Article Text

Abstract
Background Coronary artery calcium (CAC) identified on non-gated CT scan of the chest is predictive of major adverse cardiac events (MACE) in multiple studies with guidelines therefore recommending the routine reporting of incidental CAC. These studies have been limited however to the outpatient setting. We aimed to determine the prognostic utility of incidentally identified CAC on CT scan of the chest among hospital inpatients.
Methods and results Consecutive patients (n=740) referred for inpatient non-contrast CT scan of the chest at a tertiary referral hospital (January 2011 to March 2017) were included (n=280) if they had no known history of coronary artery disease, active malignancy or died within 30 days of admission. Scans were assessed for the presence of CAC by visual assessment and quantified by Agatston scoring. Median age was 69 years (IQR: 54–82) and 51% were male with a median CAC score of 7 (IQR 0–205). MACE occurred in 140 (50%) patients at 3.5 years median follow-up including 98 deaths. Half of all events occurred within 18 months. Visible CAC was associated with increased MACE (HR) 6.0 (95% CI: 3.7 to 9.7) compared with patients with no visible CAC. This finding persisted after adjusting for cardiovascular risk factors HR 2.4 (95% CI: 1.3 to 4.3) and with both absolute CAC score and CAC score ≥50th percentile.
Conclusion Incidental CAC identified on CT scan of the chest among hospital inpatients provides prognostic information that is independent of cardiovascular risk factors. These patients may benefit from aggressive risk factor modification given the high event rate in the short term.
- coronary artery disease
- multidetector CT
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Coronary artery calcium (CAC) is an established predictor of future cardiovascular events. To date, studies have evaluated the prognostic role of CAC scoring on non-gated non-contrast CT scan of the chest only in the outpatient setting.
What does this study add?
Our work is the first study to assess the prognostic role of incidentally identified CAC in determining major adverse cardiac event (MACE) among hospital inpatients without a history of coronary artery disease. Simple identification of visible CAC in this cohort was an independent predictor of MACE, beyond 30 days post discharge from hospital.
How might this impact on clinical practice?
Simple visual assessment of the CAC on non-gated CT scan of the chest in hospital inpatients provides independent prognostic information beyond traditional cardiovascular risk factors. This may provide an opportunity to identify patients who may benefit from aggressive risk factors modification.
Introduction
Coronary artery calcium (CAC) is an established predictor of future cardiovascular events.1–4 The relative risk posed by CAC scoring further improves risk stratification by traditional risk factor calculators including the Framingham risk score.5 6 Furthermore, data from the Multi-Ethnic Study of Atherosclerosis (MESA) demonstrated CAC has a net reclassification improvement of 25% compared with traditional risk assessment for predicting major adverse cardiac events (MACE).7 The finding of zero calcium score has very high negative predictive value with a 10-year MACE risk of 1.1%.8
Traditionally, CAC has been identified using ECG-gated CT scan. However, CAC can be detected on a non-contrast, non-gated CT scan of the chest and is known to be under-reported despite being in the field of view and having the potential ability to identify patients at risk who could benefit from risk factor control and improve primary prevention of coronary events.9 Various methods have been examined for optimal CAC scoring on non-gated CT scan, with a meta-analysis demonstrating that a higher CAC score on non-gated CT scan of the chest is associated with an increased risk of MACE and does not overestimate the CAC score.10 11 Accordingly, recent published guidelines recommend routine reporting of coronary calcium on such scans.12
To date, studies have evaluated the prognostic role of CAC scoring on non-gated non-contrast CT scan of the chest only in the outpatient setting. The purpose of this study was to determine the medium-term prognostic value of incidentally identified CAC for predicting MACE among hospital inpatients without a history of coronary artery disease (CAD) undergoing CT scan of the chest who were discharged alive beyond 30 days.
