Article Text

Abstract
Aim The benefit of preventive percutaneous coronary intervention (PCI) in ST elevation myocardial infarction (STEMI) has been shown in randomised trials. However, all the randomised trials are underpowered to detect benefit in cardiac death. We aim to systematically review evidence on the cardiac mortality benefit of preventive PCI in patients presenting with acute STEMI in randomised patient populations.
Methods PubMed, Scopus, Cochrane and clinicaltrials.gov databases were searched for studies published until 30 September 2013. The studies were limited to randomised clinical trials. Independent observers abstracted the data on outcomes, characteristics and qualities of studies included. Fixed effect model was employed for meta-analysis. Heterogeneity of studies included was analysed using I2 statistics.
Results In three randomised clinical trials published, involving 748 patients with acute STEMI and multivessel disease, 416 patients were randomised to preventive PCI and 332 to culprit-only PCI. Patients undergoing preventive PCI had significant lower risk of cardiovascular deaths (pooled OR 0.39, 95% CI 0.18 to 0.83, p=0.01, I2=0%), repeat revascularisation (pooled OR 0.28, 95% CI 0.18 to 0.44, p=0.00001, I2=0%) and non-fatal myocardial infarction (pooled OR 0.38, 95% CI 0.20 to 0.75, p=0.005, I2=0%) compared with culprit-only revascularisation.
Conclusions In patients presenting with acute STEMI and significant multivessel coronary artery disease, based on our data, preventive PCI is associated with lower risk of cardiovascular mortality compared with primary PCI of only the culprit artery. This finding needs to be confirmed in larger adequately powered randomised clinical trials.
- Coronary Artery Disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
-
Percutaneous coronary intervention of culprit lesion is the standard of care for patients presenting with acute STEMI.
-
A significant number of patients with acute STEMI have significant multi-vessel coronary artery disease.
-
Stenting of not only culprit lesion but also significant non-culprit lesions may reduce the risk of death from cardiovascular causes.
Background
Timely primary percutaneous coronary intervention (PCI) of culprit coronary artery is the standard of care for patients presenting with acute ST elevation myocardial infarction (STEMI). However, the literature is conflicting regarding the benefit of PCI for significant stenoses in non-infarct arteries after successful primary PCI. The American College of Cardiology/American Heart Association (ACC/AHA) guidelines states that: “Primary PCI should not be performed in a noninfarct artery at the time of primary PCI in patients with STEMI who are hemodynamically stable” and “PCI is reasonable in a noninfarct artery at a time separate from primary PCI in patients with intermediate- or high-risk findings on noninvasive testing.”1 The European Society of Cardiology (ESC) guidelines state that PCI for STEMI should be limited to the culprit lesion except in patients with cardiogenic shock.2
In congruence with the clinical guidelines, several meta-analyses of observational and non-randomised studies show no benefit from PCI of the non-infarct artery.3–5 However, conclusions from these non-randomised and observational studies are limited by the potential for selection bias.6 A recent randomised clinical trial demonstrated benefit of preventive PCI in acute STEMI. Although this trial demonstrated benefit in the primary end point (composite of cardiac death, non-fatal myocardial infarction (MI) or refractory angina), there was no benefit in all-cause mortality or cardiovascular mortality.7 Earlier, two randomised clinical trials also failed to show mortality benefit associated with preventive PCI.8 ,9 Since these studies were not powered individually to assess for mortality, we systematically reviewed the benefit of preventive PCI in a randomised patient population presenting with acute STEMI.
Methods
A protocol for this meta-analysis was prospectively devised that details the background, the objectives, and eligibility criteria of studies, outcomes and statistical method. This is available for review on request to investigators.
Study selection
The PRISMA statement for reporting systematic reviews recommended by the Cochrane Collaboration was followed for conduct of this meta-analysis.10 Two authors (SG and MRA) searched PubMed, Scopus, Cochrane and clinicaltrials.gov databases for studies published until 30 September 2013 using search terms ‘ST elevation myocardial infarction AND coronary revascularization AND multivessel disease’ OR ‘complete revascularization AND multivessel revascularization AND culprit only revascularization AND myocardial infarction’ OR ‘ST elevation myocardial infarction AND coronary angioplasty AND multivessel AND non culprit’ OR ‘preventive angioplasty AND ST elevation myocardial infarction’.
