Article Text

Abstract
Objective We sought to investigate the incidence of complications associated with V2 Guideliner, understand the mechanisms and evaluate the impact of alterations made to the V3 Guideliner.
Methods Retrospective analysis of consecutive cases employing V2 Guideliner from two university teaching hospitals. Complications were identified, analysed and classified into major versus minor ones. To understand the potential anatomical mechanism of these complications, analysis of normal great vessel anatomy was undertaken in separate cohort of patients undergoing cardiac catheterisation via right radial approach. Further analysis of consecutive cases employing V3 Gudieliner took place and the incidence of complications were compared between V2 and V3 groups.
Results Total of 188 cases of V2 Guideliner use were identified. One major complication was reported (coronary dissection). Proximal collar interaction and stent damage occurred in 19 cases (10%). Anatomical data suggest that extending the V2 Guideliner tubing sited the proximal collar of the device in the brachiocephalic/subclavian artery, a potential site of tortuosity and potential cause of the Guideliner proximal collar-stent interaction. Further analysis of 124 cases of V3 Guideliner use demonstrated no cases with proximal collar-stent interactions, one case of longitudinal stent deformation and two incidents of stent interaction with the distal edge of the V3 Guideliner.
Conclusions We have demonstrated a higher incidence of V2 Guideliner complications compared to previous series. The change in design of the V2 Guideliner was a likely contributor but the modifications with V3 Guideliner appear to have ameliorated this issue.
- CORONARY ARTERY DISEASE
- Guideliner
- percutaneous coronary intervention
- complex lesion
- Subclavian artery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
The use of a Guideliner facilitates complex coronary intervention. Reported studies have been small in number and complications’ rates varied significantly according to the Guideliner version and the chosen access route. Data on the newest generation V3 are sparse.
What does this study add?
In our experience the V2 Guideliner catheter was associated with a higher incidence of complications compared with published data, in particular when using the right radial approach. Our study provides mechanistic explanation to the complications in the V2. In addition, it highlights the benefits of the newest V3 Guideliner generation.
How might this impact on clinical practice?
While the V3 Guideliner appears to have eliminated the proximal collar/stent interaction there are now many types of guide extension catheters on the market. They are modelled on the V2 version (Guidezilla, Boston Scientific and Guidion, IMDS). Both these are 25 cm and have a similar proximal collar. Whether they have similar failure rates to the V2 remains to be seen.
Introduction
Coronary percutaneous intervention is becoming increasingly challenging due to a variety of factors and delivering often long stents into heavily calcified, tortuous coronary arteries can be problematic.1
A number of strategies have evolved over time in order to assist stent delivery. These include the use of a ‘buddy wire’, the Heartrail II system (Terumo, Japan) which was the first guide catheter extension and more recently the Guideliner (Vascular Solutions, Minneapolis, USA) monorail system has been introduced.2 This device has been transformative to our practice. This device consists of flexible, soft-tipped extension tubing with a metallic proximal collar, attached to a thin stainless steel shaft (figure 1). The Guideliner extension is advanced over a coronary guidewire through the standard haemostatic valve using a ‘monorail’ technique to facilitate stent delivery in calcific and/or tortuous vessel.3 ,4

(A) First version of Guideliner with a metal proximal collar. (B) Second Version of Guideliner with a polymer proximal collar. (C) Third version of Guideliner with a polymer collar and proximal half-pipe lead in.
One of the commonest complications associated with the first generation Guideliner was the interaction between a stent that was being delivered and the proximal collar.2 ,4 Subsequently, the second generation of the Guideliner catheter (V2) was introduced. The metal collar on the V1 catheter was changed to an all-polymer collar (figure 1). The rapid exchange section was extended from 20 to 25 cm to potentially allow deeper intubation into the target vessel. This was in response to consumer feedback. These features were included in the design of at least two other guide extension catheters (Guidezilla Guide Extension Catheter, Boston Scientific, Boston and Guidion Flexible Guide Extension, IMDS, the Netherlands) with a 25 cm catheter with a polymer proximal collar.
In a predominately radial access centre it was our impression that these changes with the V2 Guideliner had not reduced the incidence of complications in routine practice. Therefore, an audit of the use of the V2 Guideliner in clinical practice was undertaken. We then sought to understand the relationship between a right transradial approach to the coronaries and the proximal edge of the V2.
Guideliner by performing an analysis of normal great vessel and aortic anatomy.