Methods
Patients who underwent non-contrast, non-gated CT scan of the chest between January 2011 and March 2017 as an inpatient of a tertiary referral hospital (Concord Repatriation General Hospital, Sydney, Australia) were retrospectively identified. Exclusion criteria included patients with a history of known CAD and those that died during the index admission or within 30 days of discharge. Active malignancy was an additional exclusion criterion because of limited survival in these patients. The index CT scan was used in cases where patients underwent multiple CT scans. The study complies with the 1975 Declaration of Helsinki.
Baseline demographic and clinical data were obtained using electronic medical records (PowerChart, Cerner, USA). Subsequent hospital admissions, vital status and cause of death data were obtained through data linkage performed by the Centre for Health Record Linkage ((CHeReL), Sydney, Australia). In summary, CHeReL performed the population linkage of the study cohort with the NSW Admitted Patient Data Collection Registry and the NSW Registry of Births, Deaths and Marriages registrations databases. The primary outcome was MACE, a composite endpoint including all-cause death, non-fatal myocardial infarction, unstable angina requiring revascularisation, congestive cardiac failure and cerebrovascular events. Each admission diagnosis and cause of death code was based on the International Classification of Disease, Tenth Revision Australian Modification.
CT scan data analysis
CT scans were acquired on a Definition DS 64-slice or Definition AS+128-slice scanner (Siemens, Germany). All CT scans were non-contrast studies for non-cardiac indications. We used two methods to assess CAC. First, the presence of CAC was assessed by visual assessment and recorded as visible or not visible. Second, CAC was quantified by Agatston scoring using dedicated software (syngo.via, Siemens, Germany). Calcified lesions were identified based on a minimum threshold of 130 Hounsfield units. The Agatston Score is the product of the calcified area by the weighting factor, which is defined by the peak density.13 The results are expressed as both absolute values and the estimated calcium score percentile based on age, gender and race as reported in MESA.14 Patients were categorised into CAC percentile groups: <50th percentile and ≥50th percentile and groups according to the following score: 0, 1–100, 101–400 and >400. CT scans were analysed by a single observer (CY) blinded to the clinical outcomes. A random selection of 30 patients was identified for secondary reads by an experienced Cardia CT reader (CN) to determine interobserver variability.
Statistical analysis
Statistical analyses were performed on SPSS V.24 (IBM, USA). Continuous data are described as median and IQR if not normally distributed or mean±SD otherwise. Categorical data are reported as percentages. Continuous variables were compared using independent sample t-test and categorical variables using χ2 test. Kaplan-Meier analysis was used to estimate event-free survival and compared using the log-rank test. A Cox proportional hazards model was used to analyse time to a primary event and estimate HRs between age and sex-specific adjusted CAC score categories and groups by CAC score after adjusting for cardiovascular risk factors (age, sex, smoking history, hypertension, chronic kidney disease and diabetes). The proportional hazards assumption was checked with log-minus-log plots. Cohen’s kappa (κ) was used to assess interobserver agreement of categorical data and a two-way random intraclass correlation for continuous data. We defined a two-sided p value<0.05 as statistically significant.
