Article Text

Abstract
Background Intravenous adenosine is used to minimise the coronary micro-resistance to achieve maximal hyperaemia along with nitrates for optimal fractional flow reserve (FFR) measurements. We hypothesise that caffeine, being a competitive inhibitor of adenosine, would influence adenosine-mediated FFR readings.
Methods Consecutive patients undergoing angiogram and FFR measurements were enrolled after abstaining from caffeine for 24 h. Patients with any contraindications to intravenous adenosine or caffeine were excluded. FFR measurements were taken using nitrates and adenosine pre and post 4 mg/kg intravenous caffeine administration and results were compared.
Results 10 patients were analysed (80% men, age 59.9±9.4, weight 87.5±15.6). Baseline caffeine levels were undetectable in all patients and increased significantly postintravenous caffeine administration (16.4±5.5 μg/mL). Baseline preadenosine FFR values were similar before and after caffeine administration (0.91±0.06 vs 0.91±0.07; p=0.41). Postadenosine FFR readings were 0.79±0.07, which increased non-significantly to 0.82±0.11 postcaffeine (p=0.15). Two significant FFR readings (≤0.8) changed to non-significant after caffeine administration (0.77–0.93 and 0.8–0.91).
Conclusions Caffeine may affect FFR results in some patients. Larger studies are warranted to clarify the extent and magnitude of caffeine/adenosine interaction particularly due to ubiquitous nature of caffeine and increasing importance of FFR in clinical practice.
- CORONARY ARTERY DISEASE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
-
Caffeine is a competitive inhibitor of adenosine and can potentially impact on the fractional flow reserve (FFR) results. Patients undergoing adenosine perfusion scintigraphy studies are required to abstain from caffeine for at least 12 hours prior to the test. However, no such guidelines exist for FFR measurements.
What does this study add?
-
Based on our findings it may be hypothesized that sensitivity of caffeine and its inhibitory effect on adenosine can vary between the individuals and has potential to alter the FFR results. Further trials are required to confirm these findings.
How might this impact on clinical practice?
-
A caffeine history may be considered in people undergoing FFR measurements, particularly in context of an unexpected FFR result.
Introduction
Fractional flow reserve (FFR)-guided percutaneous intervention (PCI) improves outcomes in patients with stable and unstable angina.1 ,2 Maximal hyperaemia is paramount for optimal FFR measurements. Intravenous adenosine is the most widely used agent to minimise the coronary micro-resistance and thus induce maximal hyperaemia along with intracoronary nitroglycerine.3
Caffeine is a methylxanthine commonly found in tea, coffee and chocolate. Caffeine is a competitive inhibitor of adenosine A2a receptor at the cellular level.4 Patients undergoing adenosine perfusion scintigraphy studies are required to abstain from caffeine for at least 12 h prior to the test.5 However, no such guidelines exist for FFR measurements. We hypothesise that caffeine, being a competitive inhibitor of adenosine, would influence adenosine-mediated FFR readings.
Methods
Study population
Consecutive patients undergoing standard of care angiogram and FFR measurements to investigate intermediate coronary artery lesion were recruited to participate. Patients with any contraindications to intravenous adenosine or caffeine were excluded, as well as patients with normal or near normal FFR (>0.9; figure 1). Participants were required to abstain from caffeine (tea, coffee and chocolate) for 24 h prior to FFR measurements.
