Article Text

Abstract
Objective In acute coronary syndromes, switching between thienopyridines is frequent. The aims of the study were to assess the association between switching practices and quality of care.
Methods Registry study performed in 213 French public university, public non-academic and private hospitals. All consecutive patients admitted for acute myocardial infarction (MI; <48 hours) between 1/10/2010 and 30/11/2010 were eligible. Clinical and biological data were recorded up to 12 months follow-up.
Results Among 4101 patients receiving thienopyridines, a switch was performed in 868 (21.2%): 678 (16.5%) from clopidogrel to prasugrel and 190 (4.6%) from prasugrel to clopidogrel. Predictors of switch were ST segment elevation MI presentation, admission to a cardiology unit, previous percutaneous coronary intervention, younger age, body weight >60 kg, no history of stroke, cardiac arrest, anaemia or renal dysfunction. In patients with a switch, eligibility for prasugrel was >82% and appropriate use of a switch was 86% from clopidogrel to prasugrel and 20% from prasugrel to clopidogrel. Quality indicators scored higher in the group with a switch and also in centres where the switch rate was higher.
Conclusions As applied in the French Registry on Acute ST-elevation and non ST-elevation Myocardial Infarction (FAST-MI) registry, switching from one P2Y12 inhibitor to another led to a more appropriate prescription and was associated with higher scores on indicators of quality of care.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
The choice between clopidogrel and prasugrel is based on patient characteristics and management. In some clinical situations, the initial choice may be suboptimal and a switch between molecules may be performed. The relation between the rate of switching and indicators of quality of care has never been investigated.
What does this study add?
This study informs on the rates of switching practices, showing that it is quite frequent (around 21.2% of patients). We further report that in a large nationwide registry of over 4000 patients, this practice was not associated with misuse of thienopyridines, but with higher scores on indicators of quality of care.
How might this impact on clinical practice?
The findings of this study indicate that patients may safely be switched from clopidogrel to prasugrel or vice versa, to allow optimum therapy in accordance with the indications for each patient.
Introduction
Changing a patient's treatment and management in the light of new information or clinical changes is often mandatory in routine practice. In the setting of acute coronary syndromes (ACS), dual antiplatelet therapy (DAPT) is recommended as early as possible, and the initial thienopyridine is chosen according to drug labelling and available clinical information. During the in-hospital phase, more information becomes available to the physician,1 and the initial choice of treatment may come to be considered as suboptimal. Customisation of oral antiplatelet treatment can prompt a switch from one drug to another. In a large registry study, among 40 531 patients initially treated with clopidogrel, 5.2% were switched to prasugrel and 11.5% of those with an initial prescription of prasugrel were discharged under clopidogrel.2–4 Nevertheless, the appropriateness of these switches and their association with quality of care is poorly documented. We use data from French Registry on Acute ST-elevation and non ST-elevation Myocardial Infarction (FAST-MI) 2010, a nationwide multicentre registry of patients admitted for acute myocardial infarction (AMI) in France,5 (1) to determine the rate and predictors of switching between clopidogrel and prasugrel and vice versa; (2) to assess the appropriateness of the choice of thienopyridine; and (3) to assess the association between switch rate and quality of care by centre.
Methods
Data sources and population
The population and methods of the FAST-MI 2010 registry have been described previously.5 Briefly, all consecutive patients admitted for AMI (<48 hours) between 1 October and 30 November 2010 in 213 French hospitals were eligible for inclusion. Data collected included the Cardiology Audit and Registration Data System data set6 as well as a number of additional variables, and data from clinical follow-up were recorded up to 12 months. A centralised electronic case report form was used, and the quality of data was monitored by automatic data checks and independent external research assistants.
Written informed consent was provided by each patient for participation in the study. The study was conducted in compliance with Good Clinical Practice, French legislation and French data protection laws. The protocol was reviewed and approved by the Committee for the Protection of Human Subjects of Saint Louis University Hospital Paris Ile de France IV, Paris, France.