Results
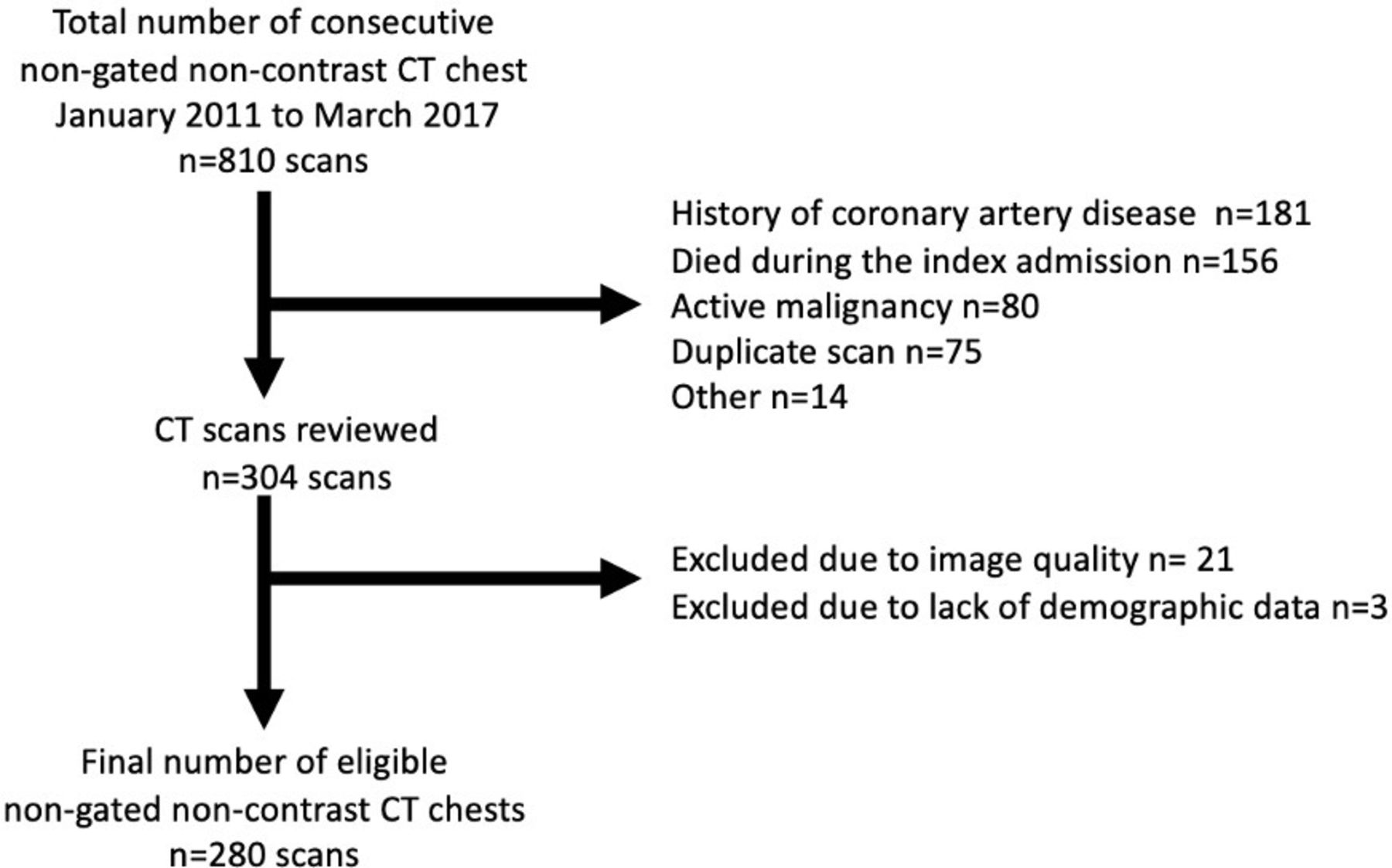
A total of 810 inpatient non-contrast non-gated CT scans of the chest were performed on 740 patients between January 2011 and March 2017. Of these, 530 scans were excluded, with most excluded due to a known history of coronary heart disease (n=181), death during index admission (n=156) and malignancy (n=80) (figure 1). A total of 280 scans were included in the analysis. The primary indications for the CT scan of the chest were chronic obstructive pulmonary disease (n=56), lung nodule assessment (n=49) and interstitial lung disease (n=36).
