Article Text

Abstract
Objective Adults operated for tetralogy of Fallot (TOF) have high risk of ventricular arrhythmias (VA). QRS duration >180 ms is an established risk factor for VA. We aimed to investigate heart function, prevalence of arrhythmias and sex differences in patients with TOF at long-term follow-up.
Methods We included TOF-operated patients≥18 years from our centre’s registry. We reviewed medical records and the most recent echocardiographic exam. VA was recorded on ECGs, 24-hour Holter registrations and from implantable cardioverter defibrillator.
Results We included 148 patients (age 37±10 years). Left ventricular global longitudinal strain (LV GLS, −15.8±3.1% vs −18.8±3.2%, p=0.001) and right ventricular (RV) GLS (−15.8±3.9% vs −19.1±4.1%, p=0.001) were lower in men at all ages compared with women. Higher RV D1 (4.3±0.5 cm vs 4.6±0.6 cm, p=0.01), lower ejection fraction (55%±8% vs 50%±9%, p=0.02), lower RV GLS (−18.1±4.0 ms vs −16.1±4.8 ms, p=0.04) and N-terminal pro-brain natriuretic peptide (NT-proBNP) over reference range (n=27 (23%) vs n=8 (77%), p<0.001) were associated with higher incidence of VA. QRS duration was longer in men (151±30 ms vs 128±25 ms, p<0.001). No patients had QRS duration >180 ms. QRS duration did not differ in those with and without VA (143±32 ms vs 137±28 ms, p=0.06).
Conclusions Our results confirmed reduced RV function in adults operated for TOF. Male patients had impaired LV and RV function expressed by lower LV and RV GLS values at all ages. Reduced cardiac function and elevated NT-proBNP were associated with higher incidence of VA and may be important in risk assessment.
- echocardiography
- arrhythmias
- cardiac
- tetralogy of Fallot
- heart failure
- systolic
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Previous studies showed that ventricular arrhythmias (VA) and heart failure are common complications in adult patients operated for tetralogy of Fallot (TOF). A QRS duration >180 ms is an established risk factor for VA.
What does this study add?
Male patients operated for TOF had significantly impaired left and right ventricular function compared with female patients, expressed by lower left ventricular and right ventricular global longitudinal strain values at all ages.
This study provides an insight on the long-term follow-up in adults operated for TOF. Our investigation showed that in adults operated for TOF, a reduced cardiac function and elevated N-terminal pro-brain natriuretic peptide (NT-proBNP) values were associated with higher incidence of VA. A QRS duration >180 ms did not emerge as associated to VA, as no patients had so prolonged QRS length.
How might this impact on clinical practice?
Reduced cardiac function and elevated NT-proBNP, together with QRS duration shorter than 180 ms, might become parameters to consider in risk stratification in patients operated for TOF, especially considering the incidence of VA.
Introduction
Tetralogy of Fallot (TOF) has an incidence of 0.34 per 1000 live births,1 and is the most common cyanotic congenital heart disease.2
Since the first surgical repair of TOF reported in 1954,3 the life expectancy of children born with TOF has dramatically improved to a survival of 94% at 25 years,4 and 72% at 40 years,5 following TOF repair. After surgical correction, patients generally enjoy a good quality of life that is almost similar to that of the general population.6 7 However, long-term survival is still significantly lower than in the general population.8
Despite significant advances in treatment and management, previous studies have documented a high risk of arrhythmias in patients with TOF.9 10 Especially ventricular arrhythmias (VA) and sudden cardiac death (SCD) remain major concerns in adults corrected for TOF late after surgical repair.
Previous reports have indicated a slightly higher prevalence of atrial and VA in male patients; however, significant sex differences in cardiac function and outcome are not known.9 10
We aimed to investigate cardiac function, prevalence of VA and heart failure in adult patients operated for TOF. Furthermore, we aimed to explore possible sex differences.
Methods
Data collection
For this retrospective cohort study, we reviewed our centre’s Adult with Congenital Heart Disease (ACHD) patients’ registry which includes all adult patients with congenital heart diseases who have been diagnosed, treated, followed and/or operated at Oslo University Hospital, Rikshospitalet, Norway in the period 1970–2020.
Patient and public involvement statement
This research was conducted without patient involvement in the study design, interpretation of results and writing this manuscript. The research project was presented to the Norwegian Association of Adults with Congenital Heart Diseases (VMH, Voksne med medfødt hjertefeil) prior to the initiation.
