Article Text

Abstract
Background Average life expectancy is rising, resulting in increasing numbers of elderly, frail individuals presenting with coronary artery disease and requiring percutaneous coronary intervention (PCI). PCI can be of value for this population, but little is known about the balance of benefit versus risk, particularly in the frail.
Objective To determine the relationship between frailty and clinical outcomes in patients undergoing PCI.
Methods Patients undergoing PCI, for either stable angina or acute coronary syndrome, were prospectively assessed for frailty using the Canadian Study of Health and Ageing Clinical Frailty Scale. Demographics, clinical and angiographic data were extracted from the hospital database. Mortality was obtained from the Office of National Statistics.
Results Frailty was assessed in 745 patients undergoing PCI. The mean age of patients was 62±12 years and 70% were males. The median frailty score was 3 (IQR 2–4). A frailty score ≥5, indicating significant frailty, was present in 81 (11%) patients. Frail patients required longer hospitalisation after PCI. Frailty was also associated with increased 30-day (HR 4.8, 95% CI 1.4 to 16.3, p=0.013) and 1 year mortality (HR 5.9, 95% CI 2.5 to 13.8, p<0.001). Frailty was a predictor of length of hospital stay and mortality, independent of age, gender and comorbidities.
Conclusions A simple assessment of frailty can help predict mortality and the length of hospital stay, and may therefore guide healthcare providers to plan PCI and appropriate resources for frail patients.
- Frailty
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Frailty has emerged as a marker of biological age and it may help predict adverse events in elderly population.
Frailty has been shown to predict postoperative complication and to correlate with quality of life, hospital admissions and mortality, independent of age, gender and comorbidities.
What does this study add?
This study highlights the association of Canadian Study of Health and Aging Clinical Frailty Scale with length of hospital stay, 30-day mortality and 1 year mortality after percutaneous coronary intervention. This association is independent of age and other conventional risk factors and comorbidities.
How might this impact on clinical practice?
Canadian Study of Health and Aging Clinical Frailty Scale is a simple and quick tool to assess frailty. It can provide additional prognostic information, complementing conventional risk scores and guide healthcare providers to plan percutaneous coronary intervention and appropriate resources for frail patients.
Introduction
Patients with symptomatic, significant or unstable coronary artery disease usually require coronary revascularisation, either with percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG).1 ,2 Life expectancy is rising,3 resulting in increasing numbers of elderly people presenting with coronary artery disease.4 Clinical decision-making for this elderly population is challenging because little is known about what treatment choices will benefit them, because older patients are often excluded from clinical trials and usually have multiple comorbidities.5–7 Traditionally, a conservative approach is adopted for many elderly patients, yet this cohort often has high-risk disease and might benefit the most from intervention.8–10 The association between age and mortality reduces significantly when corrected for other biological factors, such as comorbidity, cognition, social and functional status, which suggests that other factors, distinct from age, are relevant.5
Frailty assessment has emerged as a measure of biological age and it may help predict adverse events in elderly population. Frail patients represent a high-risk population, and frailty is a risk factor for falls, disability, institutionalisation and death.11 Frailty has been shown to predict postoperative complications and mortality in elderly patients undergoing cardiac surgery12 and to correlate with quality of life, hospital admissions and mortality, independent of age, gender, and comorbidities.13–15 It has been recently shown that addition of the Fried Frailty Index improves the discriminative ability of the Mayo Clinic PCI score for predicting angioplasty outcomes.16 ,17 However, the Fried Frailty score is not readily measurable, especially in acute clinical situations, because it includes grip strength measurement with a dynamometer, a 6 min walk test and a detailed quality of life questionnaire.
This study aimed to determine whether a simple assessment of frailty using Canadian Study of Health and Aging Clinical Frailty Scale18 can help predict adverse outcome after PCI, including mortality and length of stay in hospital.
Methods
This prospective study consisted of unselected patients undergoing PCI at the South Yorkshire Cardiothoracic Centre in Sheffield, UK. Sheffield is a tertiary centre providing the revascularisation facilities for a catchment population of 1.8M people in the north of England. Patients undergoing PCI between March 2012 and March 2014 for stable angina or acute coronary syndrome were eligible for the study providing a frailty assessment was completed at the time of their PCI procedure. Patients admitted more than once during the study period were not double counted and only data from the first admission were used for analyses.