Finally we undertook another audit of the V3 Guideliner to assess if the next iteration had overcome the limitations of the V1 and V2 devices. With the V3, the 25 cm rapid exchange section was maintained but with an additional 17 cm ‘half-pipe’ segment proximal to the collar transition to minimise stent and collar interaction by directing and aligning stents through the collar transition (figure 1).
Methods
A retrospective analysis of all cases employing a V2 Guideliner between January-2011 and November-2012 was performed. All cases where complications occurred related to the V2 Guideliner use were recorded and retrospectively analysed.
To help understand the increased failure rate with V2 a descriptive study was undertaken to explain the relationship between a right transradial approach for coronary intervention and the normal aortic and large vessel anatomy.
During planned procedures, a marker catheter was introduced via the right radial artery to sit with its tip on the aortic valve (on the right coronary cusp). A fluoroscopic image of the marker catheter was recorded in the anterioposterior projection and this was used to create a range of measurements of large vessel anatomy for a range of patients. Bony landmarks were used to define anatomy (figure 2). The initial measurement was from the aortic valve to a line drawn between the lower borders of both clavicular heads. This correlates with transition into the right subclavian artery. The distance from this point to where the catheter reached its most superior location was also measured. Finally, the distance to where the catheter crossed the most distal clavicular border was measured. This reflects the transition from the subclavian to the axillary artery. As a result, a second audit was undertaken after the incidence and nature of complications related to the V2 Guideliner were understood. A retrospective analysis of all cases employing a V3 Guideliner between August 2013 and November 2014 was undertaken (124 cases). All cases where complications occurred related to the V3 were also recorded and retrospectively analysed.
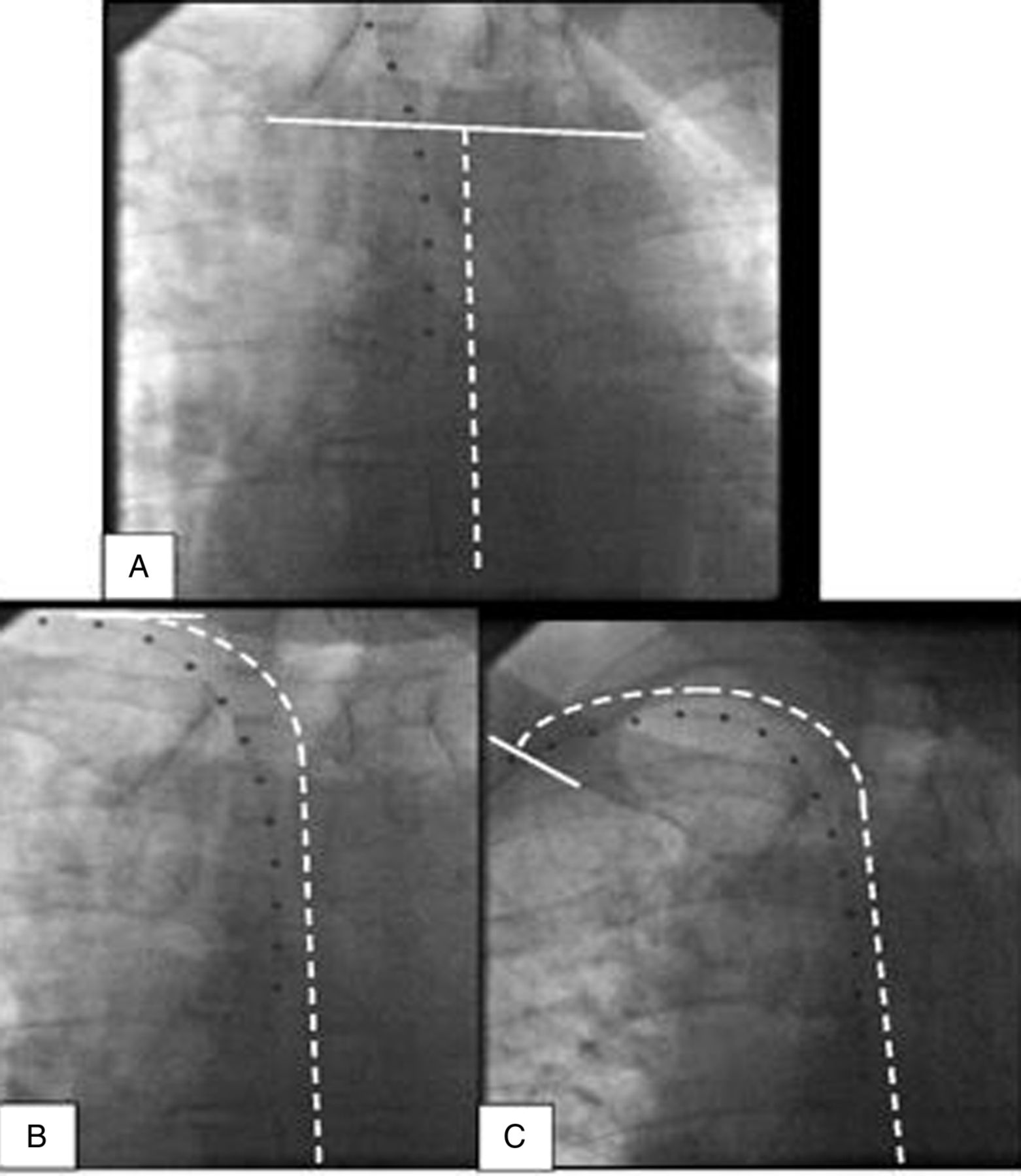