We limited our search to randomised controlled trials. We checked reference lists of the relevant articles identified by the search strategy to find other potentially eligible studies. An additional author (AP) participated in the resolution process when uncertainty was encountered. When results were unclear or relevant data were not reported, authors of studies were contacted. Three authors (AAP, NRM and AP) independently collected and abstracted the data, which was further compared for any discrepancies.
The following inclusion criteria had to be met for studies to be included in the meta-analysis: (1) studies carried out on patients with acute STEMI with multivessel coronary artery disease (CAD), (2) randomised clinical trials, (3) multivessel revascularisation carried out during primary PCI or staged, (4) studies that reported outcomes of interest and (5) one of the comparators had to be culprit-only revascularisation. The primary outcomes of interest were the incidence of cardiac death, all-cause mortality, repeat revascularisation and reinfarction or non-fatal MI. We did not use composite of major adverse cardiovascular event (MACE) as outcome because of variability in definition of MACE in different trials.
Statistical analysis
All outcome comparisons and treatment effects were calculated with RevMan V.5.2 (Cochrane Collaboration, Oxford, UK). The summary OR and 95% CIs were estimated using Mantel-Haenszel fixed effect method. We calculated the I2 statistic to evaluate the percentage of heterogeneity among the trials. Sensitivity analysis was performed by meta-analysis based on timing of PCI; preventive PCI during primary PCI versus culprit artery-only PCI. As the study sample was limited to three, publication bias was not assessed. A p value of <0.05 was used as the level of significance.11
Outcomes assessed
The outcomes assessed for this meta-analysis were cardiovascular mortality, repeat revascularisation and non-fatal MI. The definition of end points was as defined by individual trials. Repeat revascularisation did not include planned staged PCI. While abstracting data for this meta-analysis for outcome variables, we chose data from the longest follow-up period reported in each of the studies. Preventive PCI was defined as complete revascularisation performed during primary PCI or staged PCI.
Results
Characteristics of included studies
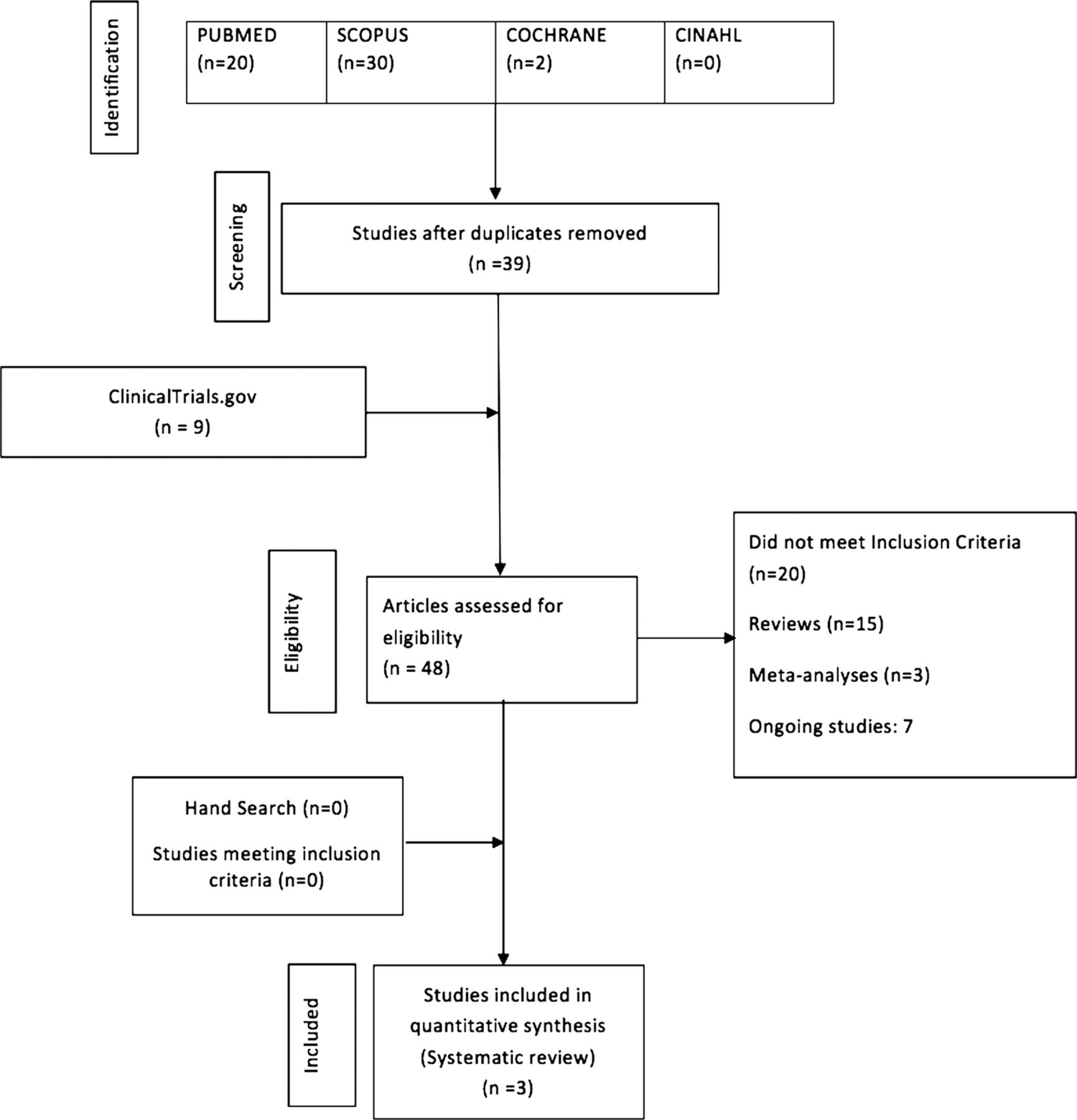
