Article Text

Abstract
Cardiovascular disease is the leading cause of premature mortality in the developed world, and hypertension is its most important risk factor. Controlling hypertension is a major focus of public health initiatives, and dietary approaches have historically focused on sodium. While the potential benefits of sodium-reduction strategies are debatable, one fact about which there is little debate is that the predominant sources of sodium in the diet are industrially processed foods. Processed foods also happen to be generally high in added sugars, the consumption of which might be more strongly and directly associated with hypertension and cardiometabolic risk. Evidence from epidemiological studies and experimental trials in animals and humans suggests that added sugars, particularly fructose, may increase blood pressure and blood pressure variability, increase heart rate and myocardial oxygen demand, and contribute to inflammation, insulin resistance and broader metabolic dysfunction. Thus, while there is no argument that recommendations to reduce consumption of processed foods are highly appropriate and advisable, the arguments in this review are that the benefits of such recommendations might have less to do with sodium—minimally related to blood pressure and perhaps even inversely related to cardiovascular risk—and more to do with highly-refined carbohydrates. It is time for guideline committees to shift focus away from salt and focus greater attention to the likely more-consequential food additive: sugar. A reduction in the intake of added sugars, particularly fructose, and specifically in the quantities and context of industrially-manufactured consumables, would help not only curb hypertension rates, but might also help address broader problems related to cardiometabolic disease.
- sugar
- fructose
- sucrose
- glucose
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known on this subject?
-
Cardiovascular disease is the leading cause of premature mortality in the developed world, and hypertension is its most important risk factor.
-
Controlling hypertension is a major focus of public health initiatives, and dietary approaches have historically focused on sodium.
What might this study add?
-
The predominant sources of sodium in the diet, processed foods, are also generally high in added sugars, the consumption of which might be more strongly and directly associated with hypertension and cardiometabolic risk.
How might this impact on clinical practice?
-
Clinicians should shift focus away from salt and focus greater attention to the likely more-consequential food additive: sugar.
-
A reduction in the intake of added sugars, particularly fructose, and specifically in the quantities and context of industrially-manufactured consumables, would help not only curb hypertension rates, but might also help address broader problems related to cardiometabolic disease.
Introduction
Cardiovascular disease (CVD) is the number one cause of premature mortality in the developed world,1–3 and hypertension is its most important risk factor.4 Hypertension was implicated as a primary or contributing factor in more than 348 000 deaths in the USA in 20095 with costs to the nation in excess of $50 billion annually.6 Controlling hypertension is a major focus of public health initiatives, and dietary approaches to address hypertension have historically focused on sodium. Nonetheless, the potential benefits of sodium reduction are debatable.7–9 Reducing sodium intake may lower blood pressure measurements in some individuals, but average blood-pressure reductions might only be as great as 4.8 mm Hg systolic and 2.5 mm Hg diastolic—being generous (only considering upper confidence limits and only considering persons with hypertension)10—and whether there would be a net health benefit from such reductions is unclear. In fact, there is some evidence suggesting that reducing sodium intake could lead to worse health outcomes, such as increased cardiovascular and all-cause mortality in patients with diabetes,11 and increased hospitalisations and mortality in patients with congestive heart failure.12–15 More importantly, recent data encompassing over 100 000 patients indicates that sodium intake between 3 and 6 g/day is associated with a lower risk of death and cardiovascular events compared to either a higher or lower level of intake.16 ,17 Thus, guidelines advising restriction of sodium intake below 3 g/day may cause harm.
Strategies to lower dietary sodium intake focus (implicitly if not explicitly) on reducing consumption of processed foods: the predominant sources of sodium in the diet.18 For instance, the Food and Drug Administration has recently announced that it is drafting guidelines asking the food industry to voluntarily lower sodium levels.19
Nonetheless, the mean intake of sodium in Western populations is approximately 3.5–4 g/day.20 Five decades worth of data indicates that sodium intake has not changed from this level across diverse populations and eating habits, despite population-wide sodium-reduction efforts and changes in the food supply.21 ,22 Such stability in intake suggests tight physiologic control, which if indeed the case, could mean that lowering sodium levels in the food supply could have unintended consequences. Because processed foods are the principal source of dietary sodium,18 if these foods became less salty, there could be a compensatory increase in their consumption to obtain the sodium that physiology demands.
