Article Text

Abstract
Introduction Pulmonary vein isolation (PVI) is an important treatment for atrial fibrillation (AF). However, many patients need more than one procedure to maintain long-term sinus rhythm. Even after two PVIs some may suffer from AF recurrences. We aimed to identify characteristics of patients who fail after two PVI procedures.
Methods and results We included 557 consecutive patients undergoing a first PVI procedure with a second-generation 28 mm cryoballoon. Follow-up procedures were performed using radiofrequency ablation targeting reconnected PVs only. Recurrent AF was defined as any episode of AF lasting >30 s on ECG or 24 hour Holter monitoring performed at 3, 6 and 12 months post procedure. Mean age was 59.1±10.2 years, 383 (68.8%) were male, 448 (80.4%) had paroxysmal AF and the most common underlying condition was hypertension (36.6%). A total of 140/557 (25.1%) patients underwent redo procedure with PVI only. Of these patients 45 (32.4%) had recurrence of AF. These patients were comparable regarding age and sex to those in sinus rhythm after one or two procedures. Multivariate logistic regression showed that non-paroxysmal AF (OR 1.08 (95% CI 1.01 to 1.15), estimated glomerular filtration rate (OR 0.96, 95% CI 0.94 to 0.99), bundle branch block (OR 4.17, 95% CI 1.38 to 12.58), heart failure (OR 4.17, 95% CI 1.38 to 12.58) and Left Atrium Volume Index (OR 1.04, 95% CI 1.01 to 1.08) were associated with AF recurrence after two PVIs. The area under the curve for the identified risk factors was 0.74.
Conclusions Using a PVI-only approach, recurrence of AF after two AF ablation procedures is associated with more advanced underlying disease and persistent types of AF.
- atrial fibrillation
- electrophysiology
- risk factors
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon a reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Pulmonary vein isolation (PVI) is an important treatment for patients with symptomatic atrial fibrillation (AF).
Unfortunately, many patients have a recurrence of AF after one procedure.
Underlying risk factors increase the likelihood for a recurrence after one PVI.
What does this study add?
This is a large cohort of patients who had a recurrence of AF after cryoballoon PVI. At redo procedure only, the pulmonary veins were addressed and no additional ablation was performed demonstrating PVI outcome after index and redo PVI-only approach.
At multivariate analysis, analysing indicators for failure of a PVI-only approach underlying conditions (heart failure, bundle branch block, Left Atrium Volume Index, estimated glomerular filtration rate) and persistent types of AF were identified.
How might this impact on clinical practice?
It is critical to understand which patients have long-term benefit from a strategy including PVI. Addressing the underlying conditions before the procedure might be essential to secure long-term results.
Future PVI studies could furthermore implement these risk factors for diverse PVI strategies in different patient populations.
Introduction
Recent guidelines consider catheter ablation as first-line treatment especially for paroxysmal atrial fibrillation (AF).1 The hallmark of AF ablation is isolation of the pulmonary veins (PVIs).2 3 Unfortunately, a significant proportion of patients experience AF recurrences following PVI (10%–35% in the first year) and need a redo procedure.4 5
AF recurrences may occur due to reconnection of the pulmonary veins. Other reasons for AF recurrence include non-PV triggers and extensive atrial structural remodelling.6 7 Contributing to these recurrences of AF may be specific risk factors such as type of AF, size of the left atrium (LA) and presence of comorbidities.8–11 These have been implemented into risk scores that can be used to predict failure after single PVI.1 12 13
There is a wide variety of ablation strategies that can be performed at the redo procedure including reisolation of the PVs, non-PV trigger ablation and substrate ablation.1 14 15 Recently, more extensive ablation beyond the PVI was shown to be equally effective as PVI alone in patients with persistent AF.3 For this reason, it is reasonable to use a PVI ablation-only approach for paroxysmal and persistent AF. Consequently, at redo procedures, reisolation of the PVs (resulting in a higher portion of patients who will achieve PV isolation) is commonly performed. The evidence for additional atrial ablation is limited and atrial tachycardias/flutter may occur as a result of re-entry in incomplete lines.
Unfortunately, also after redo PVI ablation, AF recurrences occur. Since it is likely that the PVs are isolated in these patients, the AF recurrence should be explained by mechanisms beyond the PVs. These patients may potentially benefit from ablation at additional locations.
Thus, it is important to identify patients who benefit from a PVI-only approach and/or vice versa, who may be candidates for additional atrial ablation. For this purpose, we identified patients who had a recurrence of AF despite two ablation procedures targeting only the PVs. The result of the present analysis may improve future patient selection and determine AF ablation strategy.