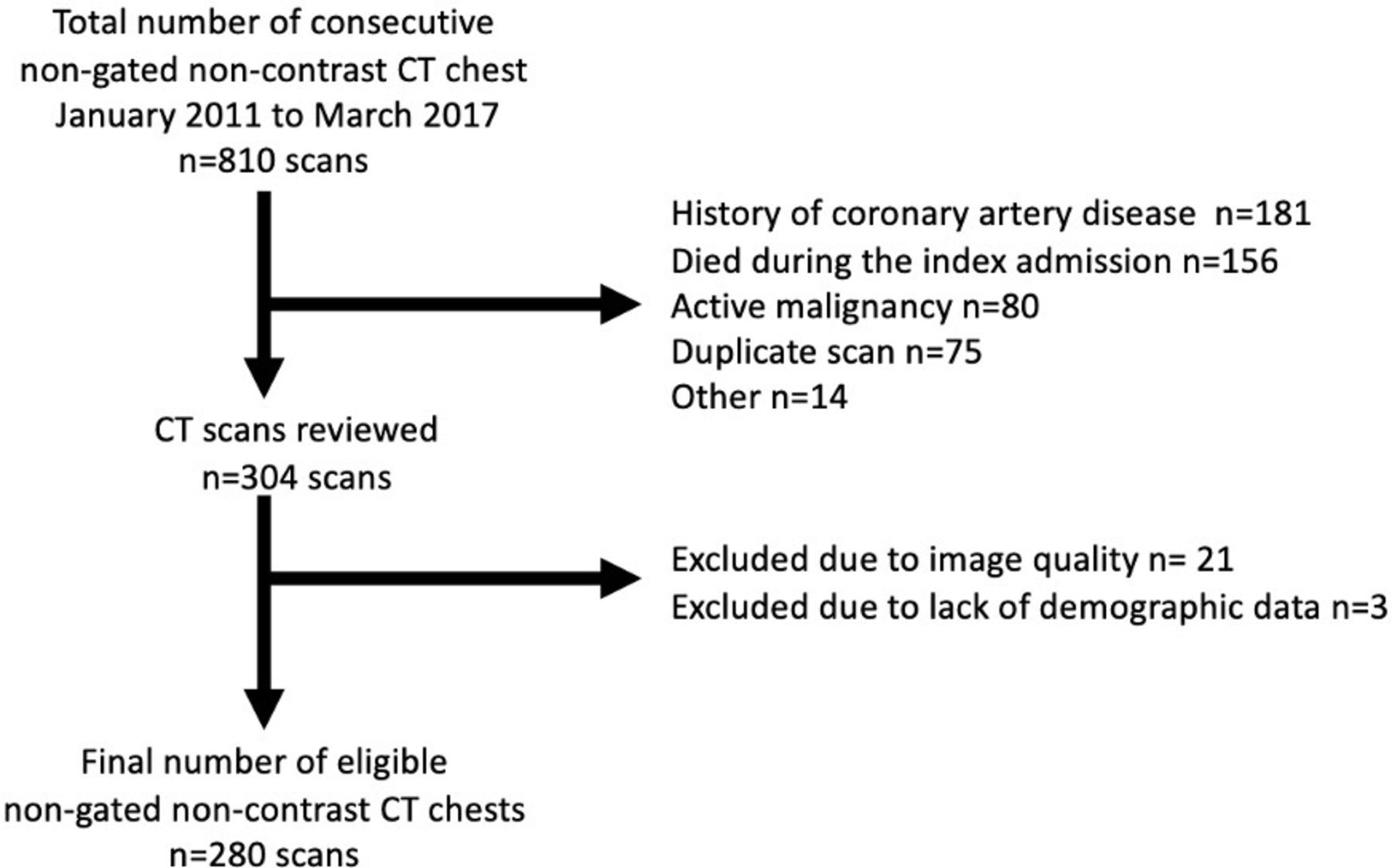
Flowchart showing selection of eligible patient in this study.
Baseline characteristics of the overall cohort are shown in table 1. The median age of the study patients was 69 years (IQR: 54–82) with 51% male. Visible CAC was identified in 172 (61%) of the patients. Patients with visible CAC were older and had a higher prevalence of diabetes, hypertension and hyperlipidaemia. However, among the 65 patients who had no known cardiovascular risk factors, 17 (26%) patients had visible CAC. Conversely, among patients with two or more risk factors, 23 (17%) had no visible CAC.