Inclusion criteria
All patients diagnosed with TOF, who were ≥18 years of age at the time of follow-up and with a history of surgical correction, were recruited from the ACHD registry. All medical records available within the past 5 years (2015–2020) were reviewed. All forms of surgical repair were considered, including cases where Waterstone or Blalock-Taussig shunt was performed prior to surgical correction.
Patients were contacted with an information letter; all of them agreed to participate to the study and informed consent was obtained from each patient.
Exclusion criteria
We excluded patients who were incapable to give informed consent.
Clinical characteristics
Patients were classified according to the severity of symptoms of heart failure using New York Heart Association (NYHA) Functional Classification.
We included patients’ most recent ECG and assessed rhythm, heart rate, PQ - QRS - QTc interval,11 and bundle branch block.
Exercise capacity was routinely assessed by exercise stress test in all patients during regular annual/biannual follow-up. Patients performed exercise stress test following Bruce protocol,12 on a bicycle ergometer, and we used results from the most recent exercise test.
We recorded N-terminal pro-brain natriuretic peptide (NT-proBNP) as a marker of heart failure from the most recent clinical visit. The reference values for NT-proBNP were age and sex specific13 (Elecsys—Roche Diagnostics, Basel, Switzerland): <170 ng/L for women<49 years of age, <85 ng/L for men <49 years of age, <300 ng/L for women 50–69 years of age, <250 ng/L for men 50–69 years of age.
Echocardiography
The most recent echocardiographic exam for each patient, performed during the period 2015–2020, was analysed offline on EchoPAC V.201, GE Healthcare, Horten, Norway. Echocardiography included all measurement obtained during a standard echocardiogram performed (M-mode, B-mode, colour Doppler, pulsed-wave and continuous-wave Doppler), including left ventricular (LV) ejection fraction (EF) calculated by the modified Simpson’s biplane method. The right ventricular (RV) basal, mid and longitudinal diameter and the RV fractional area change (FAC) were obtained from the RV-focused view. In addition, we assessed cardiac function by global longitudinal strain (GLS) using a speckle tracking technique at frame rates>50/s. LV GLS was defined as the average of peak systolic negative longitudinal deformation/strain from the three apical views.14 RV GLS was defined as an average peak negative systolic longitudinal strain from RV-focused 4-chamber view.15 16
Mechanical dispersion, a measure of RV and LV contraction heterogeneity,15 was defined as the SD of the time interval from onset of the Q/R wave in the ECG to the peak negative longitudinal strain in, respectively, 6 RV and 18 LV segments.
Ventricular arrhythmias
We recorded the occurrence of VA on ECGs, 24-hour Holter registrations and from implantable cardioverter defibrillator (ICD) monitoring.
We considered the following VA as clinically relevant: non-sustained ventricular tachycardia (NSVT), defined as consecutive runs of ≥3 ventricular beats>100 beats/min for <30 s; sustained ventricular tachycardia (VT), defined as runs of consecutive ventricular beats>100 beats for >30 s17; ventricular fibrillation (VF) with appropriate therapy from an ICD; aborted cardiac arrest (CA).
Statistics
We performed statistical analysis by using IBM SPSS V.26. Data were presented as mean±SD or median with range, as appropriate. We performed the comparisons of continuous data by the unpaired Student’s t-test or Mann-Whitney U test and compared categorical variables by the χ2 test or Fisher’s exact test as appropriate. We showed the differences in the ventricular function in male and female patients by Kaplan-Meier curve. P values ≤0.05 were considered statistically significant.
Results
Clinical characteristics
We included 148 patients, of which 80 (54%) were women. Mean age at the time of follow-up was 37±10 years (38±10 years for men vs 37±10 years for women, p=0.52; table 1). Mean time surgery-to-follow-up was 32±9 years (33±8 in men vs 31±10 in women, p=0.25).
Clinical characteristics in patients with tetralogy of Fallot
Age at surgical correction was 4 years (1–15) and number of operations was 1 (1–4), with no differences between sexes. All clinical characteristics were similar, except for larger body size and higher systolic blood pressure (SBP) in men (table 1).
ECG, exercise capacity and heart failure
Mean heart rate was 70±13 beats/min and QTC duration was 457±45 ms, similar in both sexes.
Mean QRS duration was prolonged with 141±30 ms, with significantly longer QRS duration in male patients (151±30 ms vs 128±25 ms, p<0.001; table 1).