Data collection and outcomes
At the time of PCI, clinical information, including patient demographics, comorbidities and procedural details, were collected. Our centre routinely uses the New York PCI risk score for patients undergoing PCI and this score was calculated for each patient. The New York PCI risk score comprises nine variables: age, gender, haemodynamic state, ejection fraction, timing of myocardial infarction (MI), peripheral vascular disease, congestive heart failure, renal failure and left main stem stenosis19 and has been demonstrated to predict the risk of in-hospital death following PCI.19 Frailty was assessed using the Canadian Study of Health and Aging Clinical Frailty Scale.18 These data were collected as a service improvement project with institutional approval. It is a descriptive frailty scale ranging from one (very fit) to nine (terminally ill) (figure 1). This scale is quick and easy to implement, requiring simple questions to be asked to the patient to establish their level of frailty according to the descriptions associated with each category.
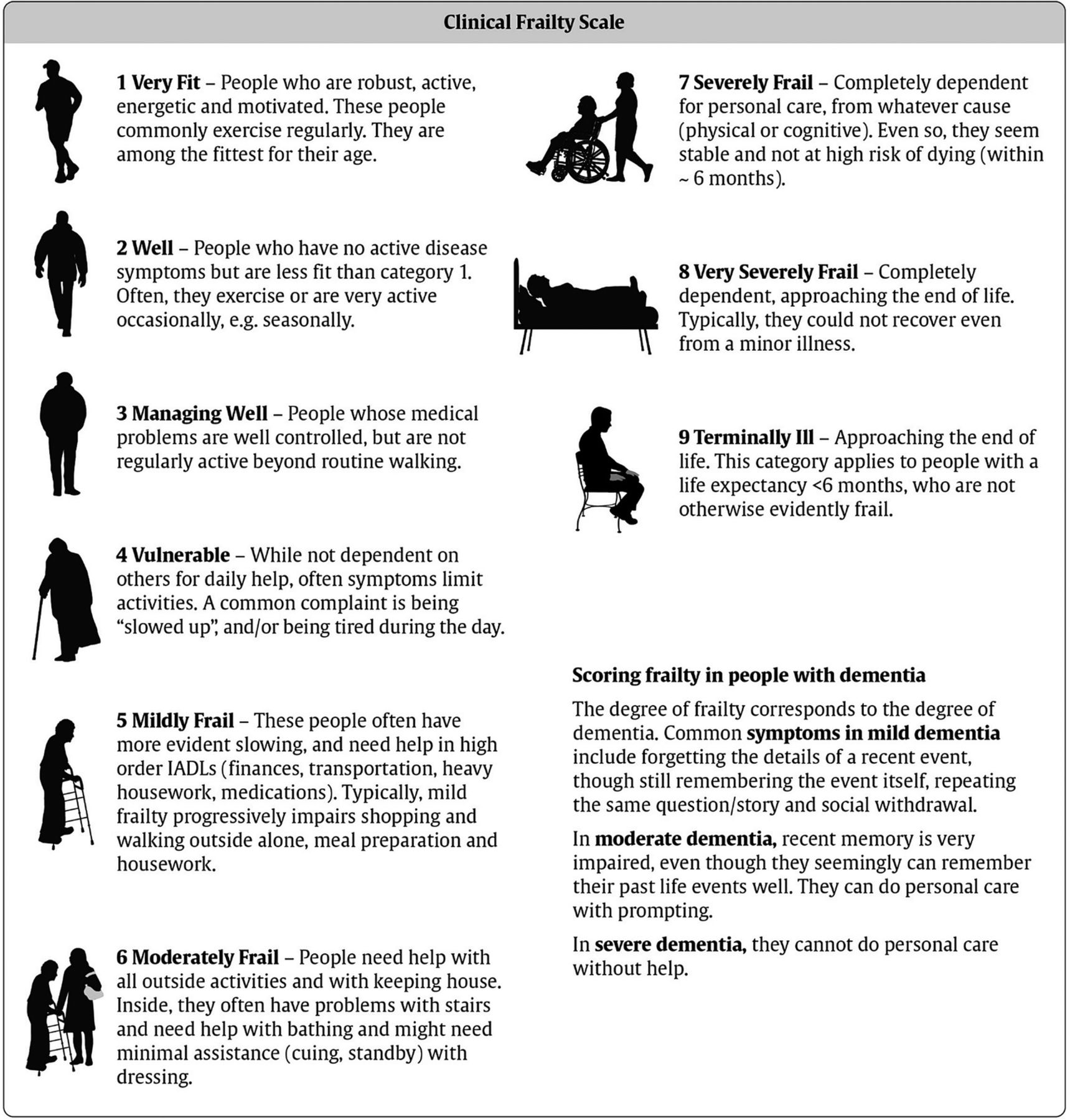
Canadian Study of Health and Aging Clinical Frailty Scale. Adapted from Rockwood et al.18
Study outcomes were length of hospital stay and mortality at 30-day and 1 year. Mortality data are routinely collected at the Office of National Statistics, UK.