Coincidentally, processed foods happen to be major sources of not just sodium but of highly refined carbohydrates: that is, various sugars, and the simple starches that give rise to them through digestion. Compelling evidence from basic science, population studies, and clinical trials implicates sugars, and particularly the monosaccharide fructose, as playing a major role in the development of hypertension. Moreover, evidence suggests that sugars in general, and fructose in particular, may contribute to overall cardiovascular risk through a variety of mechanisms. Lowering sodium levels in processed foods could lead to an increased consumption of starches and sugars and thereby increase in hypertension and overall cardiometabolic disease (figure 1).
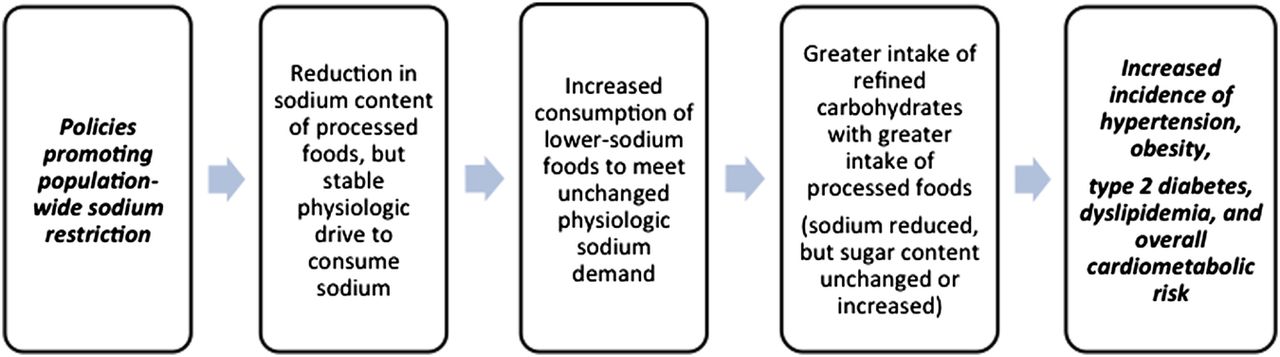
Unintended consequences of population-wide sodium restriction.23
Basic-Science: sucrose, fructose, hypertension and cardiovascular risk
Sucrose, or table sugar, is a disaccharide composed of two monosaccharides: glucose and fructose. Sucrose is a common ingredient in industrially processed foods, but not as common as another sweetener: high-fructose corn syrup (HFCS). Whereas sucrose is equal parts fructose and glucose, HFCS has more fructose (usually 55%) than glucose (the remaining 45%) and is the most frequently used sweetener in processed foods, particularly in fruit drinks and sodas.24
Feeding sucrose to rats stimulates the sympathetic nervous system (SNS),25 which leads to increases in heart rate,26 renin secretion, renal sodium retention and vascular resistance.27 All of these effects interact to elevate blood pressure and, indeed, feeding sucrose to rats increases their blood pressure.28–33 Sucrose feeding also induces other changes, like insulin resistance, as part of a broader metabolic dysfunction.28–33 Additionally, the consumption of sugar or HFCS may lead to an increase in blood pressure via other mechanisms, such as hyperleptinaemia, an increase in methylglyoxal, and a reduction in ATP (figure 2).23 Figure 2 describes the possible mechanisms through which fructose may contribute to hypertension.

{kind=link}
{kind=link}
Straight fructose induces similar results as sucrose when ingested—both in rodents28 ,34 ,35 and humans.36–42 Although high intakes of either fructose alone or sucrose may lead to insulin resistance,43–46 it is fructose that has been implicated as the sugar responsible for reducing sensitivity of adipose tissue to insulin.47 Insulin stimulates the SNS26 ,48–50 and hyperinsulinaemia may lead to hypertension, with the degree of insulin resistance in peripheral tissues directly correlated with hypertension severity.51 ,52 Reducing insulin resistance may lead to a reduction in blood pressure,48 and hyperinsulinaemia seems more related to fructose than glucose.53
Population studies: fructose and other sugars and cardiometabolic health
Insulin resistance is seen in approximately 25% of the general population and up to 80% of individuals with ‘essential’ hypertension.54 Compared to non-diabetics, diabetics have a higher prevalence of hypertension.55 ,56 This disproportion is independent of weight, suggesting that insulin resistance, not obesity per se, increases the risk of hypertension. Indeed, approximately 50% of hypertensive patients have hyperinsulinaemia compared to only 10% of normotensive patients.57 Additionally, hypertensive patients have decreased insulin sensitivity, increased basal insulin and a decreased rate of glucose disposal after an intravenous glucose tolerance test when compared to normotensives, even after adjustment for other risk factors.58 A diet high in sugar has been found to cause deterioration of glucose tolerance,59 and positive correlations exist between sugar consumed 20 years earlier and diabetes.60
A recent econometric analysis showed that an increase in sugar availability is directly and independently associated with an increase in diabetes prevalence.61 In fact, a 150-kilocalorie/person/day increase in sugar availability was found to be significantly associated with a rise in diabetes prevalence (1.1%, p<0.001). This risk was 11-fold higher compared to 150-kilocalorie/person/day increase in total calorie availability, supporting the notion that sugar may be distinct among calories in its potential detriment to metabolic health.