Methods
Patient selection
In total, 557 of 646 patients were selected from our AF Cryoballoon Registry at the University Medical Center Groningen. These were consecutive patients who underwent their first PVI between 2013 and 2017. To address the aim of the study, two groups of patients were identified. Group 1 included patients with a successful AF ablation outcome after the index or redo PVI procedure. Group 2 consisted of patients who had recurrence of AF despite two PV ablation-only procedures or who had already isolated PVs (no reconnections) at the redo procedure (failed PVI approach). The following patients were excluded from the analysis: patients with failed PVI who did not undergo a second PVI or patients with failed index PVI who had additional non-PVI ablation (lines, posterior wall isolation). Patients who underwent a pace and ablate strategy or a surgical AF ablation as follow-up procedure were consequently excluded. For the final analysis, we compared patients with failed PVI approach (failure after second PVI only) to successful PVI approach (figure 1). All data were retrospectively collected from the patients’ medical files. All patients consented to the ablation procedures.
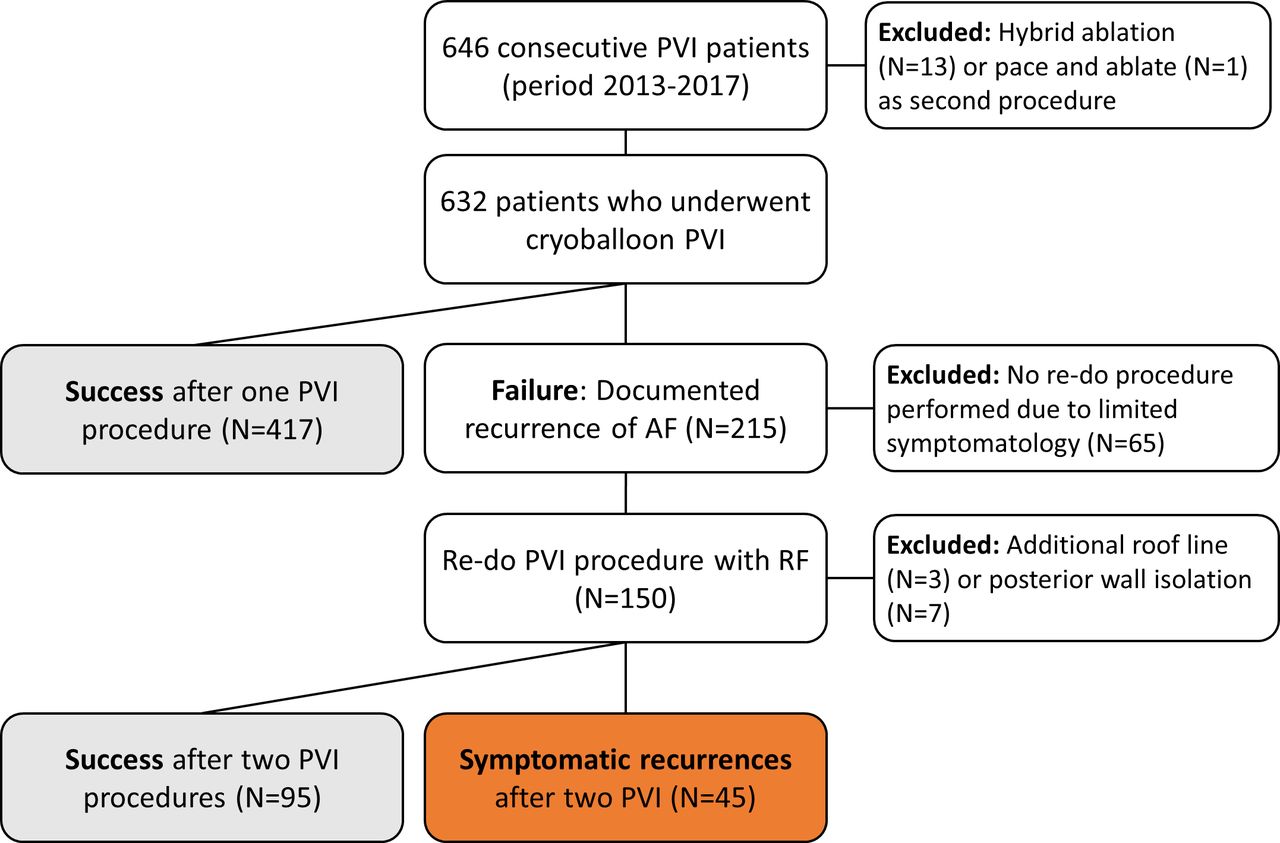
Flowchart of patients who underwent rhythm control strategy in the period of 2013–2017 with the start of a cryoballoon procedure. PVI, pulmonary vein isolation.