Definitions
Switch: Use of thienopyridines was collected at four time points (prehospital, admission—24 hours, 24–48 hours and discharge). Any change in thienopyridines during hospitalisation was recorded as a switch (regardless of the direction). Switches were also considered separately (ie, from clopidogrel to prasugrel, and from prasugrel to clopidogrel).
Eligibility for prasugrel was defined, according to the French labelling, as patients with ACS, without history of stroke or transient ischaemic attack (TIA), aged<75 years, body weight≥60 kg, and intended for percutaneous coronary intervention (PCI; to define eligibility at admission) or PCI actually performed (to define eligibility at discharge).
Appropriate use of a switch in thienopyridines was defined as (1) non-eligibility for the first thienopyridine, (2) bleeding or thrombotic event related to the admission thienopyridine or (3) expectation of potential clinical benefit, supported by the results of clinical randomised trials (ie, switch from clopidogrel to prasugrel in patients eligible for prasugrel, as shown in the TRITON study,7 or switch from prasugrel to clopidogrel in patients treated without PCI, as shown in the TRILOGY study).8
Quality of care: Quality indicators were defined for each centre as the rate of use, at discharge, of DAPT, β-blockers, ACE inhibitors and statins, irrespective of potential contraindications; and, for patients with ST segment elevation MI (STEMI), as the rate of use of reperfusion and the rate of timely reperfusion (ie, reperfusion within 120 min by primary PCI or within 60 min by thrombolysis). A composite indicator was calculated using opportunity scoring (one point by applicable indicator divided by the number of applicable indicators).
Statistics
Categorical variables are presented as number of cases (percentage), continuous non-normally distributed variables as median (IQR), and continuous normally distributed variables as mean±SD.
Description of switching practices: We report the rate, timing and modalities of switches in the whole population and by centre.
Predictors of switching (any switch, regardless of the direction) were identified by logistic regression. Variables introduced into the model were age (by quartiles), body weight (≥ or <60 kg), type of MI, symptoms at presentation (chest pain, dyspnoea, cardiac arrest or other), cardiovascular risk factors (hypertension, diabetes, hypercholesterolaemia, smoking), history (of angina, MI, percutaneous or surgical revascularisation, stroke, peripheral artery disease, heart failure, cancer, Alzheimer's disease), chronic treatment with aspirin, β-blockers, ACE inhibitors (or angiotensin receptor blockers), statins, insulin, nitrates or oral anticoagulation, haemodynamic conditions at admission (all components of the Global Registry of Acute Coronary Events (GRACE) risk score, sinus rhythm, atrioventricular block) and biological variables (glucose and haemoglobin levels). We also used centre-related variables such as university versus community hospital, high versus low volume (characterised according to the median annual number of admissions for AMI) and availability of a catheterisation laboratory on site or not. A stepwise approach was used, with a threshold of <0.05 for entry and for remaining in the model.
Quality of care indicators associated with switching: Centres were categorised into four groups according to the rate of use of switch (by quartiles): between 0% and 7%, 8–18%, 19–33% and above 33%. We compared indicators of quality of care across the four centre groups. To compare quality indicators between categories, trend analyses were performed using the Cochran Armitage test for qualitative variables or the Jonckheere-Terpstra test for quantitative variables.
All tests were two sided, and a p value <0.05 was considered significant. All analyses were performed using SAS software, V.9.2 (SAS Institute Inc, Cary, North Carolina, USA).