A total of 48 studies were assessed for eligibility. The steps of literature review and selection are summarised in figure 1. Only three randomised clinical trials met inclusion criteria.7–9 A quality assessment was performed at study level for all the included studies and is shown in table 1. Three studies included collected data between 2004 and 2013. A total of 748 patients were randomised to primary PCI of culprit artery (n=332) and preventive PCI (n=416). Inclusion and exclusion criteria for each study are found in table 2. Patients in Wald et al7 and Politi et al8 did not significantly differ in clinical characteristics with treatment arms at baseline. However, in Di Mario et al9 study, patients in the primary PCI of culprit artery group had a higher number of patients with diabetes. The mean follow-up time was 21 months for all studies and follow-up time ranged 12–30 months. Each study differed for primary efficacy end point or major adverse cardiovascular end points (MACE) as shown in table 2. We did not use MACE as an outcome because of variability in definition of MACE in each study; rather we preferred to use individual end points as outcome variables. Repeat revascularisation was performed when there was objective evidence of ischaemia.
Quality assessment of included study
Characteristics of included randomised clinical trials

Flow chart describing systematic research and study selection process.
Outcomes
Preventive PCI at the time of primary PCI or staged versus PCI limited to the culprit artery
Cardiovascular mortality
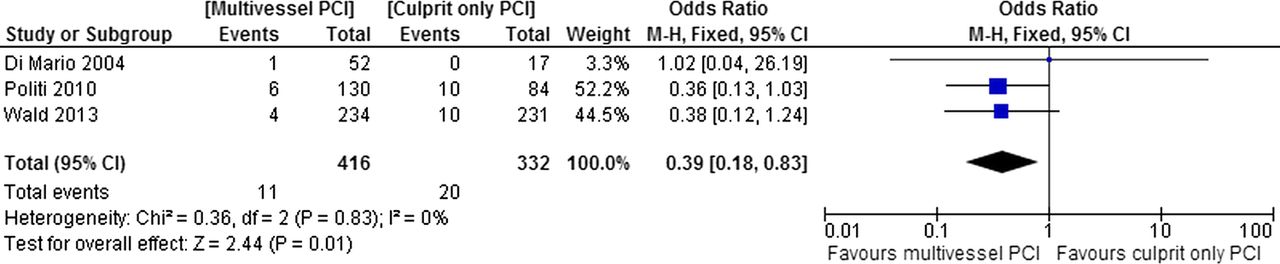
Cardiovascular death occurred in 11 of 416 (2.64%) patients in preventive PCI group compared with 20 of 332 (6%) in culprit artery-only PCI group (pooled OR 0.39, 95% CI 0.18 to 0.83, p=0.01, I2=0%), as shown in figure 2. The relative risk reduction was 61% and absolute risk reduction was 3.36%. The number needed to prevent one cardiovascular death was calculated to be 30.

Meta-analysis of cardiovascular mortality in randomised trials. Comparator: preventive percutaneous coronary intervention (PCI) versus culprit artery-only PCI.
Repeat revascularisation
Repeat revascularisation occurred in 39 of 416 (9.37%) patients in preventive PCI group compared with 80 of 332 (24%) in culprit-only PCI group (pooled OR 0.28, 95% CI 0.18 to 0.44, p=0.00001, I2=0%), as shown in figure 3. There was very significant reduction of repeat revascularisation in preventive PCI group.