The total population had mean exercise capacity of 155±38 W, with men having higher exercise capacity than women (174±35 watt vs 131±27 watt, p<0.001; table 1). NYHA class was equal between sexes.
More than half of patients (53%) had NT-proBNP above normal values, with similar prevalence in men and women (p=0.19; table 1).
One patient required heart transplant at the age of 40 due to biventricular heart failure.
Echocardiographic parameters
In the total population, RV dimensions were increased compared with normal values also when indexed for body surface area. RV and LV global function were slightly impaired measured by EF and GLS (table 2).
Echocardiographic parameters in patients with tetralogy of Fallot
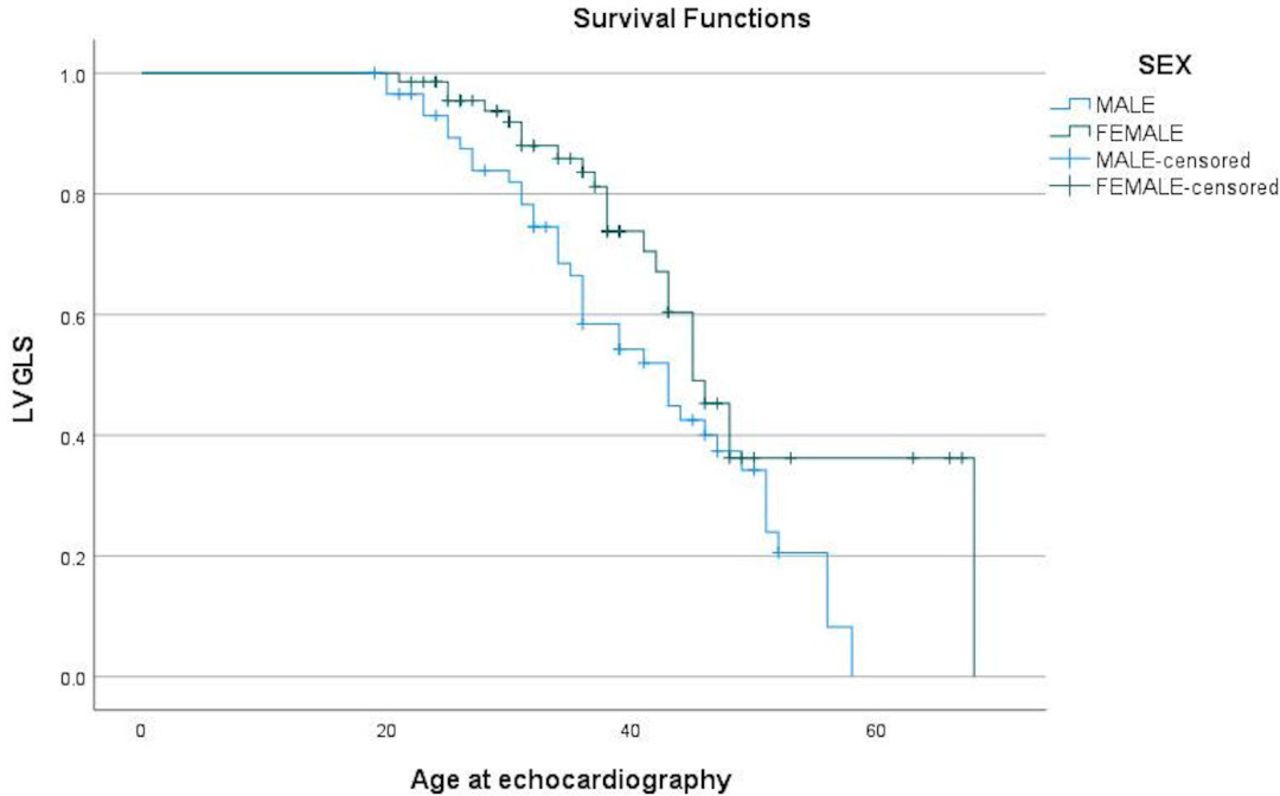
Cardiac function of RV and LV were significantly impaired in men compared with women, expressed by lower LV EF and both RV and LV GLS (p=0.001; table 2). LV GLS and RV GLS were lower in male patients operated for TOF in all age groups (figures 1 and 2).

LV GLS values in male and female patients with TOF according to age. LV GLS values were showed to be lower in male patients operated for TOF in all age groups compared with female patients. LV GLS, left ventricular global longitudinal strain; TOF, tetralogy of Fallot.

