Article Text

Abstract
Aims To assess the prognostic importance of high-sensitive C reactive protein (hsCRP) in patients with mild to moderate aortic valve stenosis during placebo or simvastatin/ezetimibe treatment in Simvastatin and Ezetimibe in Aortic Stenosis (SEAS).
Methods and results In 1620 SEAS patients, we measured lipids and hsCRP at baseline and after 1 year of treatment and registered during 4 years of follow-up major cardiovascular events (MCE) composed of ischaemic cardiovascular events (ICE) and aortic valve-related events (AVE). Simvastatin/ezetimibe reduced low-density lipoprotein cholesterol (3.49 (2.94 to 4.15) to 1.32 (1.02 to 1.69) vs 3.46 (2.92 to 4.08) to 3.34 (2.81 to 3.92) mmol/L) and hsCRP (2.1 (0.9 to 4.1) to 1.2 (0.6 to 2.4) vs 2.2 (0.9 to 4.9) to 1.8 (0.85 to 4.35) mg/L, all p<0.05) during the first year of treatment. In multivariable Cox regression analysis adjusting for traditional risk factors and baseline hsCRP, ICE was associated with a 1-year increase of hsCRP (HR=1.19 (95% CI 1.12 to 1.25), p<0.001) but not with active treatment (HRTreatment=0.86 (0.67 to 1.13), p=0.28). Patients in the top quartile of baseline hsCRP versus the rest were associated with a higher risk of MCE (HR=1.34(1.09 to 1.64), p=0.02). The prognostic benefit of reduction in hsCRP after 1 year was significantly larger (p<0.01 for interaction) in patients with high versus low baseline hsCRP; hence, a reduction in hsCRP abolished the difference in incidence of MCE between high versus low baseline hsCRP in patients with reduced hsCRP (31.1 vs 31.9%, NS) in contrast to patients with increased hsCRP.
Conclusions The treatment-associated reduction in ICE was in part related to a reduction in hsCRP but not in lipids. hsCRP reduction was associated with less MCE, especially in patients with high baseline hsCRP.
Trial registration NCT00092677.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Little is known concerning this subject. The present study is, to the best of our knowledge, the first study to test the prognostic importance of in-treatment changes in high-sensitive C reactive protein (hsCRP). In the smaller ASTRONOMER study, hsCRP was measured at year 1 as well, but these data have not been utilised.
What does this study add?
In our study, alterations in hsCRP are a stronger predictor of outcome than baseline hsCRP. We demonstrate that a reduction in hsCRP is associated with an improved prognosis, resembling that of patients with low baseline and low 1-year hsCRP.
In the Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) study, lipid-lowering treatment did not reduce the primary, combined end point, but a 22% reduction in ischaemic events was observed. This reduction in ischaemic events was associated with a reduction in hsCRP, but not in lipids. This is in line with findings from the JUPITER trial, but has not previously been shown in patients with aortic stenosis.
How might this impact on clinical practice?
We believe that better knowledge about the importance of inflammation in patients with aortic stenosis may improve risk stratification, making disease monitoring more individualised and better targeted and preventing morbidity and mortality in patients with aortic stenosis.
Introduction
The role of inflammation in the pathogenesis of aortic valve disease remains unclear. Therefore, we investigated the prognostic importance of baseline high-sensitive C reactive protein (hsCRP) and changes in hsCRP during the first year of lipid lowering with simvastatin 40 mg and ezetimibe 10 mg versus placebo in the Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) study. The SEAS study tested if simvastatin and ezetimibe in combination could reduce the need for aortic valve replacement (AVR). The study was neutral in reducing major cardiovascular events (MCE) consisting of both aortic valve-related events (AVE) and ischaemic cardiovascular events (ICE), but a 22% reduction in ICE in the treatment group was shown.1 This reduction primarily consisted of a reduction in coronary artery bypass grafting (CABG).2
Cholesterol and inflammation are involved in the development of atherosclerosis and subsequent cardiovascular disease.3 ,4 ,4a ,4b ,4c Histology of stenotic aortic valves shows subendothelial plaque-like lesions on the aortic side of the leaflets that resemble those seen in atherosclerosis and ‘atherogenic’ lipoproteins are accumulated in the lesions.5 ,6 hsCRP has shown its potential as a predictor of cardiovascular disease in several studies.7 ,8 ,8a ,8b ,8c Therefore, we hypothesised that a reduction in hsCRP would be associated with fewer ischaemic events, in line with findings from the JUPITER trial,9 and we also wanted to explore if a reduction of hsCRP would be associated with fewer MCE in this aortic stenosis (AS) population.