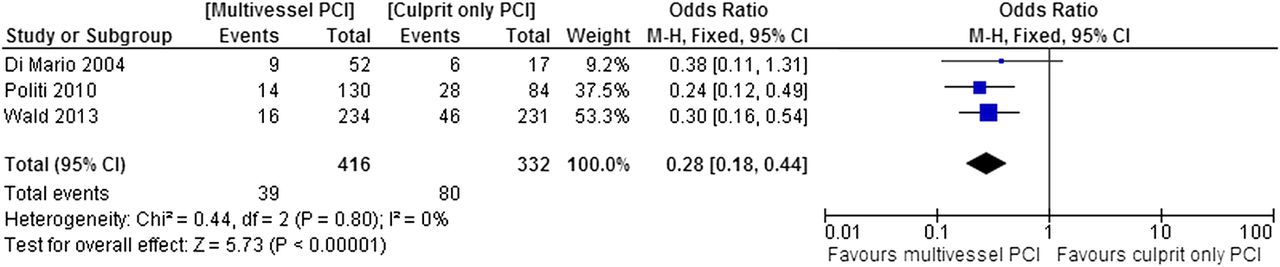
Meta-analysis of repeat revascularisation in randomised trials. Comparator: preventive percutaneous coronary intervention (PCI) versus culprit artery-only PCI.
Non-fatal MI
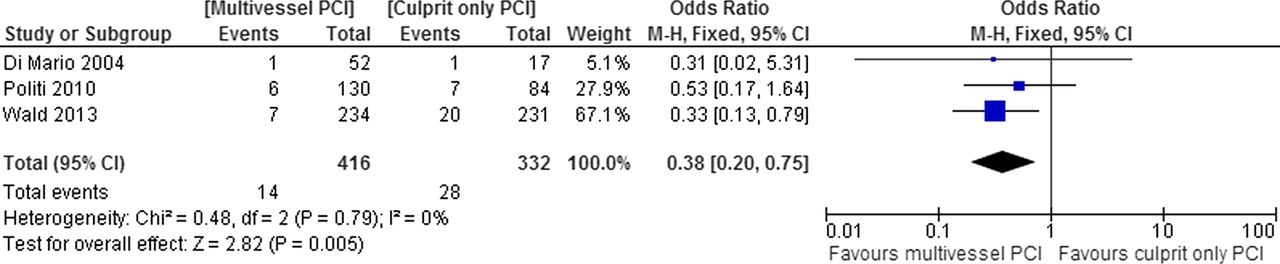
Non-fatal MI occurred in 14 of 416 (3.36%) patients in preventive PCI group compared with 28 of 332 (8.4%) in culprit artery-only PCI group (pooled OR 0.38, 95% CI 0.20 to 0.75, p=0.005, I2=0%), as shown in figure 4.
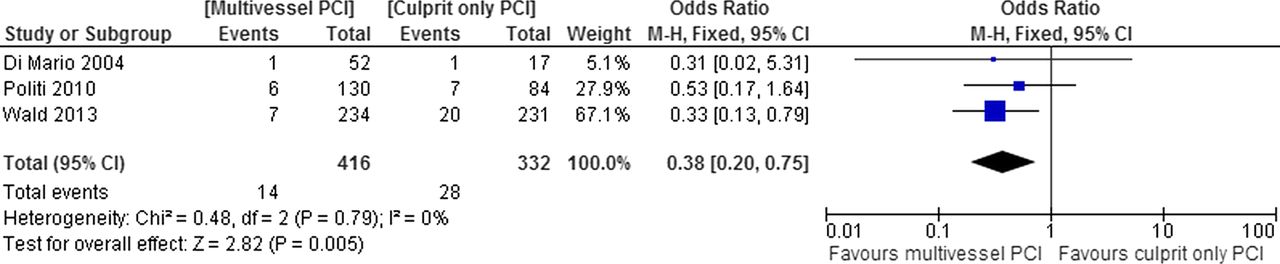
Meta-analysis of recurrent or non-fatal myocardial infarction in randomised trials. Comparator: preventive percutaneous coronary intervention (PCI) versus culprit artery-only PCI.
Preventive PCI at the time of primary PCI versus PCI limited to the culprit artery
Cardiovascular mortality
Cardiovascular deaths occurred in 9 of 351 (2.56%) patients in preventive PCI group compared with 20 of 332 (6.02%) in culprit artery-only PCI group (pooled OR 0.45, 95% CI 0.20 to 1.01, p=0.05, I2=0%), as shown in figure 5. There was absolute risk reduction of 3.5% in cardiovascular mortality favouring strong trend towards benefit.