Baseline clinical characteristics stratified by the presence of visible CAC
On quantitative assessment, the cohort’s overall median CAC score was 7 (IQR 0–205). There were 120 (43%) patients with a CAC score of 0, 109 (39%) with a CAC score of 1–399 and 51 (18%) with a CAC score ≥400. There were 12 (7%) patients who had a CAC score of 0 despite there being visible calcium on visual assessment, consistent with prior studies.15 16 Using MESA-based percentiles correcting for age, sex and race, 187 (67%) patients had a CAC <50th percentile and 93 (33%) patients had a CAC ≥ 50th percentile. Despite this adjustment, older patients (≥median age of 69 years) were still more likely to have a CAC score ≥ 50th percentile compared with younger patients (62 (44%) vs 31 (22%), p<0.001).
Outcomes
Median follow-up was 3.5 years (IQR 2.0–5.5). There were 140 MACE events (50%), with a median time to MACE of 1.5 years (IQR 0.6–3.2 years) including 98 deaths (35%), which occurred at a mean age of 77±14 years (table 2). Of the 98 deaths, 30 patients (31%) suffered cardiovascular death, with heart failure being the most common cause of cardiovascular death (n=10, 33%). Respiratory death was the most common cause of non-cardiovascular mortality (n=23; 23%) and causes included pneumonia, respiratory failure and pulmonary embolism. The cause of death was unclassified in 20 cases due to lack of death certificate information.
Major adverse cardiac events (MACE) and causes of death
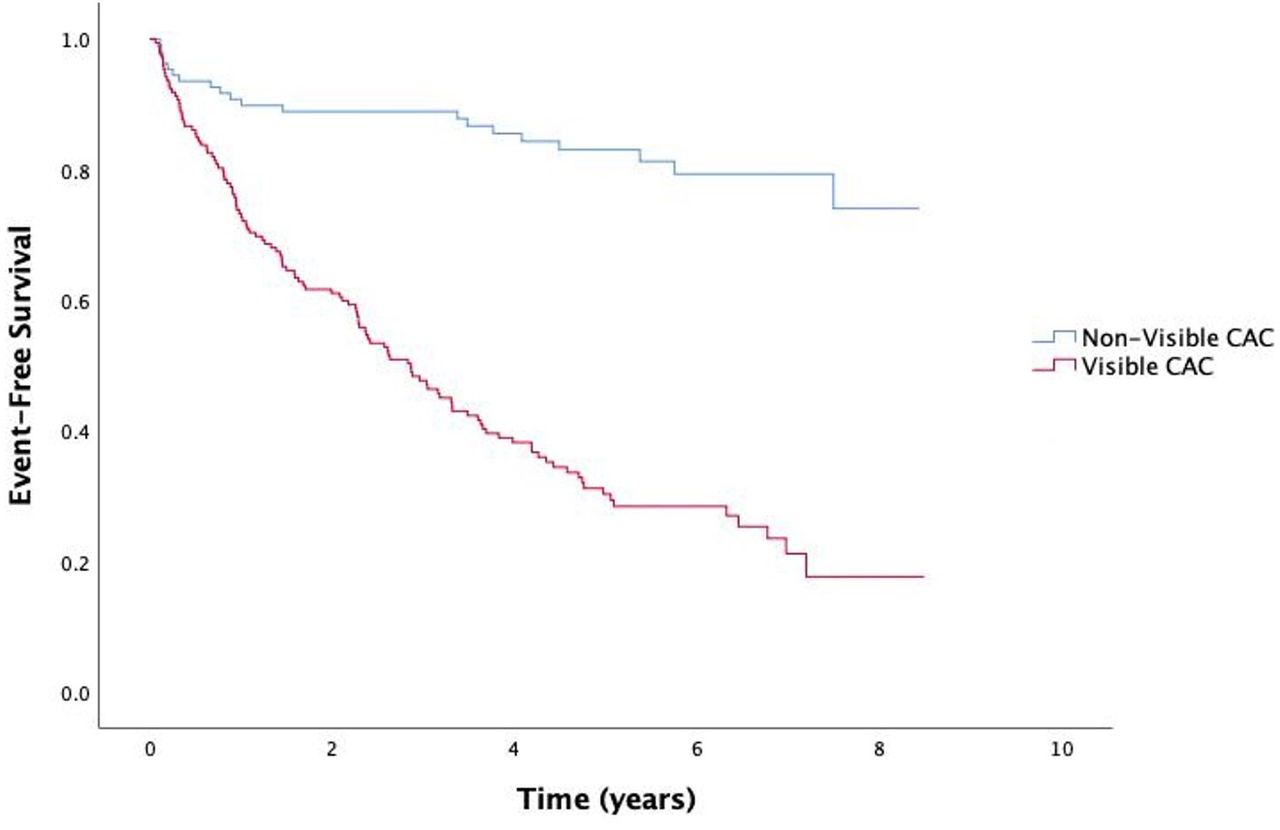
MACE-free survival was significantly higher in patients with no visible CAC compared with those with visible CAC (82% vs 30%, log-rank p<0.001; figure 2). For patients with visible CAC, the unadjusted HR for MACE was 6.0 (95% CI: 3.7 to 9.7, p<0.001) compared with patients with no visible CAC (table 3). After adjusting for age, sex and cardiovascular risk factors, visible CAC was associated with increased risk of MACE compared with non-visible CAC with a HR of 3.2 (95% CI: 1.8 to 5.6, p<0.001).

Kaplan-Meier graph for visible versus non-visible coronary artery calcium (CAC).
HRs for MACE based on CAC assessment