{kind=link}
{kind=link}
RV GLS values in male and female patients with TOF according to age. RV GLS values were lower in male patients with TOF in all age groups. RV GLS, right ventricular global longitudinal strain; TOF, tetralogy of Fallot.
No sex differences were observed in RV and right ventricular outflow tract diameters, RV FAC nor in LV and LVOT diameter (table 2).
Incidence of VA
In all, VA occurred in 35 patients at a mean age of 38±9 years, 32±6 years after surgery. Sustained VA was the first registered VA in 19 patients, while 17 patients had NSVT as first presentation of VA.
In all, 22 (14%) patients were implanted with ICD (16 secondary preventive ICD and 6 primary preventive ICD).
Higher RV D1 (4.3±0.5 vs 4.6±0.6, p=0.01), lower EF (55±8 vs 50±9, p=0.02) and lower RV GLS (−18.1±4.0 vs −16.1±4.8, p=0.04) in the entire cohort were associated with higher incidence of VA (table 3). RV D1 had strongest association to incidence of VA (table 3).
Risk factors and incidence of VA in patients with TOF
Patients with VA had more frequently NT-proBNP over reference range (n=27 (23%) vs n=8 (77%), p<0.001). NT-proBNP values were missing for five patients.
We found no differences in the incidence of VA, nor at age at VA between men and women (table 3). Male patients had mostly experienced sustained VT (77%) as first presentation of VA, while female patients frequently had NSVT (76%) at first VA presentation (p<0.01). VA had occurred at median 7 years (range 1–18 years) prior to last follow-up.
QRS duration did not differ in those with and without VA (143±32 ms vs 137±28 ms, p=0.2).
Of the 22 patients with ICD, 13 were men (59%). ICD had been implanted in 19% of the male cohort compared with 11% of the female cohort (table 1).
Discussion
This study confirmed reduced RV and LV function in adult patients operated for TOF. Interestingly, we showed that male patients had more reduced cardiac function at follow-up at all ages, indicating a more severe heart failure outcome compared with female patients. The incidence of VA was similar in men and women and 1 out of 4 patients experienced VA at the age of 38±9 years, an average of 32 years after surgical repair.
Heart failure outcome
In our study, patients operated for TOF showed lower RV function and dilated RV at long term follow-up. Similar results were showed in other adult TOF populations, where RV GLS was reduced compared with normal controls, despite unchanged RV EF on cardiac magnetic resonance and only modest RV dilatation.18 The decrease in strain values compared with healthy subjects is not unexpected, as both the anatomical features of the congenital heart disease and the following surgical correction influence the ventricular contractility resulting in alteration of GLS.
Also, LV function was decreased in our patients with TOF. Several studies investigating ventricular function and contractility have been conducted on patients with TOF. One study showed that asymptomatic paediatric TOF population with a normal LV EF already exhibited abnormal segmental and global LV longitudinal and circumferential strains compared with a matched healthy control group.19
Interestingly, our study showed that male patients with TOF had worse RV function compared with female patients at long-term follow-up. This finding supports previous findings of Menting et al as they showed that male patients with TOF had significantly lower LV GLS and RV free wall strain compared with female patients and speculated that RV dysfunction adversely affects LV function, probably by mechanical coupling of the ventricles.20
Cut-off values and possible explanations for sex differences in RV function
In a healthy population, LV GLS <−16% and RV GLS <−23% are generally considered abnormal.21 22 Extremes of age and SBP may be related to lower LV GLS values. There are currently no reference values for RV GLS in patients after corrective surgery for TOF. However, in other cardiomyopathies affecting primarily the RV, as arrhythmogenic RV cardiomyopathy, the cut-off value for abnormal RV GLS proposed is −18%.15 In our cohort of patients with TOF, more than 30 years after surgery, RV and LV GLS and global LV EF was impaired in men with TOF at all ages, while women had GLS values within the reference range of normal population. Higher SBP values reported in our male patients with TOF might influence GLS values, although SBP was within normal range in our male patients (<130 mm Hg). Lower RV and LV GLS values in male patients at all ages, together with lower EF, might reveal a subclinical myocardial dysfunction and consequently an early stage of heart failure ahead of the symptomatic phase which occur earlier than in female patients.
NYHA class level and the generally good exercise capacity in both men and women supported that myocardial dysfunction was mainly asymptomatic. However, more than 50% of patients with TOF had elevated NT-proBNP values, supporting the finding of subclinical heart failure confirmed by imaging parameters.