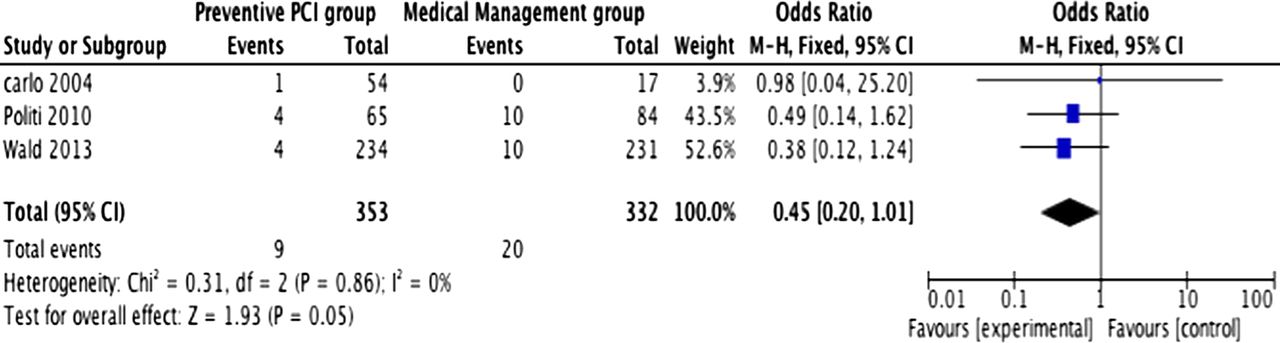
Meta-analysis of cardiovascular mortality in randomised trials. Comparator: preventive percutaneous coronary intervention (PCI) at the time of primary PCI versus culprit artery-only PCI.
Repeat revascularisation
Repeat revascularisation occurred in 31 of 351 (8.8%) patients in preventive PCI group compared with 80 of 332 (24%) in culprit artery-only PCI group (pooled OR 0.28, 95% CI 0.17 to 0.44, p<0.00001, I2=0%), as shown in figure 6A.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Meta-analysis of repeat revascularisation in randomised trials. Comparator: preventive percutaneous coronary intervention (PCI) at the time of primary PCI versus culprit artery-only PCI. (B) Meta-analysis of non-fatal myocardial infarction in randomised trials. Comparator: preventive PCI at the time of primary PCI versus culprit artery-only PCI.
Non-fatal MI
Recurrent or non-fatal MI occurred in 10 of 351 (2.84%) patients in preventive PCI group compared with 28 of 332 (8.43%) in culprit artery-only PCI group (pooled OR 0.33, 95% CI 0.16 to 0.70, p=0.004, I2=0%), as shown in figure 6B.
Discussion
Findings
The main finding of this meta-analysis is demonstration of significant benefit on cardiovascular mortality in patients undergoing preventive PCI in patients presenting with STEMI and multivessel CAD when compared with primary PCI of the culprit artery. Another important finding was a significant benefit on repeat revascularisation and recurrent or non-fatal MI.
Comparison with other meta-analyses
Results of present meta-analysis are different from those published earlier on this topic. A meta-analysis published in 2011 concluded no benefit of complete revascularisation over culprit artery-only revascularisation.3 ,5 This meta-analysis was limited by a high degree of heterogeneity among the trials included in the study, and it was mostly comprised of non-randomised studies. Another meta-analysis published on the same topic involving mainly non-randomised study did not show clear benefit of complete revascularisation over culprit artery-only revascularisation.4 Particularly, the meta-analysis published by Vlaar et al,5 which included 4 prospective and 14 retrospective studies with 40 280 patients, demonstrated that multivessel complete PCI was associated with higher mortality compared with culprit artery-only or staged PCI. Our results are different from this study because we included data from recently published largest randomised clinical trial and we excluded a study by Ochala 2004 (though randomised study) because comparators were complete revascularisation versus staged PCI, not culprit artery-only revascularisation. We believe that earlier meta-analyses were not able to show mortality benefit mainly because of the inclusion of non-randomised and observational studies, which have the inherent risk of selection biases. In the studies used for our meta-analysis, the Wald 2013 trial was the largest with 465 patients. Subsequent PCI was recommended or encouraged only in those patients with medically refractory angina, and objective assessment of reversible ischaemia. The primary outcome was a composite of cardiovascular death, non-fatal MI and refractory angina. The Politi 2010 trial enrolled 214 patients and was randomised to three strategies. Culprit artery-only PCI was compared with staged PCI and with simultaneous PCI. The primary endpoint was MACE defined as cardiac or non-cardiac death, in hospital death, reinfarction, rehospitalisation for acute coronary syndrome and repeat coronary revascularisation. The smallest study enrolling 69 patients was DiMario 2004, which specified the primary endpoint as 12-month incidence of repeat revascularisation.