Results
Study population
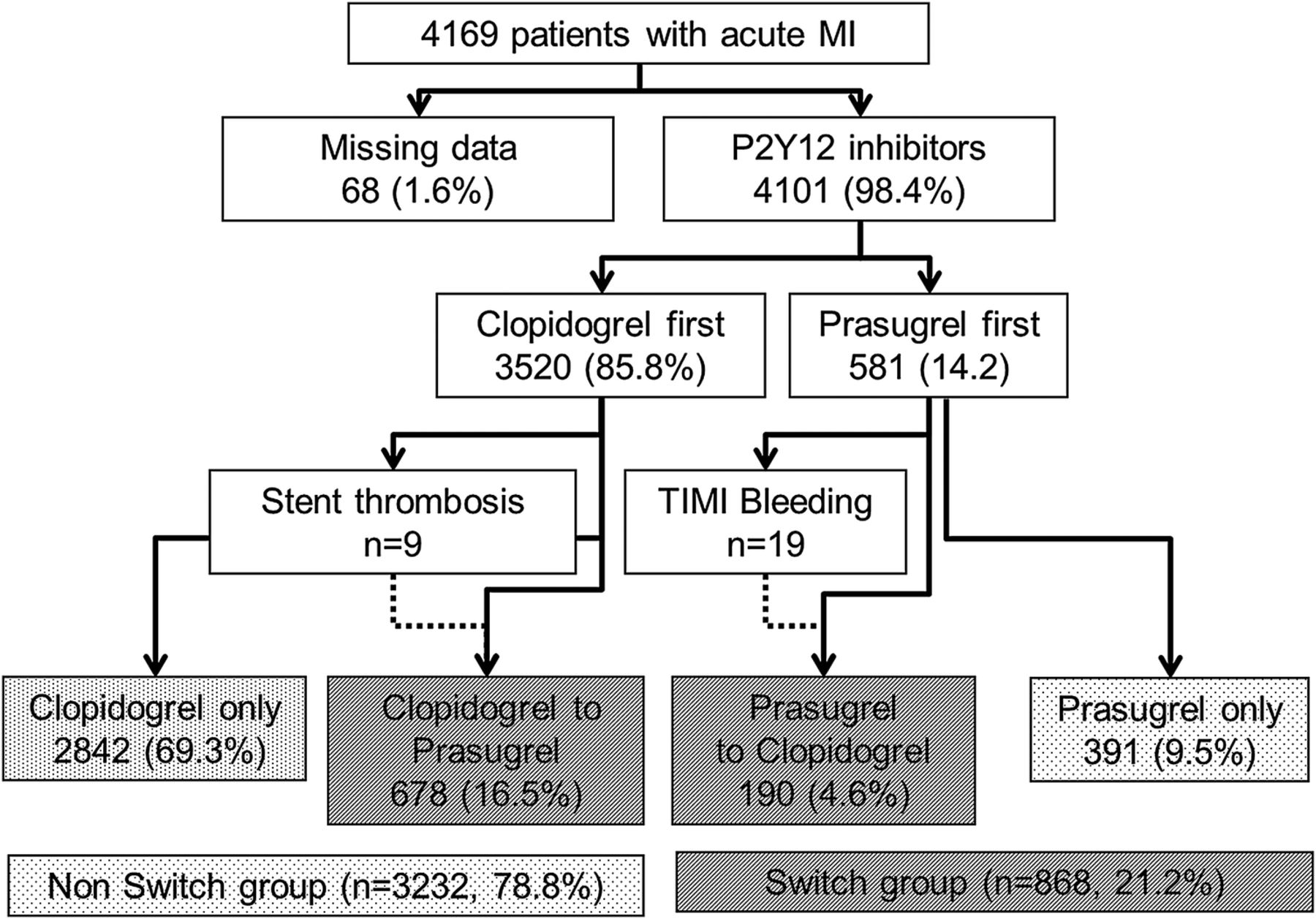
Among 4970 patients screened in 213 participating centres, 552 were excluded because they did not meet the criteria for AMI, and 249 refused to participate. Overall, 4169 patients were eligible, of whom 4101 received thienopyridines at admission (3520 (85.8%) clopidogrel, 581 (14.2%) prasugrel). The use of prasugrel as initial thienopyridine was related to the type of MI (437 (19.8%) patients with STEMI and 144 (7.5%) patients with non-STEMI (NSTEMI)). During hospitalisation, 3233 (78.8%) patients had no switch: 2842 (69.3%) were treated with clopidogrel and 391 (9.5%) with prasugrel. Conversely, 868 (21.2%) patients had a switch during hospitalisation: 678 (16.5%) from clopidogrel to prasugrel and 190(4.6%) from prasugrel to clopidogrel (figure 1).