When based on CAC score, patients with higher CAC scores had higher risk for MACE (unadjusted HR 1.001, 95% CI: 1.001 to 1.001, p<0.001). When CAC score was divided into groups by scores of 0, 1–100, 101–400 and >400, those in the >400 CAC score group had higher MACE (unadjusted HR 5.01, 95% CI: 3.1 to 8.1, p<0.001).
After adjusting for age, sex and cardiovascular risk factors, CAC score remained predictive of MACE with an adjusted HR of 1.0004 (95% CI: 1.0002 to 1.001, p=0.001) per Agatston unit. The CAC by groups was despite showing a trend for increasing CAC score group had higher risk for MACE, it was only predictive in the >400 CAC group after adjusting for age, sex and cardiovascular risk factors 2.17 (95% CI: 1. 23 to 3.84, p=0.008).
MACE-free survival was significantly higher among patients in the <50th CAC percentile group (60% for patients <50th CAC percentile and 29% for patients ≥50th CAC percentile (log-rank p<0.001, figure 3). The unadjusted HR for MACE was 2.6 (95% CI: 1.9 to 3.7, p<0.001) in the ≥50th CAC percentile group. After adjusting for cardiovascular risk factors, the HR was 1.9 (95% CI: 1.4 to 2.7, p<0.001). For each percentile increase in CAC, the unadjusted HR was 1.01 (95% CI: 1.01 to 1.02, p<0.001) and the adjusted HR was 1.01 (95% CI: 1.01 to 1.02, p<0.001).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier graph for <50th coronary artery calcium (CAC) percentile versus ≥50th CAC percentile.
Interobserver variability of visual CAC on non-gated CT scan of the chest
Among the 30 (11%) scans that were randomly selected for secondary reads, the Cohen’s κ value was 0.85, p<0.001 between observers for assessing visible CAC. Interclass correlation for CAC score was 0.97, p<0.001.
Discussion
We report that among hospitalised inpatients undergoing non-gated CT scan of the chest, both visible CAC and a CAC score ≥50th percentile provide independent prognostic information at medium-term follow-up, with half of the events occurring within 18 months. The simple, pragmatic assessment of visible CAC could potentially identify patients at increased risk of cardiac events before hospital discharge and facilitate commencement of primary prevention therapy.
