Article Text

Abstract
Objectives Report predictors and the natural course of paravalvular leak (PVL) following implantation of the ACURATE neo transcatheter heart valve (THV).
Background Understanding the mechanisms of PVL may help to improve patient selection, patient outcomes and the design of next-generation THVs.
Methods A total of 30 patients (mean age 81±5 years, 47% women) undergoing transcatheter aortic valve replacement with the ACURATE neo were enrolled in the PREDICT PVL study. The effective regurgitant orifice area (EROA, in mm2) of PVL was assessed by transthoracic and transoesophageal echocardiography before discharge and at 6 months follow-up.
Results PVL was none/trace in 10 (33%), mild in 18 (60%) and moderate in 2 (7%) patients and occurred in distinct locations with largest EROAs in the area of the left coronary cusp and its adjacent commissures. Independent predictors for EROA were implantation depth (r coefficient −1.9 mm2 per mm implantation depth, p=0.01), leaflet calcification (6.2 mm2 per calcification grade, p=0.03) and THV size L (7.6 mm2 more than size S or M, p=0.01). At 6 months follow-up, EROA decreased by 29% from 13.7±9.7 mm2 to 9.5±7.9 mm2 (p<0.01). Patients with smaller EROAs were more likely to be in New York Heart Association class 1 than patients with larger EROAs (p<0.01).
Conclusions PVL occurred predominantly in the region of the left coronary cusp and decreased by 29% during 6 months of follow-up. Our results underscore the importance of adequate patient selection and optimal implantation depth.
- aortic valve disease
- quality of care and outcomes
- transoesophageal
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Recently, transcatheter aortic valve replacement (TAVR) with the self-expanding ACURATE neo transcatheter heart valve (THV) did not meet non-inferiority compared with the balloon-expandable SAPIEN 3 (Edwards Lifesciences, Irvine, California, USA) in terms of early safety and clinical efficacy outcomes. This was mainly driven by a difference in moderate and severe paravalvular leak (PVL).
What does this study add?
The PREDICT PVL study provides detailed insights into the pathophysiology of PVL after TAVR with the ACURATE neo.
How might this impact on clinical practice?
Our results underscore the importance of adequate patient selection and optimal implantation depth and may help to improve patient outcomes. This study will continue to include patients undergoing TAVR with the ACURATE neo 2 THV, allowing direct assessment of the effect of the improved sealing skirt.
Introduction
The occurrence of paravalvular leak (PVL) remains one of the most frequent challenges following transcatheter aortic valve replacement (TAVR). Recent trials and registries have reported mild PVL after implantation of the ACURATE neo (Boston Scientific, Marlborough, Minnesota, USA) transcatheter heart valve (THV) in up to 58% and more than mild PVL in 4%–9% of patients.1–4 In the recently published SCOPE-1 study, TAVR with the self-expanding ACURATE THV neo did not meet non-inferiority compared with the balloon-expandable SAPIEN 3 THV (Edwards Lifesciences, Irvine, California, USA). This was mainly driven by a higher prevalence of moderate or severe PVL.2 However, this THV has also been associated with low postprocedural gradients and very favourable rates of conduction disturbances, strokes and mid-term survival.1 5 6
Therefore, the PREDICT PVL study aimed to investigate the pathophysiology and predictors for PVL after ACURATE neo TAVR. Furthermore, we assessed the natural course of PVL over a 6-month period.
Methods
Patient selection and study design
Between March 2018 and June 2019, patients with severe symptomatic aortic stenosis undergoing TAVR at the Heart Center Lucerne, the tertiary cardiology facility of the central part of Switzerland, were screened for enrolment in the PREDICT PVL study. Exclusion criteria were emergency procedures, bicuspid aortic valves, a pre-existing prosthetic heart valve in aortic position, pre-existing renal insufficiency with a glomerular filtration rates less than 30 mL/min/1.73 m2 and oesophageal diseases including stricture, tumour, perforation, diverticulum and active upper gastrointestinal bleed. Follow-up examinations before discharge (1–6 days after TAVR) and 6 months (±30 days) after TAVR included transoesophageal echocardiography (TEE) and ECG-gated contrast-enhanced multidetector CT.