Flow chart of the study population according to thienopyridines used in the FAST-MI registry in patients with STEMI and NSTEMI. FAST-MI, French Registry on Acute ST-elevation and non ST-elevation Myocardial Infarction; MI, myocardial infarction; NSTEMI, non-ST segment elevation myocardial infarction; STEMI, ST segment elevation myocardial infarction.
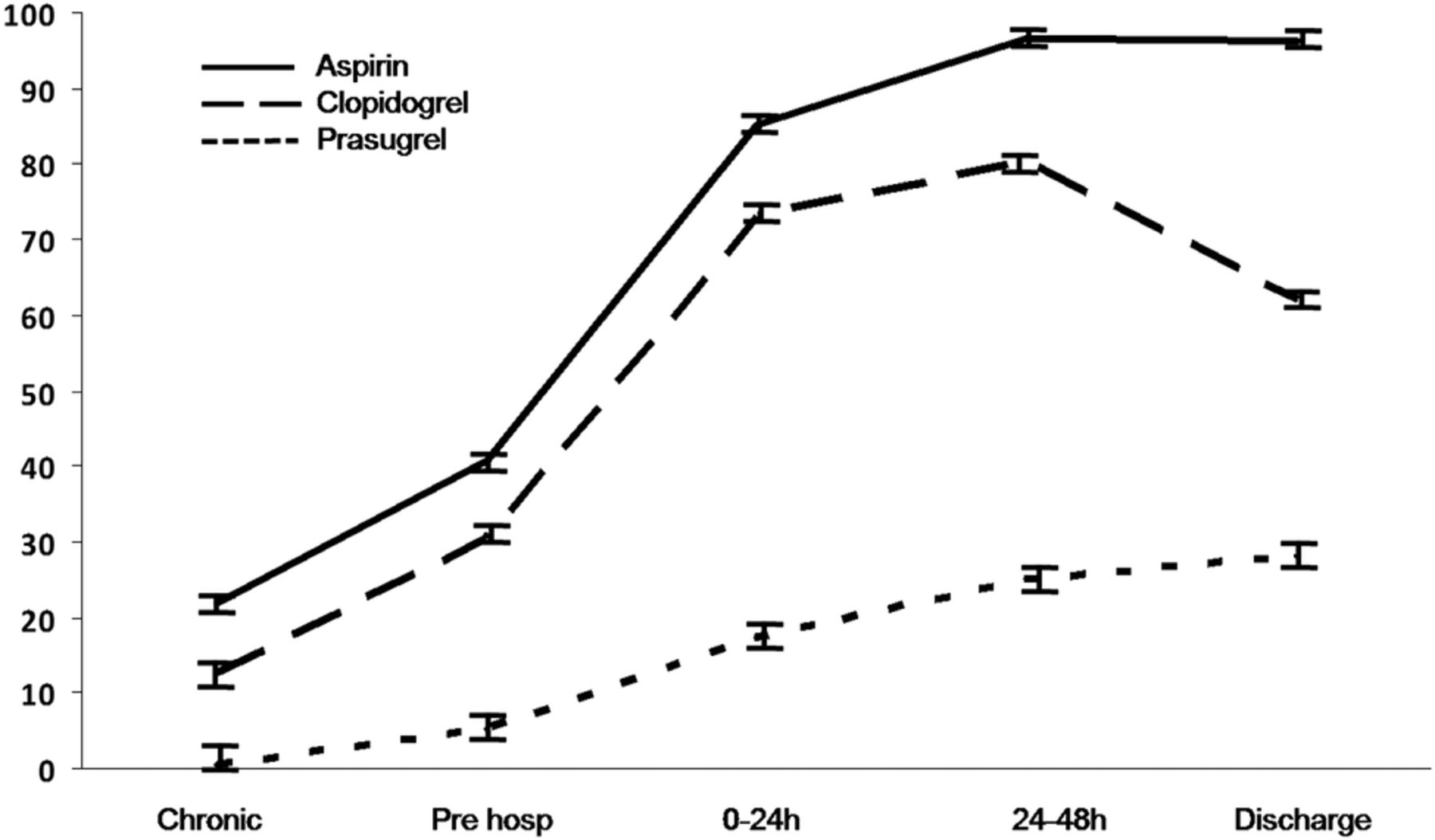
Modalities and appropriateness of switch: Aspirin and clopidogrel were introduced in the prehospital setting more often than prasugrel. After 2 days, the rate of clopidogrel use decreased due to the switch to prasugrel (figure 2). In the clopidogrel group, 48% of patients received a loading dose of 300 mg and 30% received 600 mg or more. When prasugrel was used as the first thienopyridine, a loading dose of 60 mg was given in 64%, but when patients were switched to prasugrel, only 8.3% receive a loading dose (table 1).