Methods
Study population
The SEAS study was a multicentre, randomised, double-blind, placebo-controlled study investigating whether intensive lipid lowering with simvastatin/ezetimibe combination versus placebo could reduce the need for AVR and risk of cardiovascular morbidity and mortality in 1873 patients aged 45–85 years with asymptomatic AS (defined as echocardiographic aortic valve thickening accompanied by a Doppler-measured aortic peak flow velocity >2.5 and <4 m/s and normal left ventricular (LV) systolic function). For this substudy, we included 1620 patients with hsCRP analysed at baseline. In total, 253 patients were excluded for missing baseline values of hsCRP. There were no differences between the study population and the 253 excluded patients with regard to age, gender, treatment and tobacco use. The complete study protocol, study design, organisation, clinical measures, exclusion criteria (most importantly, systolic heart failure, diabetes mellitus and known ischaemic heart disease) and baseline characteristics have been published previously.1 ,10 All patients gave written informed consent, and ethics committees in all participating countries approved the study (the SEAS trial is registered at http://ClinicalTrials.gov, identifier NCT00092677).
High-sensitive C reactive protein
hsCRP was measured at baseline and at 1 year after inclusion. Serum hsCRP concentration was determined using a particle-enhanced immunoturbidimetry assay (Roche/Hitachi) range 0.1–20 mg/L and lowest detection limit 0.03 mg/L. A 1 year increase in hsCRP was defined as a rise from baseline to year 1.
White cell count and lipids
White cell counts (WCCs) were measured only at baseline and lipids were measured at baseline, and then every 6 months during follow-up. All blood samples were analysed by the central laboratory, PPD Global Central Labs, in Belgium. Study investigators were blinded to lipid values throughout the entire study.
Hypertension and tobacco
Hypertension was defined in the SEAS study as a history of hypertension or the use of antihypertensive medication.11 This was reported by an attending physician or an elevated blood pressure at the baseline clinical visit (systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg), in accordance with the European Society of Hypertension Guidelines.12 Tobacco status was self-evaluated at study entrance.
ECG
The specifics about protocol, reading and reproducibility have been published previously.13 In short, ECGs were recorded at baseline and then annually at the local study centres, after which they were sent to the central ECG core laboratory at The Heart Center, Rigshospitalet, Denmark. A physician blinded to the randomisation and clinical data read and transferred all ECGs directly to a database by use of the Minnesota codes.13
Echocardiogragraphy
The study protocol has been published earlier.14 In short, echocardiography was performed at baseline, once a year and before valve surgery if needed. Echocardiography was performed according to a standardised echocardiographic protocol. All images were read at the SEAS Echocardiography Core Laboratory at Haukeland University Hospital in Bergen, Norway. All readings were performed according to the American Society of Echocardiography guidelines. The readers were unaware of the sequence and site in order to minimise bias.