Transthoracic echocardiography and TEE
Transthoracic echocardiography (TTE) and TEE were performed by two senior cardiologists specialised in echocardiography and cardiac imaging (BWLdB and SS). Philips IE 33 or EPIC7 machines were used (Philips, Best, The Netherlands). PVL was recorded and quantified according to guidelines with standard echocardiographic Doppler methods using mainly colour flow Doppler jet width and extension and pressure half-time. A semi-quantitative score was used for grading (none/trace, mild, moderate, severe).7 In addition, the effective regurgitant orifice areas (EROA, in mm2) of the different jets were measured at the level of the annulus using x-plane guided planimetry in colour Doppler loops. Due to acoustic shadowing and Doppler attenuation from the THV frame, TEE was preferred for measurements of posterior jets whereas TTE was preferred for measurements of anterior jets by protocol.
Multi-slice ECG-gated contrast enhanced CT
CT was performed on a Siemens Definition Flash Dual Source scanner (Siemens, Siemens Medical, Erlangen, Germany). The scan was performed electrocardiogram-triggered in retrospective mode and recorded the phase between 30% and 70% of the RR interval. Reconstructions were performed in systole and diastole. All data were transferred to a postprocessing workstation and analyses were performed using Merlin software (Phoenix-PACS, Freiburg, Germany). The data were analysed using a multiplanar double-oblique reconstruction. A CT scan was obtained before TAVR in all patients to assess the aortic annulus, left ventricular outflow tract (LVOT), leaflets, aortic root and sinotubular junction in all patients. Calcification of the aortic leaflets, the annulus and the LVOT were assessed visually on a scale from 0 to 3 (none, mild, moderate, severe).8 CT of the ACURATE neo THV was performed before discharge and at 6 months follow-up.
TAVR procedure
The ACURATE neo is a supra-annular aortic bioprosthesis consisting of a self-expanding nitinol frame and porcine pericardial leaflets. Due to the relatively low radial force of the inflow portion of the frame, predilatation was performed in almost all patients. The ACURATE neo is the most frequently implanted valve in our centre. The valve size was chosen according to the perimeter of the annulus as measured by CT. To minimise trauma to the annulus and the underlying conduction system, the diameter of the balloon for predilatation was chosen 1–2 mm smaller than the perimeter-derived annular diameter.1 Post-dilatation was only performed in case of relevant aortic regurgitation or relevant transvalvular gradient (>15 mm Hg) with a balloon 1–2 mm smaller than the perimeter-derived annular diameter. The aortic root and the LVOT were visually assessed for calcification and size. The degree of oversizing was calculated as9:

The cover index was defined as10:

Assessed endpoints
We primarily assessed the localisation of the leak, predictors of EROA and change of EROA over a 6 months follow-up. Additionally, clinical endpoints defined according to the updated definitions of the Valve Academic Research Consortium (VARC-2) were evaluated.
Statistics
Data are presented as mean±SD for continuous and as numbers and frequencies for categorical variables. Unpaired and paired continuous variables were compared with the unpaired and paired Student’s t-test. Univariate and multivariable linear regression models were conducted to identify independent predictors of PVL. Variables with a univariate p value <0.1 were included in the multivariable analysis. Statistical analyses were conducted with STATA’s statistical software package (V.13). A p value <0.05 was considered as statistically significant.
Results
A total of 30 patients undergoing TAVR with ACURATE neo were enrolled. In-hospital examinations were performed in all patients. Three patients refused to undergo TEE at 6 months follow-up. Mean age of the study cohort was 81±5 years and 14 (47%) were women. Baseline characteristics and procedural details are displayed in table 1. In-hospital and 30 days outcomes are listed in table 2. Before discharge, the mean transvalvular gradient was 9±3 mm Hg and left ventricular ejection fraction was 66%±10%. There was no stroke and no mortality at 30 days and 6 months follow-up.