Eligibility criteria for P, and appropriate choice of C or P at admission and at discharge in the four groups

Proportion of patients receiving oral antiplatelet agents at each time point (pretreatment, prehospital, admission to 24 hours, 24–48 hours and at discharge).
At admission, eligibility for prasugrel ranged from 42.9% to 59.6% in the groups treated with prasugrel at any time. Non-eligibility for prasugrel in the clopidogrel-only group mainly reflected the high proportion of patients older than 75 years (40.4%), and without a definite indication for PCI (100%−28.3%=71.7%). Among patients with a switch from clopidogrel to prasugrel, 9 had stent thrombosis during hospitalisation and among those with a switch from prasugrel to clopidogrel, 19 had a major bleeding event. At discharge, eligibility for prasugrel was 82.1–86.1% in the groups treated with prasugrel at any time. Therefore, appropriateness of the switch was high (86%) from clopidogrel to prasugrel, but low (20%) from prasugrel to clopidogrel. In addition, 39.4% in the clopidogrel-only group would have been eligible for a switch from clopidogrel to prasugrel and 16.4% in the prasugrel-only group would have been eligible for a switch from prasugrel to clopidogrel (table 1).
Predictors of switching: Compared with patients who received prasugrel at any time (ie, patients with a switch in thienopyridines or those treated with prasugrel alone), those treated with clopidogrel alone were older, more often women, more often had NSTEMI, more comorbidities, a higher GRACE risk score at admission and higher in-hospital and 1 year mortality (table 2).
Baseline characteristics, conditions at admission, management and outcomes according to P2Y12 use during hospitalisation in the FAST-MI registry
Independent predictors of a switch were presentation with STEMI, admission to a non-cardiology emergency unit, history of previous PCI, lower quartile of age, body weight>60 kg, no cardiac arrest, no stroke, no anaemia and no renal dysfunction (figure 3). The model had adequate discrimination (c-stat=0.77) and calibration (p value for the Hosmer-Lemeshow test=0.45).

Forest plot of ORs for the predictors of switch in thienopyridines. STEMI, ST segment elevation myocardial infarction; ED, emergency department; PCI, percutaneous coronary intervention.