Compared to patients who consume less than 10% of their calories from added sugars, those who consumed 10.0–24.9% of their calories from added sugars have a 30% increased risk of mortality from CVD.62 Those who consume 25% or more calories from added sugars have an almost threefold increased risk.62 Data from the National Health and Nutrition Examination Survey (NHANES 2003 to 2006) indicates a mean fructose intake of 83.1 g/day.63 Concerning, is that an intake >74 g/day of fructose is independently associated with 26%, 30% and 77% higher risks for blood pressures >135/85 mm Hg, 140/90 and 160/100, respectively.36 Consuming sugar-sweetened beverages has been directly associated with increased blood pressure in a study of almost 2700 people from 10 USA/UK populations, independent of body weight and height.64
In a systematic review of 12 studies (cross-sectional and prospective cohort) encompassing over 400 000 participants, sugar-sweetened beverage intake was significantly associated with higher blood pressure and an increased incidence of hypertension.65 The authors concluded that, “intake of >12 fL. oz. of sugar-sweetened beverage per day can increase the risk of having hypertension by at least 6%, and it can increase mean systolic blood pressure by a minimum of 1.8 mm Hg in roughly over 18 months.” Such beverages may contain substantially more fructose than once thought,66 ,67 and consumption of SSBs has been shown to increase the risk of not just hypertension, but of coronary heart disease, stroke and other cardiometabolic disease including obesity and diabetes.68–74 Worldwide, SSB consumption has been implicated in 180 000 deaths/year.75
Clinical trials: modifying sugar intake and CVD-related outcomes
Some individuals show a rise in blood pressure after just a few weeks on a high-sucrose diet (defined as 33% of total caloric intake from sucrose).76 In fact, a meta-analysis of randomised controlled trials showed that higher sugar intake significantly increases systolic (6.9 mm Hg, p<0.0001) and diastolic blood pressure (5.6 mm Hg, p=0.0005) versus lower sugar intake in trials of 8 weeks or more in duration.77 Moreover, when studies that received funding from the sugar industry were excluded from the analysis, the magnitude of blood pressure elevation was even more pronounced (7.6 mm Hg systolic, 6.1 mm Hg diastolic on average). Higher sugar intake also significantly increased triglycerides, total cholesterol and low-density lipoprotein, independent of effects on body weight and when matched for calories (suggesting that sugars may promote dyslipidemia through mechanisms unrelated to any additional calories they supply).77 Nonetheless, trial data show that patients consuming 28% of their energy from sucrose (approximately 152 g of sucrose per day, mainly from beverages) for just 10 weeks have a significant increase in body weight (1.6 kg), as well as increases in fat mass (1.3 kg) in addition to increases in blood pressure (3.8 mm Hg systolic, 4.1 mm Hg diastolic).78
As for different effects from different sugars (eg, sucrose (fructose+glucose) vs fructose alone in particular), one study examined blood pressure responses to various sugar solutions in 20 healthy normotensive men.79 Ingestion of the sucrose solution significantly increased systolic blood pressure by 9 mm Hg. The increase in systolic blood pressure resulting from the fructose-only solution (4 mm Hg) was not statistically significant, however the lower response may have been due to poorer absorption of fructose unaccompanied by glucose.80 Nonetheless, fructose had the greatest antinatriuretic effect,80 suggesting a minimal role of sodium retention as a mechanism for blood-pressure response to added sugar intake. Another trial showed a more pronounced hypertensive response to drinking a HFCS (fructose+glucose)-sweetened beverage versus a sucrose-sweetened beverage in healthy individuals (15/9 mm Hg vs 12/9 mm Hg) and both drinks increased heart rate by 9 bpm.81
Other trials have suggested that fructose may be uniquely detrimental to the cardiovascular system. In a randomised cross-over study in young healthy adults (21–33 years old), ingestion of a fructose solution (60 g) increased systolic blood pressure (6.2±0.8 mm Hg).82 A similar increase in blood pressure was not seen with ingestion of a glucose solution but both drinks significantly increased heart rate and cardiac output.82 The authors concluded that fructose, but not glucose, may cause elevations in blood pressure by increasing cardiac output without a compensatory peripheral vasodilation; whereas both glucose and fructose increase blood pressure variability and myocardial oxygen demand. The marked increase in systolic blood pressure and blood pressure variability with fructose is concerning, as these are independent risk factors for macrovascular and microvascular complications in type 2 diabetics.83 Additionally, blood pressure variability is associated with an increased risk of stroke84 and the development of hypertension and target organ damage, even without changes in average blood pressure.85