Index PVI with cryoballoon
The ablation procedure was performed under conscious sedation. Left atrial access was achieved with a single transseptal puncture guided by intracardiac echo and/or fluoroscopy. The target ACT level was >300. The second-generation 28 mm cryoballoon (Artic Front Advance, Cryocath) was used for PVI since 2014. Until 2017, at least two cryothermal applications (lasting 240 s) were delivered to isolate each vein. In 2017, we adopted the approach proposed by Aryana et al. Briefly, the number of cryoapplications was limited to one if time to isolation (TTI) was <60 s. A ‘bonus’ freeze was delivered if a TTI of <60 s was not observed.16 During cryothermal ablation of the right pulmonary veins, diaphragmatic stimulation was performed to avoid phrenic nerve injury. Electrical isolation of the pulmonary veins was evaluated using the circular Achieve mapping catheter (entrance block). Touch-up ablation with either radiofrequency ablation or cryoablation (Freezor Max) was performed in case cryoballoon ablation failed to isolate the PVs.
Redo pulmonary vein ablation procedure
For recurrences of symptomatic AF redo procedures were performed. Following double transseptal puncture mapping was performed with the EnSite Velocity or Precision (Abbott) or Rhythmia HDx (Boston Scientific) or CARTO (Biosense Webster) mapping systems. Mapping of the LA and PVs was performed with multipolar catheters: AFocus, HD Grid (Abbott), Orion catheter (Boston Scientific) or Lasso Nav or Pentaray (Biosense Webster). Ablation was performed with irrigated tip catheters: Tacti-Cath SE (Abbott), Intellanav OI MIFI (Boston Scientific) or Smarttouch (Biosense Webster). Cardioversion was performed before left atrial mapping in case of AF. During the redo procedure, the pulmonary veins were assessed during coronary sinus pacing and gaps were consequently isolated using radiofrequency applications of 35 W (anterior wall) or 30 W (posterior wall) of 60 s.
Study outcomes
Following all PVI procedures (index and redo PVI procedure), patients were seen in the outpatient clinic with ECG and 24 hour Holter monitoring at 3, 6 and 12 months after index procedure. In case of symptoms and absence of AF on ECG an event recorder was performed. If an unplanned hospital visit with AT/AF occurred or an episode of AT/AF lasting more than 30 s was documented or AT/AF was recorded with an event recorder, during the first year of follow-up the procedure was classified as failed PVI. Recurrences occurring in the first 3 months were excluded (blanking period).