(A) Fluoroscopic image of our marker catheter in an anterioposterior projection shows measurements taken from the aortic valve to a line drawn between the lower borders of both clavicular heads (inferior border). (B) Fluoroscopic image shows distance from aortic valve to the point to where the catheter reached its most superior excursion (superior border). (C) Fluoroscopic image shows the distance to where the catheter crossed the most distal clavicular border (posterior border).
Results
Experience with the V2 Guideliner
A total of 188 cases were identified where the V2 Guideliner was used. Technical success during the procedure was defined as PCI with successful stent deployment and <20% residual stenosis. Procedural success was defined as technical success and where no major or minor complications related to the V2 Guideliner device occurred. Major complications were defined as those that led to further additional unplanned intervention (by PCI or surgery) or any major adverse cardiovascular events (death or myocardial infarction). Minor complications included any technical complication that led to equipment damage or a failure to complete the planned PCI.
Baseline demographics of the cohort are presented in table 1
Comparison between V2 and V3 Guideliner patient and lesion characteristics
Technical success was achieved in 183/188 cases (97%). Stent delivery was attempted but failed for the target lesion in five cases. In one case, right coronary artery dissection also occurred as a result of the Guideliner use. This occurred during an intervention for ST elevation myocardial infarction. Hydraulic dissection extending into the proximal segment of the vessel occurred as a result of contrast injection. This was covered with a stent with a good angiographic result and distal flow was successfully restored with POBA (plain old balloon angioplasty). This patient ultimately had a successful coronary artery bypass operation later in the hospital admission. This event was classified as the only major complication related to Guideliner use and also qualified as a technical failure, although there were no major adverse clinical sequelae for the patient. The other four patients were managed medically without any inpatient complications as a result of the inability to stent the target lesion.
The minor complications encountered can be split into two main categories.
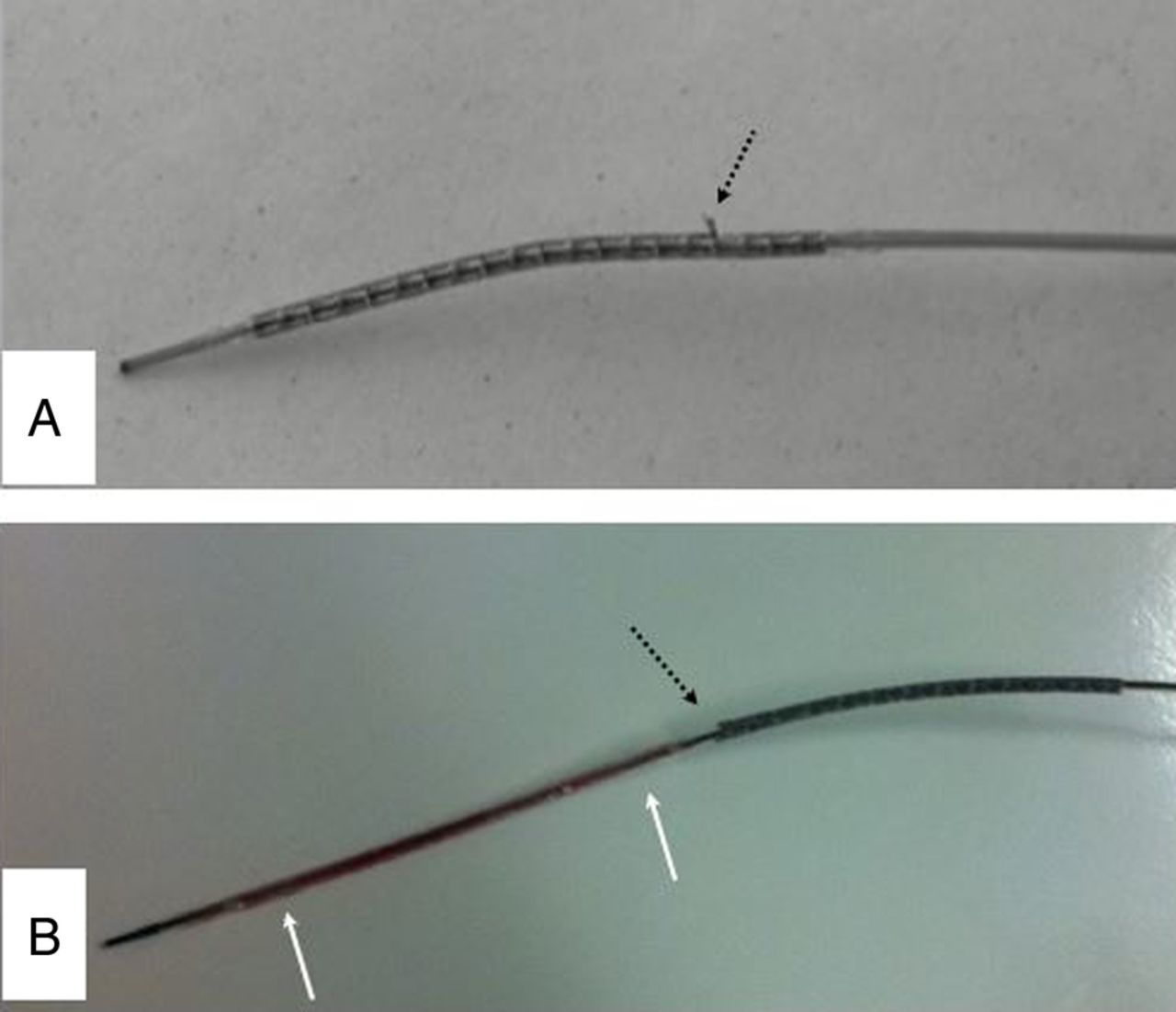