Statistical analysis
Data are presented as mean±SD for continuous variables and counts or proportions for categorical variables. Data were analysed using Student t test for continuous variables and χ2 or the Fisher's exact test for categorical variables. Baseline clinical and procedural covariates with a significant trend (p<0.1) in the univariate analyses were considered candidate variables for multivariate model. Multivariate Cox regression analysis was used to identify the variables independently associated with outcomes. A two tailed p value <0.05 was used for statistical significance. All analyses were carried out using SPSS V.21 (IBM SPSS Inc, New York, USA).
Results
A total of 745 patients were investigated, with a mean age of 62±12 years, of which 70% (n=522) were male. The mean frailty score was 3.0±1.3 (median 3, IQR 2–4) and no patients had a frailty score higher than 7. The scale identified 81 (11%) patients with a score of 5–9. These were henceforth designated ‘frail’, versus patients with a score 0–4 ‘not frail’.
Baseline variables and frailty
Baseline variables are outlined in table 1. Frail patients were older, more likely to be female, and to have comorbid conditions, including lower left ventricular ejection fraction, peripheral vascular disease, a history of congestive heart failure, renal impairment, diabetes mellitus, hypertension and previous stroke. The overall predicted mortality risk from New York PCI risk score was 2.2±6.7%. Frail patients had substantially higher predicted mortality risk from New York PCI risk score than non-frail patients (7.4±15.6 vs 1.6±4.2%, p<0.001).
Patient characteristics in over-all population and according to frailty status
Length of hospital stay