Incidence of VA and device therapy
Our study confirmed a high incidence of VA of 25% 30 years after surgery in patients with TOF. A large multicentre study reported SCD as the most common causes of death in TOF with 49%, followed by heart failure (27%) and coronary artery disease (6%).9
Importantly, our study showed that in the entire TOF cohort reduced cardiac function expressed by reduced EF and RV GLS was associated with VA, highlighting the importance of follow-up cardiac imaging in risk assessment for VA in these patients. GLS has been shown to predict VA in certain patient populations, as after myocardial infarction and in arrhythmogenic RV cardiomyopathy.15 23 Similarly, use of strain echocardiography for arrhythmic risk assessment could be broadened to patients with congenital heart disease, in particular patients operated for TOF. The incidence of VA was equally represented in both sexes and VA occurred at approximately the same age for male and female patients. This finding confirmed that the arrhythmic burden is equally distributed in both sexes during adult life as showed in previous multicentre studies.9 10 In contrast, men in the general population have higher risk of sudden CA than women, in all age groups,24 and the higher incidence of coronary artery disease and a higher prevalence of cardiac structural abnormalities may explain these differences.25 Our patients were young and probably too young to include the full risk regarding coronary artery disease. Nevertheless, the equal VA incidence between sexes in our TOF population may indicate a relatively higher risk of SCD in female patients with TOF compared with the general population.
A similar pattern is observed in some cardiomyopathies, where male patients have generally higher risk of severe VA. In arrhythmogenic RV cardiomyopathy, male sex is one of predictors for VF and ICD therapy.26 In a similar way, a history of VF is more frequent in men with Brugada syndrome, being the age at the onset of VF also lower in men than in women.27
Our study confirmed prolonged QRS duration in long-term follow-up of patients with TOF as reported previously,28 with the novel finding of longer QRS duration in male patients. An increased QRS duration has previously been recognised as risk factor for VA and SCD in patients with TOF. QRS duration of 180 ms or more, QRS duration rate of change (>3 ms per year over a 10-year period), older age at repair and pulmonary regurgitation were the most important risk markers of VA and SCD in adults with repaired TOF. In contrast, we found no association between QRS duration and VA in our population. None of our patients diagnosed with severe VA presented QRS duration >180 ms. This finding highlights increased arrhythmic risk also at QRS duration below 180 ms.
In our cohort, 14% of patients had received ICD implantation during adult life. We found no sex differences in frequency of ICD implantation (19% of men, 11% of women). However, we cannot exclude that larger studies may show sex differences.
The reason of a more balanced distribution of severe VA between sexes in patient with TOF compared with the general population and to cardiomyopathies is currently not known. One might speculate that the prolonged and, in some cases, reiterated haemodynamic stress occurring in pregnancy,29 might outweigh females’ benefit and increase the risk of VA in female patients with TOF, according to a previous report.30
Study limitations
This was a cross-sectional cohort study with retrospective event adjudication, with intrinsic limitations. We cannot draw a conclusion about causal connection, and we cannot measure incidence. The relatively limited sample size may give rise to insufficient power to detect subtle differences.
Conclusion
This study confirmed reduced RV function in adult patients operated for TOF at long-term follow-up. Male patients had significantly impaired LV and RV function expressed by lower LV and RV GLS values at all ages.
The incidence of VA was high, 25% at 30 years after surgery and was similar between sexes. Reduced cardiac function and elevated NT-proBNP were associated with higher incidence of VA and may be important in risk assessment.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The study conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the Regional Committees for Medical Research Ethics (reference number 2017/383).
Acknowledgments
We thank all the patients that participated in this study.
References
Footnotes
Contributors AQ: acquired data, analysed data, performed statistical analysis, writing. OHL and KH: analysed data, performed statistical analysis, made critical revision of the manuscript. EN: designed the study, made critical revision of the manuscript for important intellectual content. CdL and HLL: conceived and designed the study, made critical revision of the manuscript for important intellectual content. KT: acquired data, made critical revision of the manuscript for important intellectual content. HS and GE: acquired data, made critical revision of the manuscript for important intellectual content. TE: handling the funding, made critical revision of the manuscript. MEE: conceived and designed the research, made critical revision of the manuscript for important intellectual content, handling funding and supervision, writing.
Funding This study was supported by the South-Eastern Norway Regional Health Authority (NR 2017103).
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.