Proximal collar and stent interactions: This included stent deformation (figure 3A) or stripping (figure 3B) in 19 cases (10%). There included one case of the proximal collar cutting into a stent delivery balloon shaft as the Guideliner was withdrawn backwards to ‘unsheathe’ a delivered stent.5 This meant the delivery balloon could not be expanded and that the stent had to be withdrawn undeployed. We have already described a similar issue previously.5

{kind=link}
{kind=link}
{kind=link}
(A) Image of a stent that was damaged withdrawing it back into a Guideliner V2 after failing to cross the lesion. A proximal strut has been distorted (black arrow). (B) Image of a stent which interacted with proximal collar of Guideliner V2 resulting in it being stripped off the balloon (white markers) and damaging the leading struts (black arrow).
Longitudinal stent deformation within the target vessel: This occurred in two cases, where there was evidence of damage to already deployed stents caused directly by the V2 Guideliner extension tip. One case was of damage to a pre-existing bare metal stent. The second case involved damage to a previously implanted drug eluting stent (Promus Element 4.0×38 mm; Boston Scientific, Nattick, Massachusetts, USA). The latter stent was deployed 6 months prior to Guideliner use; while the bare metal stent in the first case was 13 years old (procedural data from this implant could not be obtained).
Therefore, a total of 22 cases demonstrated any procedural complication with 1 major (already qualified as a technical failure) and 21 minor complications.
There were four other cases of failed stent delivery. Therefore, the procedural success associated with Guideliner use was 86% (26/188 unsuccessful cases or cases where any complication occurred). This was higher than the reported data for V1 and we felt the additional 5 cm length with the V2 may have contributed and thus undertook the second part of the project.
Description of subclavian artery anatomy
A total of 46 patients were included for this analysis. The mean age was 65 (±11.5) and 30 (66%) were male. Mean height was 168 cm (±9); with a mean weight of 84 kg (±19) and body mass index of 29.6 (±5.7). Examples of where the measurements were taken are demonstrated in figure 2. The mean distance from the tip of the measuring catheter to the inferior border of clavicular heads was 109 (±19) mm. The mean distance to the most superior segment of the clavicle was 137 (±18) mm. Finally, the mean distance to the most posterior border of the clavicle was 193 (±19) mm.