Fructose may cause other cardiometabolic harm as well. In a randomised trial of 74 adult men, a high-fructose diet for just 2 weeks not only significantly increased 24 h ambulatory blood pressure (+7/5 mm Hg, p<0.004 and p=0.007, respectively) and increased pulse rate by 8% (4 bpm), but also increased triglycerides, fasting insulin and homeostatic model assessment index (a measure of insulin resistance and β-cell function).86 Additionally, fructose lowered levels of high-density lipoprotein and doubled the prevalence of metabolic syndrome, with 25–33% of patients developing the condition.86 Lowering fructose intake (from 59 to 12 g/day) has been shown to lower blood pressure, fasting insulin levels and inflammation in patients with chronic kidney disease.87
A critical dietary caveat
Importantly, it is likely only ‘added’ fructose and other sugars (eg, as found in processed foods and sugary beverages) that may be a problem. Naturally occurring sugars, including fructose, seem to be benign in their usual biological context (ie, in the context of accompanying water, fibre, and other carbohydrates, or even fats and proteins as in many whole plant foods). In fact, in one trial, switching from a Western diet, to a diet containing approximately 20 servings of whole fruit significantly decreased systolic blood pressure, despite a fructose intake of approximately 200 g.88 Moreover, a study randomising 131 patients to two low ‘added-fructose’ diets (a low-fructose diet of <20 g/day, and a moderate-fructose diet of 50–70 g/day including natural sources like fruits) showed comparable improvements from baseline in blood pressure, lipids, serum glucose, insulin resistance, uric acid, soluble intercellular adhesion molecule-1 (ICAM-1) and quality of life score.89
Current levels of sugar consumption and dietary guidelines
Approximately 300 years ago humans were only consuming a few pounds of sugar per year.90 More recent estimates suggest intakes in the US population anywhere from 77 to 152 lbs of sugar per year,91 ,92 with 13% consuming at least 25% of their total caloric intake as added sugars.63 This level of consumption equates to an approximate average intake of added sugars of 24–47 teaspoons (about 100–200 g) per day, with an average daily fructose consumption of 83.1 g.63 Table 1 suggests how such large intake may be possible, showing some representative foods and the sugar loads associated with their consumption.93 In a study of over 1000 American adolescents (aged 14–18) the average daily intake of added sugars was 389 g for boys and 276 g for girls, or up to 52% of total caloric intake.90 The level of added fructose intake implied by these numbers (at least 138 daily grams) is shocking, especially considering there is no physiological requirement for added sugar, particularly fructose, in the diet so potential harms of ingestion clearly outweigh any potential benefits.94
Amount of sugar in common food items93
The American Heart Association (AHA) makes no specific recommendations about fructose, but recommends no more than six teaspoons of sugar per day for women, and no more than nine teaspoons of sugar per day for men.95 The WHO likewise makes no specific recommendations about fructose, but recommends that added sugars should make up no more than 10% of our entire daily caloric intake, with a proposal to lower that level even further (to 5% or less) for optimal health.96 By teaspoons, the WHO advises no more than 6–12 teaspoons per day (based on a 2000 calorie per day diet). Even at the higher end, this is only slightly more than the amount of sugar in a single 12 oz. can of Coca-Cola (around 40 g of sugar/10 teaspoonful). Concerning, is that an entire 1 L bottle of Coca-Cola (at 400 calories) might be okay to drink by more liberal Institute of Medicine (IOM) recommendations, which allow an intake of added sugars up to 25% of total daily calories.97 Such allowance is a problem. Added sugar at this level may increase the risk of death due to CVD by almost threefold.62
Other dietary guidelines focus not on sugar, but salt. For instance, the 2013 AHA/American College of Cardiology (ACC) Guidelines on Lifestyle Management to Reduce Cardiovascular Risk recommend lowering sodium intake to 2400 mg/day with further reduction to 1500 mg/day in order to promote optimal reductions in blood pressure.98 Such dietary restrictions may not result in benefit, may produce harm, and may distract focus from other white crystals of greater concern.99 Sugar may be much more meaningfully related to blood pressure than sodium, as suggested by a greater magnitude of effect with dietary manipulation.10 ,77 There is no mention in the AHA/ACC guideline of reducing intake of added sugars to a specific level, and this deficiency is concerning. Still, as the most substantial dietary sources of sodium are also often the most substantial dietary sources of added sugars (ie, processed foods), advice to limit sodium consumption could coincidentally result in less sugar consumption as well. Hence even potentially misdirected dietary guidelines could serendipitously result in benefit.