The total length of hospital stay was documented in 576 (77.3%) of the patients (the missing data being due to interhospital transfer). The mean length of stay in hospital was 4.9±5 days (range 1–37 days). The time interval from admission to PCI was longer for frail patients (2.9±5.6 vs 1.7±3.1 days, p<0.001). After PCI, frail patients remained in hospital substantially longer than non-frail patients (14.1±26.7 vs 3.5±8.8 days, p<0.001; figure 2). Frailty was an independent predictor of the length of hospital stay in multivariate regression analysis (p<0.001).
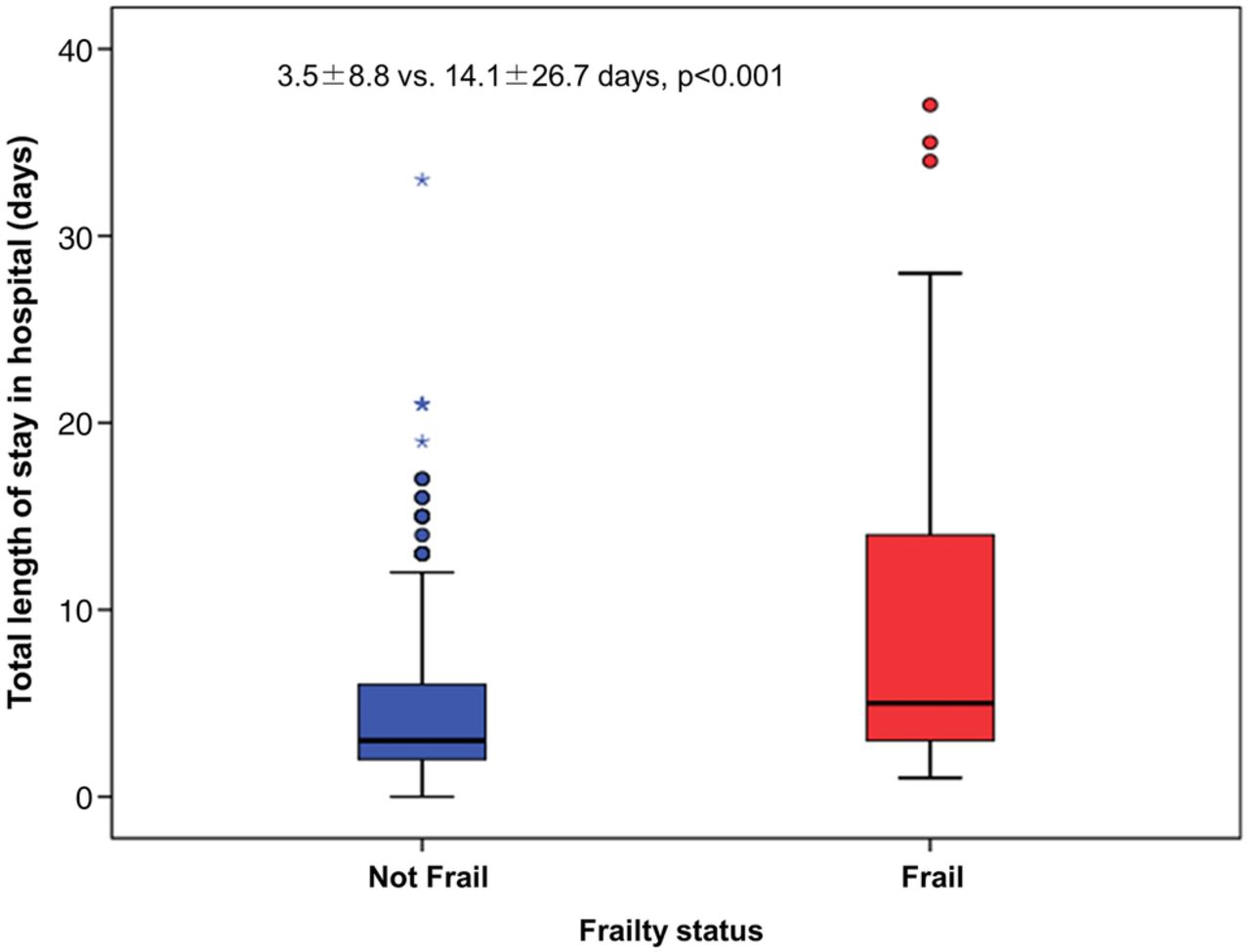
Frailty and length of hospital stay. Frailty was associated with increased length of hospital stay.
Mortality
The 30-day mortality rate after PCI was available for 744 (99.8%) of the patients, and it was 1.5% (n=11) for the entire group. For frail patients 30-day mortality was 4.9% versus 1.1% for non-frail patients. Frail patients were nearly five times more likely to die within 30 days after PCI, compared with non-frail patients (HR 4.8, 95% CI 1.4 to 16.3, p=0.01; figure 3). Patients with higher frailty scores had higher 30-day and 1 year mortality (table 2). Covariates with a significant trend (p<0.1) in the univariate analyses were included in a multivariate model. Frailty, but not age, predicted 30-day mortality. The predictors of mortality from cox-regression analyses are shown in table 3.
Frailty scores and mortality
Predictors of mortality from cox regression analyses

{kind=link}
{kind=link}
{kind=link}
Mortality according to Frailty score. Frailty was associated with higher 30-day (A) and 1-year (B) mortality.
The 1 year mortality rate was 2.7% for the entire cohort; 11.1% for frail patients and 1.9% for non-frail patients. Frailty conferred a sixfold risk of death at 1 year compared with non-frailty (HR 5.9, 95% CI 2.5 to 13.8, p<0.001; figure 3). At multivariate analysis, both age and frailty were independent risk factors for 1 year mortality (table 3).
Discussion
Our study highlights a strong association between frailty and length of hospital stay, 30-day mortality and 1 year mortality after PCI. This association is independent of age and other conventional risk factors and comorbidities.