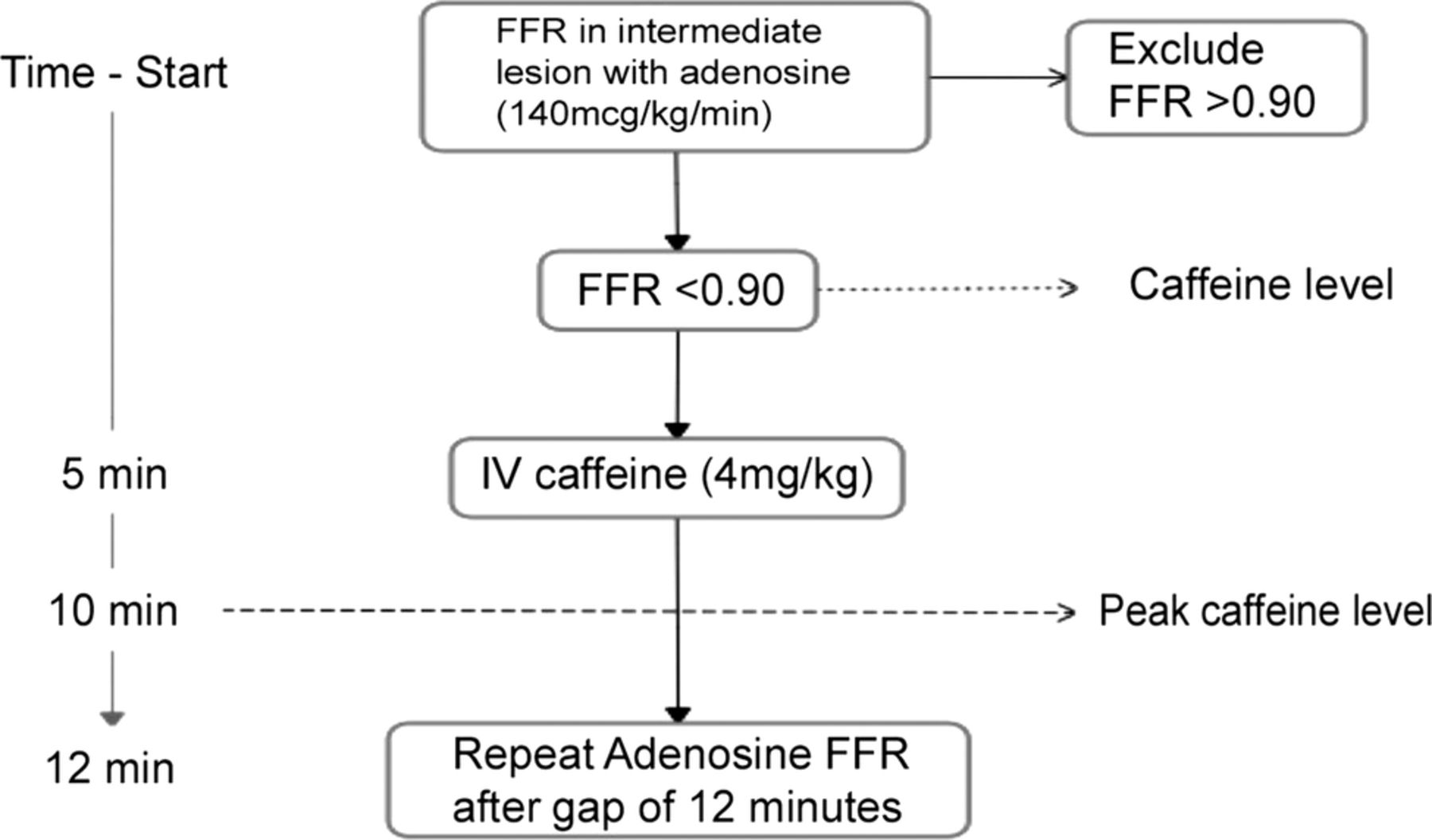
Protocol (IV, intravenous; FFR, fractional flow reserve).
Angiography and baseline FFR
Angiography was performed via right radial or right femoral approach. After guide catheter placement, intracoronary nitroglycerine (200 μg) was administered and repeat angiographic images were obtained to confirm lesion severity. FFR was measured using a 0.014-inch pressure guidewire (St Jude Medical, Minneapolis, Minnesota, USA) after a 3 min peripheral intravenous infusion of adenosine (140 μg/kg/min). The lowest FFR reading over 3 min of adenosine infusion was recorded. All FFR tracings were analysed to ensure absence of artefacts.
Intravenous caffeine and repeat FFR measurements
A period of 3 min was prescribed to allow postadenosine FFR to return to baseline levels. Intravenous caffeine, roughly equivalent of 3–4 cups of average coffee (4 mg/kg),6 was injected over 1 min after obtaining blood samples for baseline caffeine level. Peak caffeine level blood samples were collected after 5 min. A repeat FFR measurement was then performed utilising the same protocol within 12–15 min of initial FFR measurement (figure 1).