Conclusion
High-sugar diets may contribute substantially to cardiometabolic disease. While naturally occurring sugars in the form of whole foods like fruit are of no concern, epidemiological and experimental evidence suggest that added sugars (particularly those engineered to be high in fructose) are a problem and should be targeted more explicitly in dietary guidelines to support cardiometabolic and general health.
Added sugars probably matter more than dietary sodium for hypertension, and fructose in particular may uniquely increase cardiovascular risk by inciting metabolic dysfunction and increasing blood pressure variability, myocardial oxygen demand, heart rate, and inflammation. Just as most dietary sodium does not come from the salt shaker, most dietary sugar does not come from the sugar bowl; reducing consumption of added sugars by limiting processed foods containing them, made by corporations would be a good place to start. Indeed, reducing processed-food consumption would be consistent with existing guidelines already in place that misguidedly focus more on the less-consequential white crystals (salt).
Future dietary guidelines should advocate substituting highly refined processed foods (ie, those coming from industrial manufacturing plants) for natural whole foods (ie, those coming from living botanical plants) and be more explicitly restrictive in their allowances for added sugars. The evidence is clear that even moderate doses of added sugar for short durations may cause substantial harm. Box 1 provides important take-aways.
Important take-aways
-
Sugar may be more meaningfully related to blood pressure than sodium, as suggested by the greater magnitude of effect with dietary manipulation.10 ,77
-
Reducing the amount of sodium in processed foods may lead to an increase in their consumption causing a greater prevalence of cardiometabolic disease (figure 1).23
-
Higher sugar intake significantly increases systolic (6.9mm Hg) and diastolic blood pressure (5.6 mm Hg) in trials of 8 weeks or more in duration.77 This effect is increased to 7.6/6.1 mm Hg, when studies that received funding from the sugar industry are excluded.
-
Ingesting one 24 ounce soft drink has been shown to cause an average maximum increase in blood pressure of 15/9 mm Hg and heart rate of 9 bpm.81
-
Those who consume 25% or more calories from added sugar have an almost threefold increased risk of death due to cardiovascular disease.62
-
Fructose has been shown to stimulate sympathetic tone directly,26 and indirectly by inciting insulin resistance and hyperinsulinaemia.27 ,45 ,46
-
An increase in sympathetic tone from the overconsumption of fructose is one likely mechanism for the sugar's ability to increase heart rate, cardiac output, renal sodium retention, and vascular resistance, all of which may interact to elevate blood pressure and increase myocardial oxygen demand.27 ,80 ,82
-
A high-fructose diet for just 2 weeks not only significantly increased 24 h ambulatory blood pressure (+7/5 mm Hg, p<0.004 and p=0.007, respectively) and increased pulse rate by 8% (4 bpm), but also increased triglycerides, fasting insulin, and homeostatic model assessment (HOMA) index (a measure of insulin resistance and β-cell function).86 Excess fructose intake has also been shown to double the prevalence of the metabolic syndrome.86
-
Current US per capita intake of added sugars is approximately 2–8 times higher than current recommendations by the American Heart Association (AHA) and WHO.91 ,92 Considering adolescents specifically, current consumption might be as much as 6–16 times higher.90
-
Ingestion of sugars, including fructose, in their naturally occurring biological contexts (eg, as whole fruits) is not harmful and is likely beneficial.88 ,89
References
Supplementary materials
Press release
Files in this Data Supplement:
Footnotes
-
Contributors JJD conducted the literature review, conceived the paper, and drafted the main arguments. SCL helped revise and reorganise the arguments, modified the framing, and recast the introduction and discussion. JJD and SCL cowrote the final paper.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.