Prevalence of CAC in non-gated inpatient chest CT
Despite the high prevalence of incidental CAC, it remains under-reported.17 Multiple large outpatient cohorts have shown a prevalence of incidentally visualised CAC of approximately 70%.11 18 There is only one report on incidental CAC prevalence in inpatients cohorts, reporting a prevalence of 63%.19 Our study found a similar prevalence of 61% despite none of our included patients having a known history of CAD. Furthermore, among patients with no cardiac risk factors, just over a quarter (26%) had visible CAC, and conversely, among patients with seemingly increased risk based on traditional risk assessment (two or more cardiac risk factors), 17% had no visible CAC. These findings highlight the ability of CT scan of the chest to restratify patients into high-risk and low-risk groups independent of baseline traditional risk assessment. Additionally, we found that CAC could be assessed reproducibly with excellent interobserver reliability between two readers for both visual CAC and CAC score. This finding emphasises the ease at which simple CAC assessments can be done in non-gated CT scans of the chest.
Prognostic value of CAC in non-gated inpatient chest CT scan
Our results show that visible CAC and ≥50th CAC percentile on non-gated CT scan of the chest are independent predictors of MACE in the medium term among hospital inpatients without a known history of coronary artery disease and remained significant after adjusting for cardiovascular risk factors. The current literature on the prognostic role of CAC in non-gated CT scan of the chest is primarily based on lung cancer screening outpatient scans.11 20–22 These studies have all consistently shown that CAC can be identified on non-gated CT scan of the chest and identification of CAC is associated with poorer cardiovascular outcomes.11 20–22 More recently, Shao et al demonstrated the prognostic utility of visible CAC among all comers presenting for outpatient CT scans of the chest requested by respiratory physicians.15 This has been reaffirmed by Xie et al’s systematic review and meta-analysis.10 The Society of Cardiovascular Computed Tomography/Society of Thoracic Radiology guidelines now support the use of visual assessment of CAC as an alternative to Agatston scoring.12 Our study uniquely involved hospital inpatients, which has not been reported previously. As a result, there was a wider variation in scan indications, such as trauma and foreign bodies (n=25, 9%). We found that CT scan of the chest is still predictive of prognosis in this group of inpatients independent of cardiovascular risk factors. The fact that incidental visible CAC was independently predictive of MACE in an acute inpatient population, with half of the MACE events occurring within 18 months of discharge, indicates that intervention to reduce the risk of cardiovascular events may be temporally relevant in these populations.
Limitations
The first limitation of our study is selection bias as patients were primarily referred for non-contrast CT scan of the chest for lung disease. Moreover, a significant number of patients were excluded due to malignancy and death during the index admission. The applicability of the results is therefore limited to similar patients. Second, although non-gated CT scan of the chest was used for calcium scoring, there was excellent interobserver reliability for this method. Third, our study was a single-centre retrospective cohort study with a small sample size, thus leading to underpowering when CAC was divided into ordinal groups. Future studies are needed to prospectively evaluate the prognostic role of incidentally identified CAC on non-gated CT scan of the chest among hospital inpatients.
Conclusion
CAC is frequently observed among hospital inpatients undergoing non-gated CT scan of the chest who otherwise have no known history of CAD. Simple visual assessment of the CAC on non-gated CT scan of the chest in hospital inpatients provides independent prognostic information beyond traditional cardiovascular risk factors. This may provide an opportunity to identify patients who may benefit from aggressive risk factors modification.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was approved by New South Wales Population and Health Services Research Ethics Committee (Reference HREC/18/CIPHS/62) with a waiver for informed consent.
References
Footnotes
Twitter @drchrisyu
Contributors All authors contributed to the manuscript. ACCN assisted with the ethics application. CY, LR and CN performed coronary artery calcium analysis. MA performed data collection.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.