Efficacy outcomes
The SEAS study was event driven and was designed to continue until 464 events had occurred or all patients had been followed for at least 4 years. The primary outcome was MCE, a composite consisting of death from cardiovascular causes, AVR, congestive heart failure because of progression of AS, non-fatal myocardial infarction, hospitalisation for unstable angina, CABG, percutaneous coronary intervention (PCI) or non-haemorrhagic stroke. MCE included AVE and ICE. ICE was defined as death from cardiovascular causes, non-fatal myocardial infarction, hospitalisation for unstable angina, CABG, PCI or non-haemorrhagic stroke. All outcomes were classified by an independent End-point Classification Committee unaware of study group assignment.1
Statistical analyses
Baseline characteristics are presented as mean±SD for continuous variables and proportions for categorical variables. Non-Gaussian distributed variables are presented as median values and IQR. hsCRP was log2 transformed in order to fulfil model assumptions in statistical analyses. Log2 was used to evaluate the risk associated with doubling of the concentration. Changes (1 year) in hsCRP are reported as the 1-year value minus baseline hsCRP. Unpaired Student t test was used to determine differences between treatment groups and paired Student t test was used to determine changes during treatment within each treatment group for normally distributed variables. For non-Gaussian distributed variables, Mann-Whitney U test and Wilcoxon signed-rank test, respectively, were used. Differences in continuous and categorical baseline characteristics were analysed using the one-way analysis of variance. Correlation between baseline characteristics of interest was explored using Spearman correlation analysis. For outcome prediction and comparison between groups, Kaplan-Meier plots and the log rank test were used. HRs were assessed by multiple Cox proportional hazard analyses and presented with 95% CI. hsCRP as a variable of interest along with gender, age and treatment allocation were forced into the models. The other variables of interest: blood pressure, body mass index (BMI), heart rate, glucose, WCC, total and low-density lipoprotein (LDL) cholesterol, 1-year changes in total and LDL-cholesterol, estimated glomerular filtration rate, tobacco, aspartate aminotransferase (AST) and ejection fraction were added to the models by backward selection. The performance of the Cox models was summarised using C-statistics to allow for right censoring of data and variable follow-up time.15 The two models compared were the basic model (the best statistical performing model predicting outcome without hsCRP and treatment forced into the model age, sex, heart rate, WCC, tobacco and treatment group) versus the new model (basic model plus baseline hsCRP and 1-year changes in hsCRP). Net reclassification improvement (NRI) was estimated as continuous NRI and presented with its CI and upward and downward reclassification rates.16 The bias-corrected 95% CIs for the C-statistics and NRI were assessed by the usage of bootstrapping. Finally, the integrated discrimination improvement (IDI) was calculated.17 This measure can be described as the difference in improved sensitivity and potential increase in ‘one minus specificity’, with the new model including the marker of interest versus the basic model.17 For all models, a two-tailed p<0.05 was required for statistical significance. Statistical analyses were performed using IBM SPSS V.20.0.0 (SPSS, Chicago, Illinois, USA) and R V.2.15.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
At baseline, the median age was 69 years (IQR 61–75; table 1).
Baseline characteristics according to quartiles of baseline hsCRP
With ascending quartiles of hsCRP, most of the traditional cardiovascular risk factors increased significantly. The proportion of men proportion fell with increasing quartiles of baseline hsCRP. With increasing quartiles of hsCRP, LV mass indexed by body surface area (baseline mean=102 g/m2) and aortic valve peak velocity (baseline mean=3.05 m/s) did not increase, whereas aortic valve area index (baseline mean=0.63 cm2/m2) did decrease significantly (table 1).
At baseline, hsCRP was associated with WCC (r=0.33, p<0.001), but not with total cholesterol (r=−0.041, p=0.10) or LDL-cholesterol (r=0.002, p=0.94). Baseline and 1-year values of lipids, liver marker AST and inflammatory markers are shown in table 2.
Effect of treatment on lipids and markers of inflammation
At 1 year, hsCRP, total and LDL-cholesterol were lower in the treatment group, but unchanged in the placebo group. AST was similar in the two groups at baseline, but increased in the treatment group.
In univariate Cox regression analyses, higher baseline hsCRP as well as an increase in hsCRP predicted MCE as well as ICE (table 3).
Cox regression models predicting major cardiovascular and ischaemic events
In multivariate Cox regression analyses, hsCRP values predicted both MCE and ICE independently of each other as well as the traditional cardiovascular risk factors (table 3). The highest event-free survival was observed in the two groups with reduced hsCRP values (figure 1A).