Statistical analysis
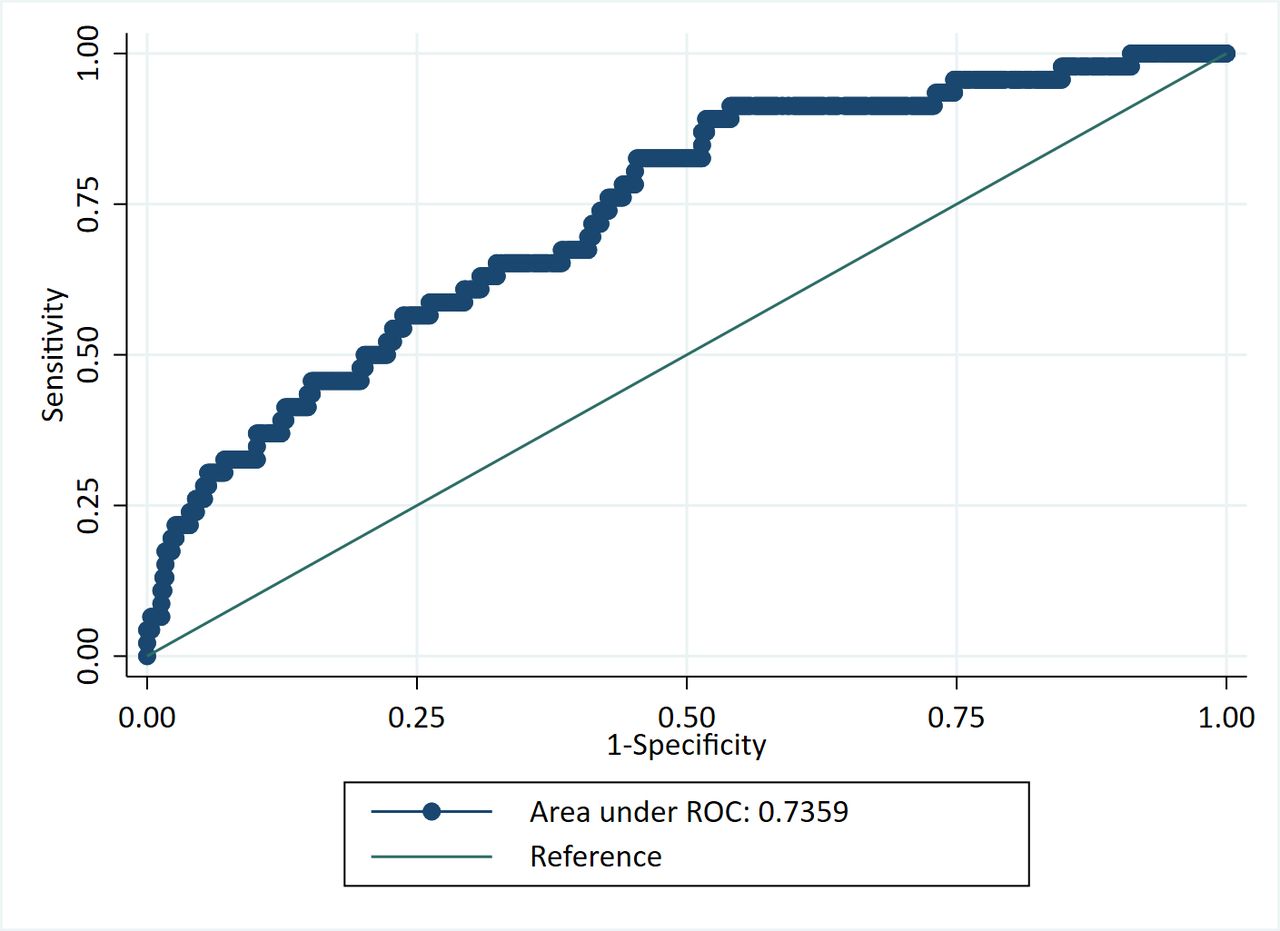
Normally distributed continuous variables were given as mean±SD, skewed data as median with IQR and categorical data as numbers with percentages. The χ2 was used to compare nominal variables. Univariate logistic regression was done to identify risk indicators of AF recurrence after two PVIs. All variables used in the univariate analysis were used in the multivariate model to account for confounding. Area under the curve (and the receiver operator curves) was assessed using multivariable logistic regression. All tests of significance were two sided, with p- values of <0.05 assumed to indicate significance. Data were analysed with Stata/SE V.16.1 (StataCorp, College Station, Texas).
Results
Patient population
Illustrated in figure 1 is that several patients were excluded to assure patients with PVI only were included. After index PVI, 13 patients had a hybrid AF ablation as second procedure, 1 patient opted for pace and ablate and in 65 patients no redo procedure was performed (usually patient preference due to reduction of symptoms after index PVI). Furthermore, 10 patients were additionally excluded from the analysis as left atrial linear lesions in addition to PVI were made during the redo procedure. Therefore, in total 557 patients were used for the present analysis (figure 1). In these 557 patients undergoing index PVI, 31.2% were female, the average age was 59.1 years and 80.4% and 19.6% had paroxysmal and persistent AF, respectively. Following the index PVI, 417 (74.9%) had sinus rhythm during 1-year follow-up and AF recurrence for which redo PVI was performed was observed in 140 (25.1%). At the redo procedure, PV reconnection was observed in 2.1%, 60.9% and 37.0% for respectively 0, 1–2 and >3 of the PVs. The mean number of reconnected veins was 2.2±1.0 per patient. After the redo procedure all PVs were again isolated. Percentages of individual pulmonary veins showing reconduction at redo procedure are shown in figure 2.

Percentages of reconduction found at redo procedure. LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein; RIPV, right inferior pulmonary vein; RSPV, right superior pulmonary vein.