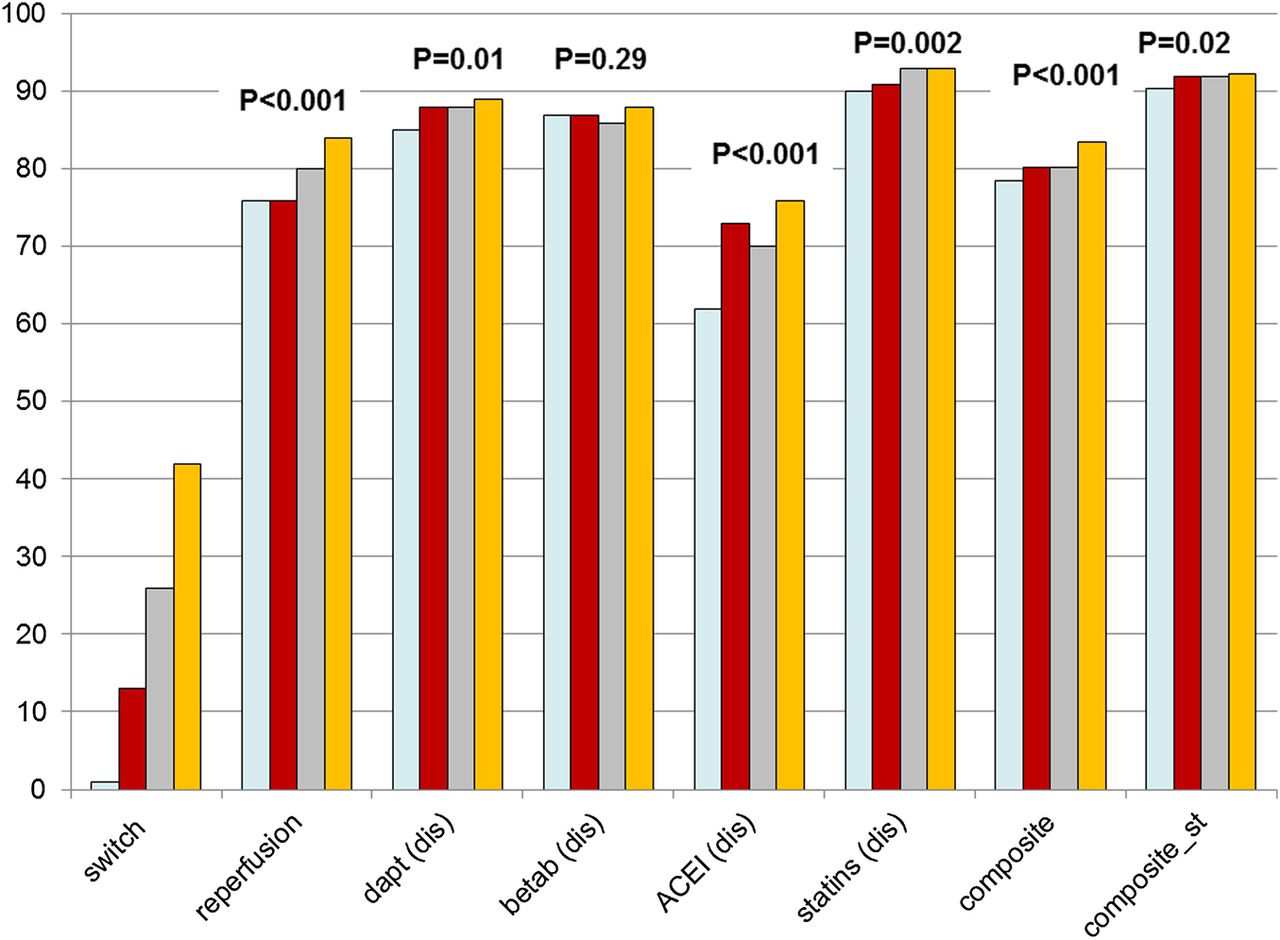
Switch and quality of care: A significant interaction was observed between the centre and the rate of switching (p=0.006). Among the 213 participating centres, 59 (28%) never performed a switch. Four categories of centres were defined according to their switching rates: from 0% to 7% (n=75), from 8% to 18% (n=51), from 19% to 33% (n=46) and >33% (n=41). With increasing switch categories, there was a trend towards higher rates of use of coronary angiography, GPIIbIIIa inhibitors, radial access, reperfusion (for patients with STEMI, either by primary PCI or thrombolysis), timely reperfusion, and DAPT, ACE inhibitors and statins at discharge. As a result, there was a significant trend towards an increase in the composite indicator (for all MI and for STEMI) with higher rates of switching (table 3 and figure 4).