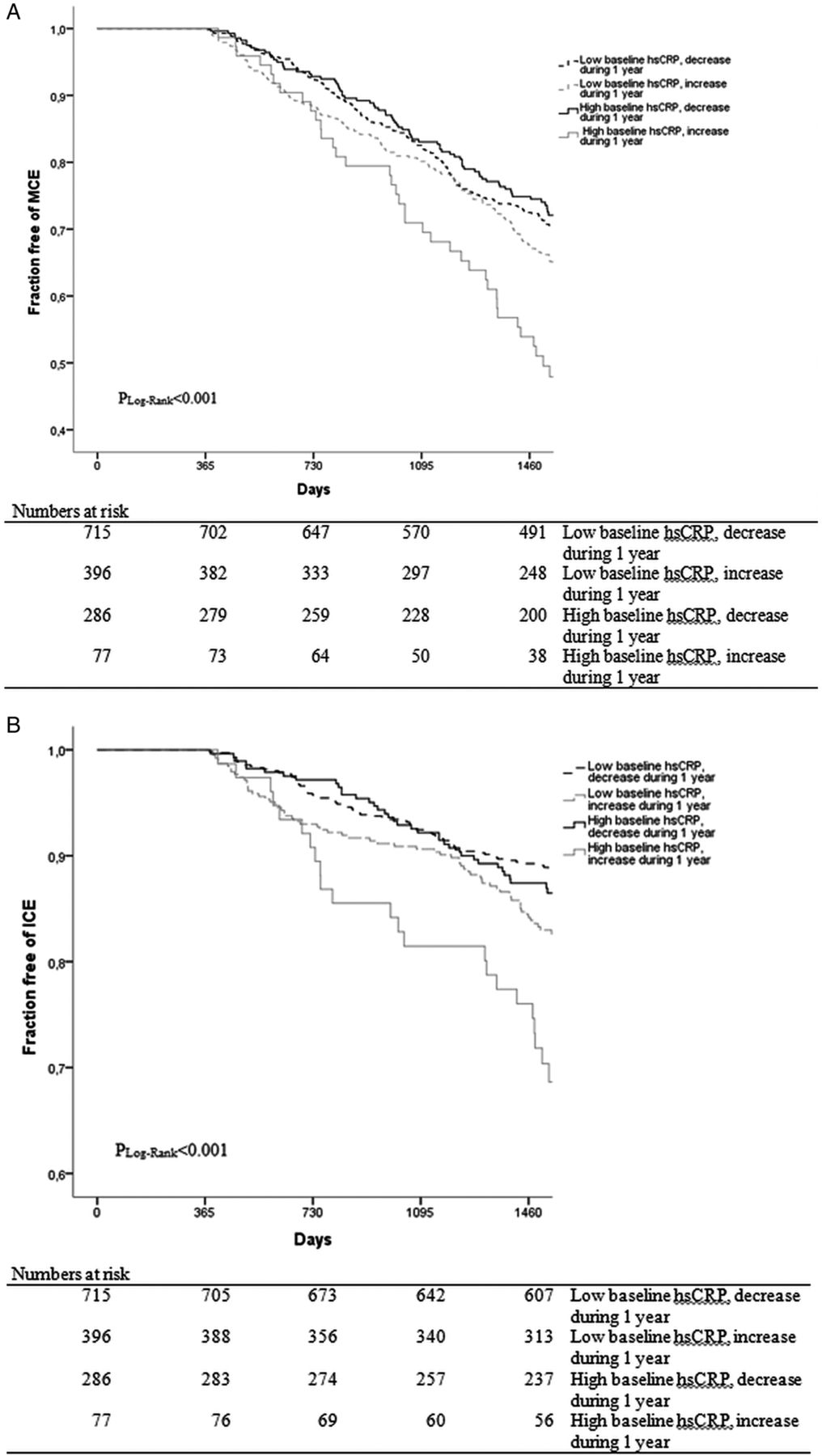
{kind=link}
Event-free survival according to baseline and 1-year changes in high-sensitive C reactive protein (hsCRP). Survival free of (A) major cardiovascular event (MCE) and (B) ischaemic cardiovascular event (ICE) according to baseline and 1-year changes in hsCRP.