Experience with the V3 Guideliner
A total of 124 cases were identified and analysed. Technical and procedural success (defined previously) were 118/124 cases (95%) and 115/124 cases (93%), respectively.
The V3 group had some features of increased complexity compared with the V2 group (table 1), more frequent Chronic Total Occlusion, more stents per case (2.5+/−1.43 vs 1.8 +/−0.81, p=0.0001), and longer stent length (59 +/−83 vs 50 +/−26, p=0.17). However the calcification and tortuosity scores suggested the V2 group were a more complex group. So the differences probably cannot be explained by the patient factors.
In four cases stent delivery was deemed extremely difficult and the procedure was concluded with POBA only. Haematoma secondary to lesion disruption led to procedure abandonment in one case and inability to wire the target vessel was the cause of technical failure in another case. All patients made a complete recovery and were subsequently discharged without any clinical sequelae. No major complications were reported.
There were no proximal collar/stent interactions reported with the V3 Guideliner use. Three minor complications were noted due to stent interaction with the distal edge of the V3 Guideliner. One longitudinal stent deformation of a 1-year old drug eluting stent (Resolute Integrity 3.0×38 mm, Medtronic Inc, Minneapolis, Minnesota, USA) was noted and covered with a further 3.5×9 mm Resolute Integrity DES. Two stents were stripped off the balloon during an attempt to withdraw the stents back into the guide system. This interaction occurred at the leading edge of the V3 Guideliner. Both were Promus Element stents (Boston Scientific, Nattick, Massachusetts, USA) and were 2.75×20 mm and 2.5×38 mm sizes. These PCI cases were completed without complication.
Discussion
This case series demonstrates a high incidence of proximal collar interactions between the V2 Guideliner and stents. We have shown a higher incidence of this complication (10% of cases) compared with other historical V1 data (range 0–6%).2 ,4 ,6 We felt this was in part related to the high radial use in our centre.
Lengthening the extension tube to 25 cm was one of main changes from the V1 to V2 Guideliner, altering the interface between the proximal collar and a stent by bringing this area more proximally possibly aiding alignment.5
The need to use guide catheter extension is more common in our experience using smaller calibre guide catheters from a transradial approach. In general, the Guideliner is advanced only a few centimeters into the target vessel, rarely more than 10 cm. Its length of 25 cm will therefore frequently place the proximal collar within the brachiocephalic and right subclavian segments (averaged at 10–20 cm in most patients).
We demonstrated that the average distance from the right coronary cusp to the posterior border of the clavicle was 193 mm.
With advancing age, the aorta and subclavian artery becomes angulated, tortuous and elongated. We speculate that if the proximal collar resides in this area it is subject to ovoid distortion with respiration. Any ovoid distortion will create a potential space between the guide catheter and the Guideliner and allow interaction with the stent. In contrast, the V1 Guideliner proximal collar will have resided within the ascending aorta and the metal collar less susceptible to distortion.
Our experience with the V3 Guideliner would support this hypothesis. There were no cases of proximal edge/stent interaction in the second series. The half-pipe technology appear to, at least in our experience, align the stent and ensure minimal interaction with the semicircular polymer collar transition (figure 1). There were minor differences between the patient populations (table 1). However, despite delivering more stents per case with the V3 Guideliner this was still associated with lower complication rates. Thus it appears that the newer iteration has minimised the potential for proximal collar and stent interactions.
Conclusion
Our data suggest that the V2 Guideliner catheter had a higher incidence of complications - particularly stent/proximal collar interaction, especially when using the right radial approach, compared with V1 historical data. The change in design of the V2 Guideliner from the V1 was a likely contributor (extending from 20 to 25 cm, modifying the proximal collar from metal to plastic). These changes place the proximal collar of the device in the right brachiocephalic or subclavian artery, a potential site of tortuosity. Subsequent analysis demonstrates that the further modifications with the latest Guideliner version (V3) seems to have ameliorated these complications when compared with older generation.
Footnotes
Contributors MA contributed to the design of the study, data acquisition, statistical analysis, and drafted the manuscript. AS contributed to data acquisition and drafting the manuscript. SJW initiated the concept of the study, revised the intellectual content and contributed to the statistical analysis. CMcQ contributed to data acquisition and drafting the manuscript. MSS contributed to the concept of the study and drafting the manuscript. CGO contributed to the concept of the study and drafting the manuscript. CGH initiated the concept of the study, revised the intellectual content and had the final approval of the published version. All authors declare that they are accountable to all aspects of the work in relation to the accuracy and integrity of any part or the whole published paper.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.