Risk stratification is important in clinical decision-making and also aids patient counselling and informed consent.20 All PCI risk scores have age as an integral factor.20–22 However, chronological age correlates poorly with biological age;14 about one-third of people above 85 years may be frail, while other two-thirds are not,11 representing the heterogeneity of ageing. Exploration into factors such as frailty, comorbidity, cognitive impairment and disability are required to reorganise care and management of elderly patients with coronary artery disease.4–7 Although there is overlap with comorbidity and disability, frailty is now considered to be a distinct pathophysiological condition.5 ,11 The traditional cardiac risk scores, while they offer good correlation with cardiovascular outcomes, may not help to identify patients who may benefit from an invasive treatment and who should receive conservative medical or palliative care. Novel holistic tools may be required.23 The ‘Gold Standards Framework Prognostic Indicator Guide’ (GSF), originally developed for patients with cancer, has been recently shown to have a good accuracy to stratify risk in patients presenting with ACS.24 ,25 We have shown that frailty is an independent and perhaps more important risk factor than age. NY risk score has age, comorbidities and angiographic data on left main stem disease and may therefore not help to guide which patients should go invasive or conservative therapy. Furthermore, it remains to be seen if replacing age with frailty in the NY score improves its prognostic utility.
The Canadian Study of Health and Aging Clinical Frailty Scale is a simple tool to quickly establish level of frailty and can be used by any healthcare professional with no extra investigations or expertise required to complete the assessment.26 Using this scale, we found that a sizeable proportion of patients undergoing PCI were frail. Several clinical characteristics, including age and comorbidities, were associated with frailty. It is unsurprising that age is strongly associated with frailty as people tend to become frail as they age. Frailty is considered to be a ‘geriatric’ syndrome as a broad generalisation5 ,11 ,27 although the two are not necessarily synonymous. The relationship between frailty and being female is in keeping with previous findings.18 ,27 ,28 This may be due to diseases, such as osteoporosis, that are more common in women than men; or to the later presentation of coronary artery disease in women. Osteoporosis escalates the frailty stereotype particularly in reducing mobility. Cardiovascular risk factors and comorbidities tend to increase with age, which may explain their association with frailty.
Our data indicate that frailty is a risk factor for longer hospital stay and mortality after PCI. Frailty has previously been found to be associated with longer hospital stay29 and also with increased rates of hospitalisation for any cause.30 Greater length of stay implies that the frail patients are in worse health, take longer to recover after PCI and may have more postprocedural complications. This suggests they are at increased risk of adverse outcomes. Greater length of stay also has implications for increased costs of healthcare. Frailty was found to be significantly associated with 30-day and 1 year mortality following PCI, suggesting that it could be considered as short and mid-term prognostic marker. There were no patients with frailty score 8 or 9 undergoing PCI, suggesting that clinicians were managing these patients conservatively. Further studies are needed to find how to best use frailty scores in decision-making for conservative versus invasive management.
Limitations
This study has several limitations. It was not logistically possible to enrol all consecutive patients, especially out of hours, which may have excluded high-risk emergency patients. Furthermore, only patients undergoing PCI were included in this study and it is likely that a proportion of frail patients were not offered interventions based on clinical judgment about futility of invasive approach in these patients. While mortality rates were available for almost all patients, total length of hospital stay was not available for 22.7% patients as many patients were repatriated to their local hospitals after PCI. Finally, the Canadian Study of Health and Aging Clinical Frailty Scale used to assess frailty is subjective in nature and therefore predisposed to interobserver variability. However, this does not appear to reduce the predictive power of this frailty score to predict outcomes.
Conclusion
The Canadian Study of Health and Aging Clinical Frailty Scale can help to predict mortality and the length of hospital stay after PCI. This simple and quick to use assessment tool can provide additional prognostic information, complementing conventional risk scores and guide healthcare providers to plan PCI and appropriate resources for frail patients.
Acknowledgments
The authors are grateful to all the interventional cardiologists at South Yorkshire Cardiothoracic Centre who contributed to this study. The authors would also like to thank Louisa Yates for help in data extraction.
References
Footnotes
RM-K and JI have contributed equally.
Contributors JI, AS and JG conceived the idea. RM-K, RR, EH, YP and AS collected data. JI, RM-K and JR analysed the data. JI drafted the paper and all authors critically reviewed and approved.
Competing interests None declared.
Ethics approval Sheffield Teaching Hospitals NHS Trust.
Provenance and peer review Not commissioned; externally peer reviewed.