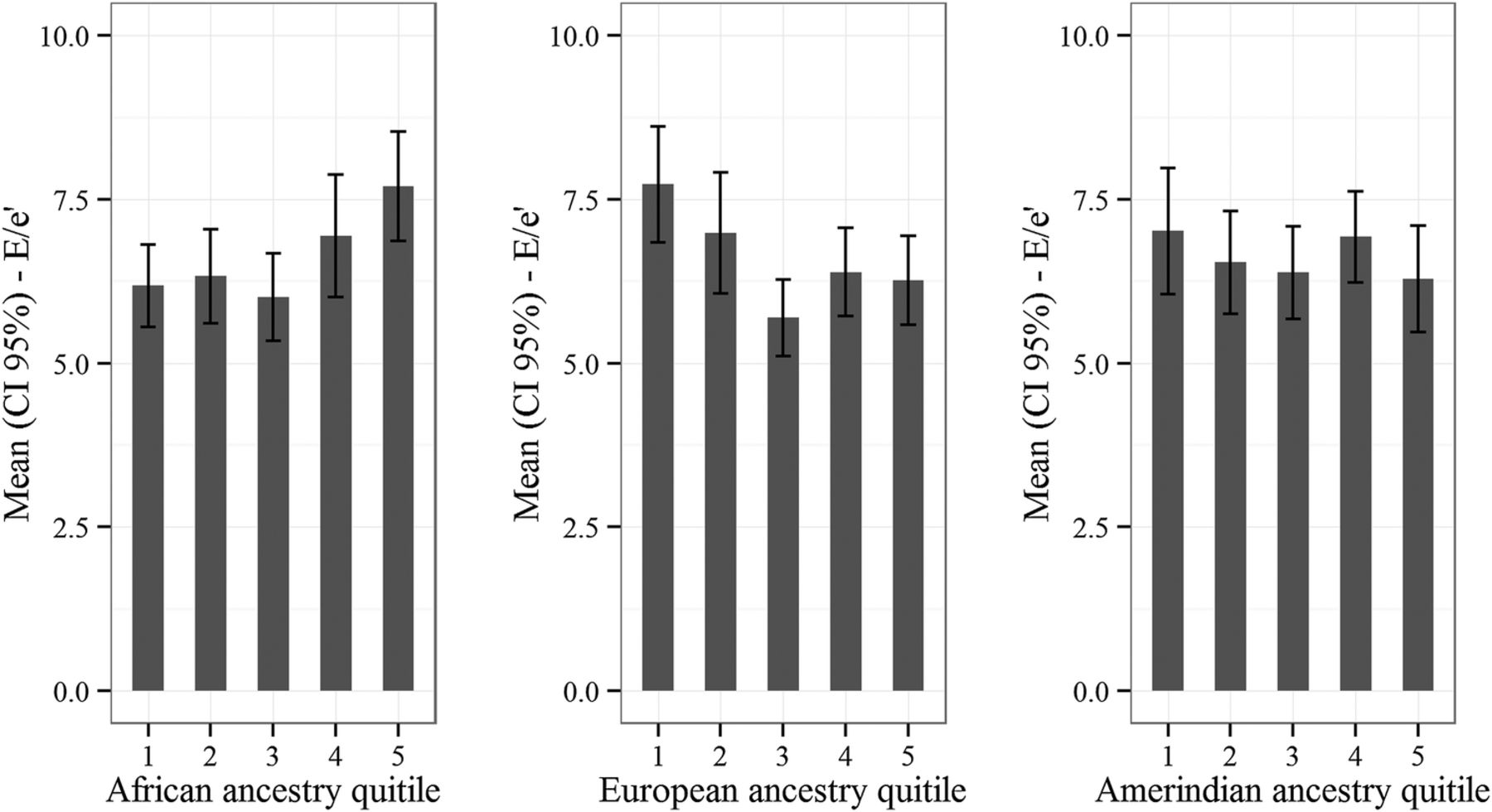
Finally, the higher the African ancestry, the higher lateral E/e′. The opposite being true among those of European ancestry, as demonstrated by the association between the mean of lateral E/e′ by quintiles of genomic ancestry (figure 3).
{kind=link}
{kind=link}
{kind=link}
Lateral E/e′ ratio and genomic ancestry.
Discussion
To the best of our knowledge, this is the first study reporting genomic ancestry and haemodynamic pattern in patients with HF. We found that although self-reported race was associated with genetic ancestry, there was a considerable range which ancestry levels would characterise a given self-reported race disagreement between them in a considerable percentage of patients. In addition, the results of this article showed the presence of a positive association between peak E wave, septal and lateral E/e0 ratio and thoracic fluid content with African ancestry while the contractility parameter, systolic time ratio, was positively correlated with ancestry Amerindian. Finally, African ancestry showed a positive relationship with the lateral E/e′ ratio, which did not occur for the self-declared non-white.
Genetic ancestry and self-declared race
The Brazilian population was constituted by an extensive miscegenation among three different ancestral origins: Amerindians, Europeans and Africans.27 Our present study demonstrated a predominance of European ancestry in the entire study population. Previous data are in agreement with our findings.19 ,24 ,27
In this study, self-declared race is associated with genetic ancestry. However, our data suggest a higher reliability of the use of genetic ancestry in clinical studies, especially in a mixed population. Feldman et al argue that confusing self-declared race and ancestry can be potentially devastating to the practice of medicine. In one of our arms, we have used a categorical variable (white, brown and black), while the other has been quantified using a continuous variable indicating genetic ancestry (European, Amerindian and African).28
Amerindian ancestry and ventricular contractility
We found a weak positive correlation between the systolic time ratio and Amerindian ancestry. This ICG parameter is derived from the relationship between the pre-ejection and LV ejection time. The higher the systolic time ratio, the worse the ventricular contractility. This ICG parameter has shown to have great potential to be a reliable monitoring method of ventricular function in chronic HF.