Statistical analysis
All data were analysed using SPSS Statistics Software (IBM, Windows, V.19). Data are presented as values and percentages or mean value±SD. Paired t test was used to compare continuous data. A two-tailed p value of <0.05 was considered statistically significant.
Ethical consideration
Therapeutic Goods Administration (TGA, Australia) exemption was sought and obtained to use intravenous caffeine for non-approved trial indication. Informed written consent was obtained from all patients.
Results
Two patients were excluded as their baseline adenosine FFR was >0.9. A total of 10 patients were enrolled. Baseline characteristics of these patients are described in table 1. Mean coffee consumption was 2.85±1.02 cups a day. Individual FFR results are summarised in the table 2. Baseline caffeine levels were undetectable (<5 μg/mL) in all patients and increased significantly postintravenous caffeine administration (16.4±5.5 μg/mL). Mean caffeine dosage administered was 348±41.3 mg. All patients reported flushing symptoms with initial adenosine infusion which were markedly less with repeat adenosine infusion postintravenous caffeine on subjective assessment.
Baseline characteristics
Individual results
Baseline preadenosine FFR values were similar before and after caffeine administration (0.91±0.06 vs 0.91±0.07; p=0.41). Postadenosine FFR readings were 0.79±0.07, which non-significantly increased to 0.82±0.11 postcaffeine (p=0.15). Interestingly, significant FFR values (≤0.8)2 for two patients changed to non-significant after caffeine administration (0.77–0.93 and 0.8–0.91; figure 2). Graphical representation of individual results before and after caffeine is shown in figure 3. There was no relation noted between average baseline coffee consumption (2.85±1.02 cups) and affect to intravenous caffeine on FFR.
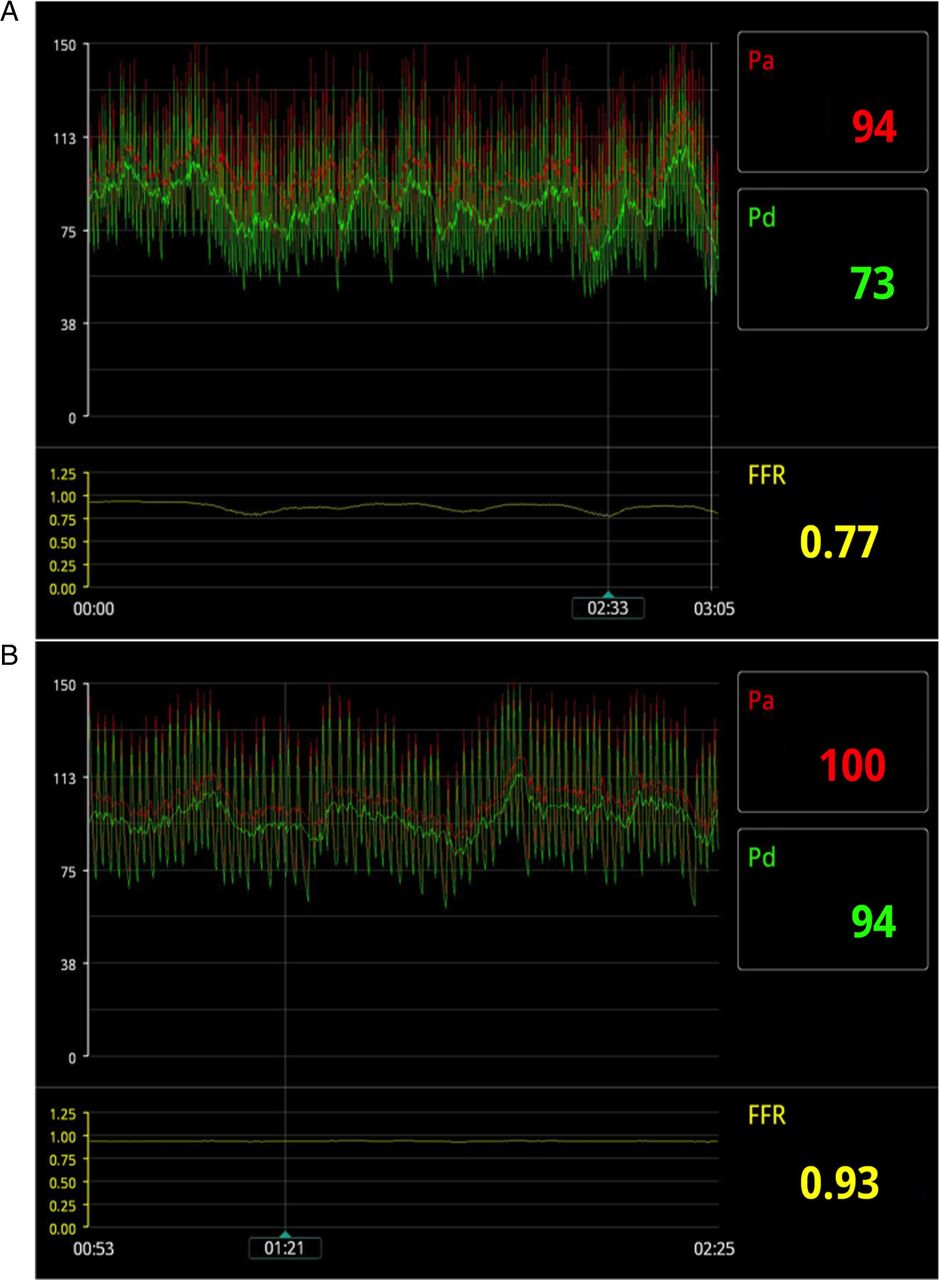
Adenosine fractional flow reserve (FFR) tracings of a patient reading 0.77 before caffeine (A) which changed to insignificant value of 0.93 after caffeine (B).

{kind=link}
{kind=link}
{kind=link}
Graphical representation of individual fractional flow reserve (FFR) results before and after caffeine.
Discussion
Our study demonstrates higher average FFR readings after caffeine administration in 7 (70%) patients using intravenous adenosine when compared with baseline readings. Although this difference did not reach statistical significance over all, it potentially can be clinically relevant in selected individuals, as two patients’ results changed from positive2 (≤0.8) to negative (>0.8). Baseline (preadenosine) readings for both FFR measurements remained unchanged suggestive of caffeine being the causative factor for the change. FFR readings of two patients were decreased after caffeine, the reason of which is unclear. These two patients had significantly positive FFR readings at baseline, which despite the change remained positive after caffeine.