Patient characteristics and management according to the rate of switch by centre
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rates of quality indicators across categories of centres (according to the rate of switch). DAPT, dual antiplatelet therapy; betab: β-blockers, ACEI, ACE inhibitors; dis, discharge; composite, composite indicator calculated using opportunity scoring (one point by applicable indicator divided by the number of applicable indicators); composite_st, composite indicator for patients with ST elevation myocardial infarction (including reperfusion within 120 min by primary percutaneous coronary intervention or within 60 min by thrombolysis).
Discussion
Our results provide insights into the rates and modalities of switching between thienopyridines, and raise questions about the appropriateness of switching drugs when the initial thienopyridine choice appears suboptimal.
Modalities and rates of switching
A switch was performed in 21.2%, and more often from clopidogrel to prasugrel than vice versa. Thus, switching thienopyridines from a less potent to a more potent inhibitor is common practice. The modalities of prescription of thienopyridines at admission and at discharge after ACS were previously investigated in a study from 2012 based on data from the GRAPE registry.9 At the time, ticagrelor was already available, which considerably increased the number of possible combinations of treatment. The GRAPE study used a similar definition of appropriate P2Y12 inhibitor treatment as in our study, and their findings are also in line with those from the FAST MI registry; namely, at admission, initial selection was considered appropriate in 45.8%, less preferable in 47.2% and inappropriate in 6.6%. In the majority of cases, an initially less-preferable selection was due to prescription of clopidogrel when in fact the patient was eligible for prasugrel or ticagrelor. Switches in therapy made it possible to achieve appropriate prescription in 64.1% at discharge. Our results are in line with those from the merged Acute Coronary Treatment and Intervention Outcomes Network Registry-Get with the Guidelines and CathPCI registry, where, among 47 040 patients, a switch from clopidogrel was performed in 5.2% and from prasugrel to clopidogrel to prasugrel in 11.5%.4 Analysis of the first dose of thienopyridine in our study showed that half the patients who were switched did not receive a loading dose for the second thienopyridine. This prudent attitude is coherent with published data showing greater platelet inhibition after a switch from clopidogrel to prasugrel in stable10 ,11 and unstable patients,12 ,13 compared with clopidogrel alone, regardless of the loading13 or maintenance11–13 doses.
Reasons for switching
Our results suggest that the decision to switch was based on three main reasons: (1) the need to tailor platelet inhibition according to an in-hospital adverse event, (2) compliance with the labelling of prasugrel based on information not available at admission and (3) the expectation of better long-term clinical outcome by changing the thienopyridine, according to the results of the TRITON and TRILOGY studies.
A small proportion of switches were explained by in-hospital complications. Indeed, 19 (10%) patients had a major bleeding and were switched from prasugrel to clopidogrel, while 9 (1.3%) patients with stent thrombosis were switched from clopidogrel to prasugrel. The second explanation for a switch was compliance with the labelling of prasugrel and this largely explained the switching from prasugrel to clopidogrel. The last explanation for a switch was the expectation of better outcomes with a change from clopidogrel to prasugrel based on the results comparing clopidogrel and prasugrel.
Switching from clopidogrel to a more potent inhibitor (ticagrelor) was shown to be effective in the PLATO trial, without any apparent excess of events,14 and is recommended by guidelines.15–18 This explained a large proportion of the switches from clopidogrel to prasugrel. In this group, the appropriateness of switching practices was high, but did not reach 100%. Nevertheless, although a small proportion of patients were not eligible for prasugrel, none had a strong contraindication, such as previous stroke or TIA.
The predictors for a switch were analysed globally, without distinguishing between directions of the switch, as in the reports by Bagai et al.3 ,4 The results suggest that a switch was not used to correct initial misuse of prasugrel, since older age, previous stroke and low body weight were associated with a low switch rate.