Thompson et al29 demonstrated that systolic time ratio was able to distinguish between HF with preserved function and systolic dysfunction HF. Changes in the cardiac index and systolic time ratio were highly correlated with changes in LVEF.30 Furthermore, systolic time ratio proved to be a reliable prognostic parameter in patients with HF. Brain natriuretic peptide (BNP) and systolic time ratio proved to be the strongest future event predictors related to HF. Patients with BNP >100 pg/mL and systolic time ratio >0.45sec−1 had a free-events survival rate significantly smaller.31
To the best of our knowledge, the only study evaluating genetic ancestry in another sample population of patients with HF in Brazil demonstrated that the Amerindian ancestry was associated with greater survival rates compared to African and European ancestries, which contradicts our findings.32 Once the Amerindian ancestry correlated positively with systolic time ratio and the higher the values of this parameter, the worse the ventricular function, we would expect a worse prognosis. Therefore, new studies in the field are required to have a better understanding of the role of genetic ancestry in the occurrence of events in patients with HF.
African ancestry and diastolic function
We found that the greater the degree of African ancestry, the higher the indices of the E/e′ ratio. These findings remained significant even after adjustment. However, when a similar model was run for the association with the self-declared non-black race, the association was no longer significant.
A worse diastolic LV performance was observed in African-Caribbean hypertensive patients (expressed by the high values of the E/e′ ratio and lower values E’ wave) included in the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) when compared to their white European counterparts. The role of African-Caribbean ethnicity in diastolic function persisted even after adjustment for potential confounders such as age and LV mass, leading researchers to hypothesise the existence of an intrinsic difference in diastolic LV performance between the two racial/ethnic groups. However, this previous analysis did not include the time at diagnosis of hypertension as well as the difference in antihypertensive treatment between the groups.33
Russo et al observed, after adjustment for age and sex, that blacks and Hispanics had worse diastolic function when compared to whites. Hispanics showed lower E/A ratio transmitral velocity, lower E’ wave and higher E/e′ ratio in relation to whites, while blacks had a significantly lower wave velocity medial E’ and a tendency to higher E/e′. After adjustment for cardiovascular risk factors and other potential confounders, the authors found no significant differences in the parameters of diastolic function between the three ethnic-racial groups. These findings suggest that most of the observed differences were secondary to significantly imbalanced risk factors, rather than factors intrinsic to ethnicity or race.34
Patients in the GENIUS-HF cohort are currently being followed every 6 months for a 3-year follow-up, which will allow us to present new information about prognosis and genetic ancestry.
Limitations
Despite its novel findings, our study has limitations. First, it is an observational study and thus is not free of selection bias and confounding. Owing to this possibility, some actions were taken as a multivariate analysis to control for confounding factors.
Another issue that could be a limitation in our study is the number of patients who were not evaluated by ICG. Most of the 134 patients did not perform the ICG analysis due to unavailability of the equipment during the enrolment phase of the study. Less than 10% of all patients undergoing ICG analysis presented factors limiting the examination. Thus, we believe that the selection bias was not of a magnitude that could affect our main results and conclusions.
Regarding statistical analysis, the tests, although multiple, are correlated and our sample size is not powered for conservative multiple testing correction approaches.
Finally, external validity can also be compromised in this study since the genetic ancestry data may vary between regions.
Conclusion
The African genetic ancestry was associated with worse parameters of diastolic function in patients with HF, while the Amerindian ancestry was associated with higher values of systolic time ratio and raises the hypothesis of a possible explanation for the differences in prognosis between the ethnic groups. Additionally, the results of this study emphasise the need to be cautious when using self-declared race as a representative of ancestry or by extrapolating the results of a mixed population to another.
Acknowledgments
The authors thank Rafael Muniz Miranda da Silva for his assistance in data management and Lucas Petri Damiani for his statistical modelling assistance.
References
Footnotes
Contributors SB-P conceived of the GENIUS-HF substudy, designed the data collection tools, contributed to protocol development, monitored the data collection, acquired and analysed the data, and designed the draft. LG-P designed the data collection tools, monitored the data collection, contribute to protocol development and revised the draft paper; FGM-B designed the data collection tools, contribute to protocol development, acquired the data and revised the draft paper. PCJLS provided statistical expertise, analysed the data and revised the draft paper. JMRS planned and managed the data collection and acquired the data. ARVRH provided expertise in genomic analysis and revised the draft paper. HCS provided expertise in genomic analysis and revised the draft paper. FB contributed to protocol development and revised the draft paper. FF contributed to protocol development and revised the draft paper. AJM contribute to protocol development and revised the draft paper. RP provided statistical expertise, analysed the data and revised the draft paper. JEK analysed the data and revised the draft paper. ETM conceived of the substudy; analysed the data and revised the draft paper. AdCP conceived of the GENIUS-HF study, analysed the data and drafted and revised the paper. All authors contributed to refinement of the study protocol and approved the final manuscript.
Funding Fundação Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), n11/2009, Brazil. Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP)—n 17368-0/2013, Brazil. PROADI-SUS Program, Brazil Health Ministry, Brazil. This study had no relationship with the industry.
Competing interests None declared.
Ethics approval The Ethics Committee for Medical Research in Human of the Clinical Hospital of the School of Medicine, University of São Paulo approved the study protocol (Protocol number 0398/04—SDC 2368/03/162).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.