A previous study to elucidate the effect of caffeine on FFR did not show a difference using intracoronary adenosine as a hyperaemic agent.4 Although there have been a multitude of studies comparing intravenous and intracoronary adenosine, intravenous adenosine is the most widely used method for inducing maximal hyperaemia.3
The competitive inhibition of adenosine A2a receptors with caffeine has been studied in a number of adenosine nuclear perfusion studies with mixed outcomes.7 ,8 Higher doses of adenosine (210 μg/kg/min) have been used by few to overcome the effect of caffeine on adenosine nuclear perfusion studies.8 Though our study did not include higher dose adenosine, it is plausible that similar effect may be seen in FFR readings. Further studies are needed to evaluate that.
Our study is limited by power to achieve any definitive conclusive results. Furthermore, orally consumed coffee or tea has other metabolites such as theophylline and theobromine that can have vasodilatory effects in addition to their adenosine inhibition similar to caffeine. Our study used intravenous caffeine administered over a short duration of time and may not have accounted for any additional effects of these metabolites on FFR. Another weakness of the study is that only 4 out of 10 patients had an FFR value ≤0.8. It does however raise questions which require larger trials to clarify. The present practice across majority of cardiac catheterisation laboratories for elective FFR or PCI is though variable, mostly involves a fasting period of >4 h, and caffeine history is not routinely obtained. Based on our findings, it may be hypothesised that sensitivity of caffeine and its inhibitory effect on adenosine can vary between the individuals and has potential to alter the FFR results. A caffeine history may be considered particularly in context of an unexpected FFR result.
Conclusion
Caffeine may affect FFR results in some patients. A larger scale trial is needed to clarify the extent and magnitude of caffeine/adenosine interaction particularly due to ubiquitous nature of caffeine and increasing importance of FFR in clinical practice.
Footnotes
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval The study complied with the declaration of Helsinki and was approved by institutional ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.