AF recurrence after index or redo PVI
In total 557 patients were included in the analysis. In 140 (25.1%) patients, a redo procedure was performed of which 42 (30%) had a recurrence of AF after the redo procedure and in 3 (2.1%) all pulmonary veins were isolated at redo PVI. Table 1 shows baseline characteristics of the patients who had AF recurrences after two PVIs versus those with sinus rhythm after index or redo PVI. There were no differences in age (59.5±9.1 years vs 58.8±10.1 years, p=0.683) or sex (women 16 (35.6%) vs 158 (30.9%), p=0.506). Patients with recurrences of AF after two procedures more often had persistent (24.4% vs 18.2%) or long-standing persistent AF (4.4% vs 0.6%) and less often paroxysmal AF (71.1% vs 81.3%) (p value for group comparison=0.016) and more severe underlying disease as shown in table 1.
Baseline characteristics
Risk indicators of recurrence after two PVIs
Multivariate logistic regression showed that non-paroxysmal AF (OR 1.08 (95% CI 1.01 to 1.15), estimated glomerular filtration rate (eGFR) (OR 0.96, 95% CI 0.94 to 0.99), bundle branch block (OR 4.17, 95% CI 1.38 to 12.58), heart failure (OR 4.17, 95% CI 1.38 to 12.58) and Left Atrial Volume Index (LAVI) (OR 1.04, 95% CI 1.01 to 1.08) were independently associated with AF recurrence after two PVIs (table 2 and figure 3). The area under the curve (for all variables included in the multivariate model) as represented by receiver operator curve (ROC) is shown for the risk factors in figure 4.

Central figure illustrating potential characteristics of patients in whom a pulmonary vein isolation (PVI) approach alone might be less beneficial. AF, atrial fibrillation; eGFR, estimated glomerular filtration rate; LAVI, Left Atrium Volume Index.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operator curve (ROC) for the multivariable model (including non-paroxysmal AF, estimated glomerular filtration rate, bundle branch block, heart failure, Left Atrium Volume Index which were associated with AF recurrence after two PVIs). AF, atrial fibrillation; PVI, pulmonary veins isolation.
Logistic regression for the outcome of AF recurrence after two PVIs
Discussion
In 557 patients with AF in whom a PVI-only ablation approach is performed (at both the index and the redo procedure), we identified several clinical risk factors associated with AF recurrences. Patients with non-paroxysmal AF, bundle branch block, heart failure and increased LAVI had a higher chance of AF recurrence despite AF ablation procedure targeting only the PVs.
As PVI has evolved into a frontline therapy in patients with AF, identification of patients who will not benefit from a PVI approach is pivotal.17 18 Many patients face moderate long-term outcome after single PVI.4 19 Although ablation technologies are improving PV reconnection remains a common phenomenon.19–22 For this reason, following AF recurrence, the next step is often a redo AF ablation procedure where the PVs are assessed and in case of reconnection conduction gaps are ablated. De Pooter et al demonstrated that many patients can be arrhythmia free following repeat PVI, highlighting the importance of obtaining durable complete PVI.23 This was also observed in the present study.
Nevertheless, as was also shown in the present study, there remains a group of patients in whom AF ablation targeting the PVs only will not be sufficient for maintaining long-term sinus rhythm. The last decades several ablation strategies targeting the atrial substrate have been introduced. These approaches include linear atrial lesions, left atrial appendage (LAA) or/and superior vena cava isolation, ablation of complex fractionated electrograms (CFAE), voltage-based approach, ablating non-pulmonary foci or ganglionated plexi or recently vein of Marshall alcohol ablation.14 15 24 In the Substrate and Trigger Ablation for Reduction of Atrial Fibrillation Trial Part II trial, patients with persistent AF were randomised to either PVI alone (similar to our population) or PVI with addition of CFAE or PVI with addition of additional linear lines (roof and mitral valve isthmus).3 In this trial, there was no difference observed in the rate of recurrent AF in any of the randomised groups.3 Recently, vein of Marshall ablation in combination with LA ablation was compared with LA ablation in patients with persistent AF. Freedom from AF was slightly higher in vein of Marshall treated patients.24 Of note, these trials included patients based on the type of AF (persistent AF). It is likely that some of these patients had only moderate degree of structural remodelling and PV ablation only could have been sufficient. Interestingly, in the electrophysiological substrate ablation in the LA during sinus rhythm (STABLE-SR) trial, it was shown that in non-paroxysmal AF a PVI strategy including cavotricuspid isthmus ablation and targeted low-voltage areas and complex electrogram was equally successful as stepwise linear lesions and defragmentation. Importantly, in the substrate-based ablation group, almost half of the patients had no low voltage and only PVI ablation was performed.25 Future studies are needed to address the question whether ablation based on electroanatomical mapping or preprocedural scar characterisation with cardiac MR could potentially lead to a more tailored ablation and improve outcome.