Switch use and quality of care
A switch from one drug to another, when the initial choice seems suboptimal, is usually considered as a positive action. In this view, switching thienopyridines for a more appropriate treatment might thus be considered to be good medical practice. There was a trend towards higher scores on quality indicators with increasing rates of switching, as shown by the higher rates of reperfusion, greater avoidance of complications (eg, use of radial access) and more compliance with guidelines for discharge treatment across categories of centres. Given that centres with a low rate of switching were also the centres that performed less well in terms of application of guidelines for reperfusion and discharge medication, it is unlikely that the low switch rate is a reflection of excellent initial treatment choices in these centres.
According to current methodology for the definition of performance measures,19 a switch in thienopyridines cannot per se be considered as an indicator of quality of care. Conversely, the appropriateness of the thienopyridine during hospitalisation and at discharge could be used as an indicator of quality since the use of prasugrel or ticagrelor instead of clopidogrel in eligible patients is evidence-based and supported by a IB recommendation in the European Society of Cardiology (ESC) guidelines; 15 ,20 ,21 furthermore, it is interpretable, actionable and its assessment is most likely feasible.
Study limitations
Our findings, although resulting from a large cohort, are derived from observational analyses, which are subject to well-known limitations. First among these is the potential for confounding by measured or unmeasured variables, which cannot be completely ruled out. Therefore, caution is advised in interpreting these results. Second, our ‘quality indicators’ are only rates of use and do not consider potential contraindications. Third, the term ‘appropriate’ was used to describe whether the prescriptions at discharge were in accordance with the labelling for each drug, in view of the patient's characteristics. This should under no circumstances be construed to imply superiority of either treatment. Lastly, owing to the retrospective nature of this study, the exact reasons for switching were not recorded, but simply deduced from the clinical characteristics of the patients. For example, it is possible that for the assessment of eligibility, certain justified contraindications to one or other therapy were not recorded.
Conclusion
The findings of the FAST-MI registry underline the complexity of choosing appropriate thienopyridine treatment in routine practice in patients with AMI when only clopidogrel and prasugrel are available. During hospitalisation, in a substantial proportion of patients, the thienopyridine initially prescribed is considered to have been suboptimal, leading to a switch to another drug. As applied in the FAST-MI registry, the switch in thienopyridines was performed according to the labelling of the drugs, and was associated with higher rates of quality of care indicators.
References
Footnotes
Contributors ND and TS were involved in study conception and design. All authors were involved in data collection. FS, NM and ND were involved in statistical analysis. FS, NM, ND and TS were involved in drafting of the manuscript. All authors were involved in critical revision of the manuscript, and approval of final version for publication.
Funding FAST-MI is a registry of the French Society of Cardiology, supported by the Société Française de Médecine d'Urgence, SAMU de France, the Collège National des Cardiologues des Hôpitaux and the Collège National des Cardiologues Français. The study was sponsored by the French Society of Cardiology and funded by unrestricted grants of the following companies: MSD, AstraZeneca, the Daiichi-SankyoEli-Lilly alliance, GlaxoSmithKline, Novartis and sanofi-aventis.
Competing interests FS reports research contracts and consulting with sanofi-aventis, astra, MSD, Bristol Myers Squibb, Amgen and Pfizer. TS has received research grants from Pfizer and Servier for the FAST-MI registry; served as a board member for Bayer; and has given lectures to Sanofi and Lilly. ND reports grants, personal fees and non-financial support from Amgen, grants, personal fees and non-financial support from AstraZeneca, grants and personal fees from Daiichi Sankyo, grants, personal fees and non-financial support from Eli Lilly, personal fees from BMS, personal fees from GSK, grants and personal fees from MSD, grants and personal fees from Novartis, personal fees from Novo-Nordisk, grants and personal fees from Pfizer, personal fees from Roche, grants, personal fees and non-financial support from Sanofi, and personal fees and non-financial support from Servier, outside the submitted work.
Patient consent Obtained.
Ethics approval Committee for the Protection of Human Subjects of Saint Louis University Hospital Paris Ile de France IV, Paris, France.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.