More events (MCE) occurred with increasing hsCRP at baseline (p=0.014). However, an interaction was observed indicating that risk was primarily confined to those with increasing hsCRP values, in contrast to those with a decreasing hsCRP (table 4; p<0.01 for interaction).
Major cardiovascular event rates and HRs according to quartiles of baseline hsCRP in the whole cohort as well as in patients with increasing or decreasing hsCRP
Actually, in patients with a decrease in hsCRP during the first year, there was no significant difference in event rates in patients with high versus low baseline hsCRP (31.1% vs 31.9%, NS). However, in patients with an increase in hsCRP, a higher MCE rate was observed (56.8 vs 42.5%, p<0.01; table 4). The same pattern was observed for ICE (table 5 and figure 1B), except that the p value for interaction did not reach significance.
Ischaemic cardiovascular event rates and HRs according to quartiles of baseline hsCRP in the whole cohort as well as in patients with increasing or decreasing hsCRP
The risk for MCE rose significantly between the second and the third hsCRP quartile (HR 1.28, p<0.05) and remained elevated (table 4), while the risk for ICE increased between the first and the second quartile (HR 1.64, p<0.05; table 5).
The addition of hsCRP (baseline and 1-year changes) to the basic model improved C-statistics from 0.57 to 0.60 (p<0.05) (table 6).
Performance of MCE risk models including traditional risk factors with and without hsCRP
The addition of hsCRP (baseline and 1-year changes) to the basic model resulted in an improvement in continuous NRI of 0.24 (95% CI 0.13 to 0.38), continuous NRI for events 0.03 and continuous NRI for non-events 0.20. The IDI was 0.03 (p=0.07). For ICE (table 7), the C-statistics improved from 0.65 to 0.68 (p<0.05), and continuous NRI improved by 0.26 (95% CI 0.02 to 0.39), when adding hsCRP (baseline and 1-year changes) to the basic model. Baseline hsCRP alone did not improve prediction of MCE or ICE significantly.
Performance of ICE risk models including traditional risk factors with and without hsCRP
Discussion
This study has two new observations relevant for the role of inflammation in aortic valve stenosis. First, elevated baseline hsCRP as well as a 1-year increase in hsCRP predicted MCE independently of traditional cardiovascular risk factors because an increase in hsCRP was strongly associated with more MCE in patients with elevated baseline hsCRP. Second, the beneficial effect of simvastatin and ezetemibe on ICE seemed to be related to a reduction in low-grade inflammation rather than a reduction in lipids.
Elevated baseline hsCRP as well as a 1-year increase in hsCRP predicted outcome independently of traditional cardiovascular risk factors
To the best of our knowledge, this is the largest study investigating the prognostic importance of hsCRP in patients with asymptomatic mild to moderate AS to date. In the present study, baseline hsCRP as well as a 1-year increase in hsCRP predicted the combined end point independently of the traditional risk factors. In a study performed by Solberg et al,18 hsCRP predicted cardiovascular events in patients with severe AS significantly in univariate analysis, but not when included in a multivariate analysis. In a small study by Dichtl et al,19 CRP remained significant in multivariate analysis, with an HR of 1.6. The study by Dichtl et al19 resembled the SEAS study with regard to inclusion criteria and baseline characteristics, while the population in the study by Solberg et al18 had more advanced disease, an incidence of coronary artery disease of 50% and all were referred for AVR. However, in the ASTRONOMER trial, the only other study with in-treatment CRP values, although not to the best of our knowledge reported, CRP did not predict outcome and there was no difference in survival according to baseline CRP.20 The baseline characteristics in ASTRONOMER were different from those in SEAS.21 In total, 48.9% had congenital bicuspid aortic valves, they were younger and only fewer were currently smoking at inclusion. Our findings complement these studies. In a previous report from the SEAS study22 evaluating hsCRP as part of developing a risk score for predicting mortality in patients with asymptomatic mild to moderate AS, hsCRP also significantly predicted mortality.