Preprocedural predictive clinical risk factors may also be helpful to guide patient selection and ablation strategy.1 Ablation beyond the PVs should not be considered in patients with a high likelihood of maintaining sinus rhythm following ablation of only the PVs. A number of risk factors can predict AF recurrence after single PVI: LA size, duration of AF, age of the patient, renal dysfunction and atrial late gadolinium enhancement visualised by MRI.1 These variables are associated with structural abnormalities of the atria predisposing to more persistent form of AF.26 Kosiuk et al observed that a high APPLE Score was associated with more low-voltage areas detected during electroanatomical mapping of the LA.12 The variables found in our study suggest that patients who fail two PVIs had also already progressive disease: non-paroxysmal AF, heart failure and bundle branch block. If clinical success after two PVIs is not achievable for these patients, the question that remains is whether long-term sinus rhythm can be achieved at all or with other ablation strategies. To highlight the different ablation strategies used in populations with advanced disease, it is illustrative to observe the differences in the Catheter Ablation vs Standard Conventional Therapy in Patients with Left Ventricular Dysfunction and Atrial Fibrillation (CASTLE-AF) Study.27 In CASTLE-AF, an extended approach in addition to PVI was chosen in more than half of the patients even for the first procedure. Of the 151 patients randomised to the ablation group, in 74 patients the primary approach was PVI only and in 77 patients the first PVI was already performed with additional linear lines or CFAE.27 Importantly, at the redo procedure, 21 of the 37 patients had a redo of the PVs with additional lines. It is unknown if one approach was superior in this heart failure trial but it illustrates that many different strategies are performed as primary AF ablation approach. Another extensive ablation strategy that could be used as a primary approach in an advanced diseased population is a surgical or hybrid AF ablation.28 For example, for non-paroxysmal AF patients, 3-year follow-up without AF recurrences may reach up to 80%.29 However, data in patients with heart failure are limited and ideally a randomised trial should be conducted to address the discussion which PVI approach is most successful.30 Concluding, it remains controversial in which patient’s substrate ablation outside the pulmonary veins should be performed but selection may be limited to those with non-paroxysmal AF, heart failure and increased LAVI as they have an increased risk for AF recurrence after two PVIs.
Limitations
In the present analysis, we identified a subgroup of patients in whom a PVI-only approach failed. For this purpose, we identified patients who underwent at least two PVI procedures or demonstrated permanent PV isolation after the first procedure. We cannot exclude that even after the second PVI procedure, some of the veins had still no durable PVI and a third PVI procedure would have succeeded. Therefore, one cannot conclude complete PVI even after two PVI procedures. On the other hand, there is ample evidence that with each PVI the likelihood of permanent isolation increases.31 32 Recurrences of AF were monitored by standard outpatient clinic ECG and regular Holter monitoring. It is possible that patients were now classified as successful but long-term monitoring could have led to detection of asymptomatic episodes. Furthermore, more extensive follow-up would have provided greater power to our analyses and allowed us to draw more stringent conclusions on the efficacy of a PVI-only approach. Also, residual confounding may be present in the logistic regression model. To allow a robust model we did adjust for all known relevant comorbidities. There was a selection bias in our cohort as some of our (long standing) patients with persistent AF already underwent a hybrid AF ablation as primary approach and were not included in this paper.28 Lastly, although our analyses showed that non-paroxysmal AF, heart failure, eGFR, bundle branch block and increased LAVI are associated with a significantly higher risk of failure after a PVI-only approach, the predictive strength of these variables individually is modest.
Conclusion
Several clinical risk factors were identified to be associated with AF recurrence after two PVIs. These factors suggest that these patients have advanced underlying conditions. This may be used in clinical practice to identify patients in whom a PVI-only strategy may not be enough. Additional AF ablation beyond the PVI may be considered in these patients; however, further research on optimal ablation strategy in these patients is warranted.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon a reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Dutch law allows the use of electronic healthcare records for research purposes under certain conditions. According to this legislation, neither obtaining informed consent from patients nor approval by a medical ethics committee is obligatory for this type of observational studies containing no directly identifiable data (Dutch Civil Law, Article 7:458).
References
Footnotes
Contributors BM, YB and MR designed the study and are responsible for the overall content as guarantor and thereby accept full responsibility for the finished work and the conduct of the study, including access to the data. BM and YB drafted the manuscript. BM performed all statistical analyses. All authors provided substantial contributions to data interpretation and critical revisions and all authors approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.