The findings of our study seem to be more reliable and consistent because of lack of heterogeneity among the included trials as shown by I2 statistics of 0% across all outcome variables assessed. We clearly showed for the first time that preventive PCI at the time of primary PCI, or when staged, has benefit on cardiovascular mortality in a randomised patient population.
Clinical implications
Current AHA/ACC guidelines for STEMI states “more work is needed to clarify the indications for and timing of non-infarct artery revascularisation.”1 Patients presenting with acute STEMI have significant multivessel CAD in one-third to two-third of patients and this is associated with significant morbidity and mortality.11 Further, AHA/ACC 2013 STEMI guidelines states “ there seems to be a clear trend toward lower rates of adverse outcomes when primary PCI is limited to the infarct artery and PCI of a non-infarct artery is undertaken in staged fashion at a later time.”1 The studies looking into preventive PCI among patients with stable angina and significant lesions observed during coronary angiography have failed to prevent death and MI.12 The recently published larger randomised clinical trial showed benefit of preventive PCI in STEMI with regard to composite end point of cardiac death, non-fatal MI and recurrent angina.7 This study demonstrated benefit on recurrent MI but failed to show benefit on cardiovascular mortality. The study, however, was not powered to demonstrate cardiovascular mortality.7 The findings of our meta-analysis are very important because it suggests that cardiovascular mortality is higher with culprit artery-only PCI when compared with preventive PCI in randomised patient population. It is not known whether real-time evaluation of non-culprit artery lesions by intravascular ultrasound or fractional flow reserve in this patient population would be more effective than angiography alone in identifying lesions that warrant PCI. Findings of our meta-analysis are different from the current opinion that PCI of non-infarct-related artery during primary PCI is associated with, and increase in, adverse outcomes.1 The findings of our meta-analysis conflict with PCI revascularisation strategies in stable patients with coronary disease such as the COURAGE trial, which showed no clear advantage of elective PCI over optimal medical therapy.13 This discrepancy is likely due to, at least in part, because of inherent differences of the coronary system in an acute, inflammatory clinical setting such as an acute coronary syndrome compared with a chronic, stable CAD. This includes the finding that non-culprit arteries can be found to also have a vulnerable, inflamed states during acute coronary syndrome.14 ,15 Prophylactic revascularisation in this circumstance could be hypothesised to decrease the incidence of MACE.
Strengths and limitations
The potential limitation of this meta-analysis could be the small number of included randomised trials. However, it should be emphasised that there are only three randomised trials conducted to date on this subject that met inclusion criteria.7–9 One randomised clinical trial did not meet inclusion criteria because it compared staged PCI with PCI of non-infarct artery during primary PCI.16 The control group in our study was determined to be culprit artery-only revascularisation. Despite having smaller randomised clinical trials, this meta-analysis demonstrated benefit in cardiovascular mortality and very significant benefit on repeat revascularisation and non-fatal MI. We followed rigorous steps in conducting meta-analysis as recommended by PRISMA statement; therefore, we believe that our findings are valid and robust. Another limitation of this meta-analysis is lack of patient-level data, which precluded us from performing covariate-adjusted analysis or time-to-event analysis.
Other limitations include limited availability of procedural and index hospitalisation details from the studies included in the analysis. Thus, we have not assessed procedural risks, length of hospitalisation and financial implications of preventive PCI.
Conclusions
In patients presenting with acute STEMI and significant multivessel CAD, based on our data, preventive PCI is associated with lower cardiovascular mortality compared with primary PCI of only the culprit artery. This finding needs to be confirmed in larger adequately powered randomised clinical trials.
References
Footnotes
-
Contributors AP conceived, designed, participated in data abstraction, analysis, interpretation and drafting of the manuscript. HRL, FAH, FDF and FM analysed, interpreted data and provided intellectual content and approved the final manuscript. MRA, AAP, NRM, PS and SG participated in data abstraction, analysis, interpretation and final approval of the manuscript. AP is responsible as overall guarantor of the content.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.