Furthermore, reduction in hsCRP during the first study year was associated with better outcome independently of baseline hsCRP and traditional cardiovascular risk factors. This is the first time that an association between treatment-induced changes in an inflammatory marker and MCE has been demonstrated in a population of patients with AS. The beneficial effect of a decrease in hsCRP during the first year of treatment was largest for those with a baseline hsCRP in the top quartile. Interestingly, the beneficial effect of a decrease in hsCRP seemed to obliterate the prognostic importance of baseline hsCRP (tables 4 and 5). These observations have also been reported in other populations, that is, in the general population,23 in patients with chronic heart failure,24 and in patients with non-ST elevation acute coronary syndrome.25
Furthermore, we found that hsCRP added significantly to the model predicting MCE assessed by C-index and continuous NRI. This suggests that low-grade inflammation assessed by hsCRP might be an important marker of progression of AS. However, our results need confirmation in other studies before hsCRP can be used clinically for estimation of cardiovascular risk in participants with AS.
The beneficial effect of simvastatin and ezetimibe on ICE was partly due to reduced hsCRP
Not surprisingly, baseline hsCRP as a marker of low-grade inflammation significantly predicted ICE as previously demonstrated in many other cohorts.7 ,26 ,27 When 1-year changes in hsCRP were added to the model, treatment allocation was no longer significant in the prediction of ICE. As expected, simvastatin and ezetimibe treatment reduced the lipid levels, but in Cox regression analysis changes in neither total nor LDL-cholesterol were significantly associated with ICE. Therefore, our study indicates that the reduction in ICE was related to the reduction in inflammation and not to changes in lipids. This corresponds well with previous findings from the JUPITER trial.9 However, neither studies were able to show conclusively whether it was the lipid reduction, reduced inflammation or a combination of the two, which accounted for the beneficial effect on ICE. Therefore, further studies are needed to answer this question. A possible confounder could be the inflammatory effects of LDL-cholesterol itself and its contribution to increased hsCRP.
Limitations
The inclusion and exclusion criteria for the SEAS study induce some limitations on this study. As this is a non-prespecified explorative substudy no causual relationship can be established. Additionally preconsisting inflammatory diseases or conditions were not considered in planning the original study design. The participants had to be asymptomatic, as well as jet velocity between 2.5 and 4 m/s. In addition, participants with known ischaemic heart disease and diabetes were excluded due to the placebo comparison of the study. However, the study population was otherwise not at low cardiovascular risk due to the relative high age, hyperlipidaemia, obesity, smoking and high prevalence of hypertension10 and did reflect patients seen in the daily clinic. As the findings were generated from post hoc analysis, any causal relationship cannot be inferred from these results.
Conclusion
Although treatment with simvastatin 40 mg and ezetimibe 10 mg reduced both cholesterol and hsCRP, the treatment-associated reduction in ICE seemed to be related to the reduction in hsCRP rather than in cholesterol. hsCRP reduction was associated with fewer MCE and the prognostic benefit of a 1-year reduction in hsCRP was larger in patients with high baseline hsCRP.
References
Footnotes
Contributors AB wrote the manuscript; CA, OWN, TS, KW and MHO took part in the concept and design of the substudy. YAK, CG-B, KB, RW, SR, CAN and AR were active participants in the interpretation and critical revision of the data; in addition to designing the SEAS main study. All authors have read and approved the final manuscript.
Funding The SEAS study was conducted with financial support from Merck & Co, Inc, Whitehouse Station, New Jersey, USA. This SEAS study was supported by a scientific grant from the Interreg IVA program, a European Union regional fund.
Competing interests CG-B, KB, SR, CAN and KW were investigators and members of the steering committees of the SEAS study and have received honoraria from Merck & Co, Inc, the sponsor of the SEAS study. KB, SR and KW have received grant support from Merck & Co, Inc, the sponsor of the SEAS study. AK reported Speaker's fee from Abbott, MSD and Novo Nordisk, Consult for MSD. Research funding from MSD. Ownership of Orion Pharma stock.
Provenance and peer review Not commissioned; externally peer reviewed.