Baseline and procedural characteristics
In-hospital and 30 days outcomes
Paravalvular leak
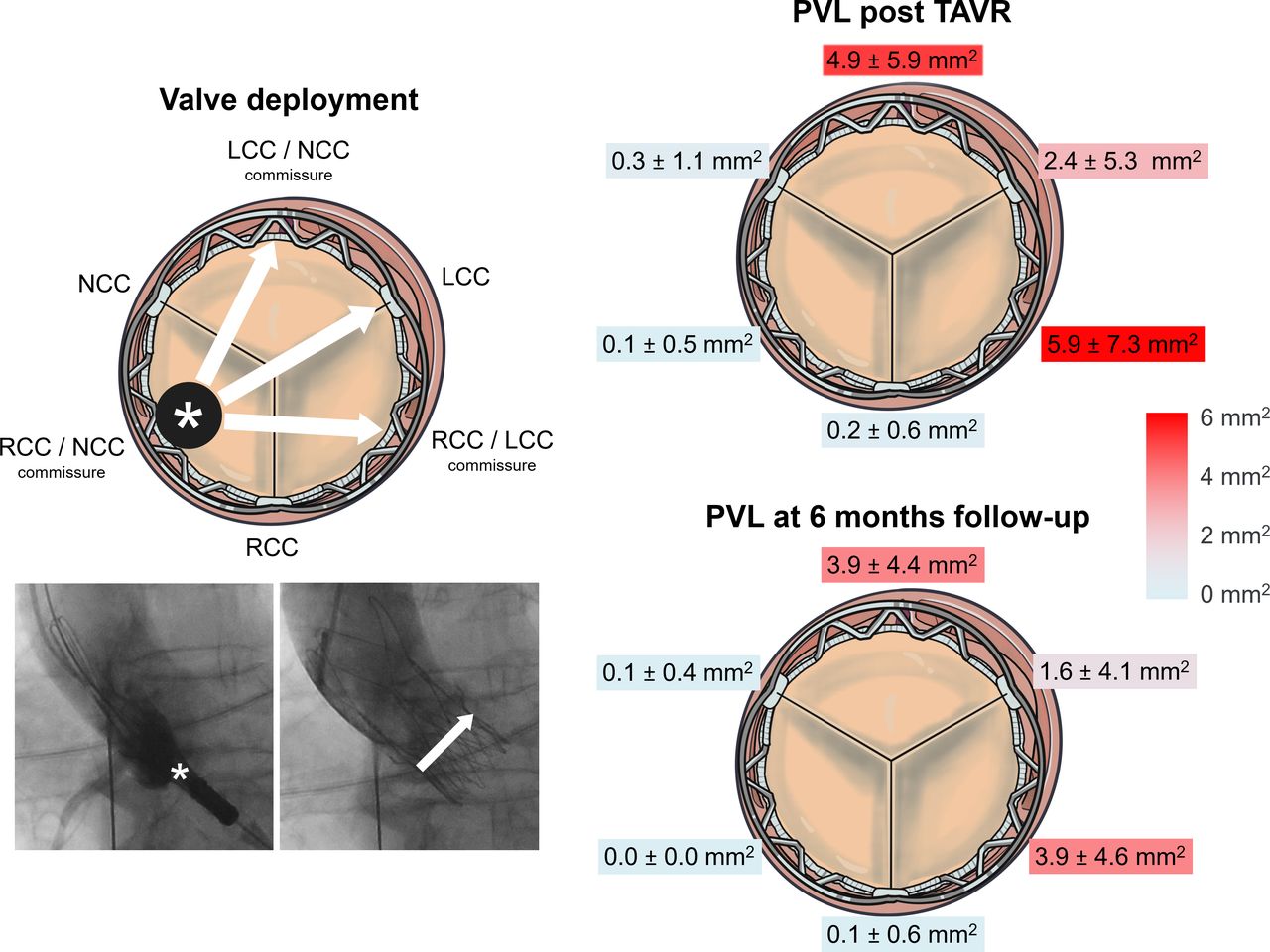
PVL was graded as none in 1 (3%), trace in 9 (30%), mild in 18 (60%) and moderate in 2 patients (7%). None of the patients had severe PVL. More than 95% of PVL EROA was located in the area of the left-coronary cusp (LCC) and its adjacent commissures which is located opposite to the initial position of the delivery catheter and the valve (figure 1). EROA was largest with 5.9 mm²±7.3 mm² between the LCC and right-coronary cusp (RCC) and with 4.9 mm²±5.9 mm² between the LCC and non-coronary cusp (NCC). During follow-up, total EROA decreased by 29% from 13.7±9.7 mm2 to 9.5±77.9 mm2, p<0.01. The localisation and amount of EROA before discharge and at 6 months follow-up is depicted in the figure 1. Figure 2 shows an example of PVL in a patient with significant PVL reduction over time.

Mean EROA in relation to the annular anatomy post-TAVR and at 6 months follow-up. Valve deployment process starts with the device in the outer curvature of the aorta and the THV being positioned in the commissure between the NCC and the RCC (asterisk). The ACURATE neo expands towards the LCC and its adjacent commissures (arrows). PVL occurred predominantly in the region of the most distant cusp the LCC and its adjacent commissures. EROA decreased at 6 months follow-up. EROA, effective regurgitant orifice area; LCC, left-coronary cusp; NCC, non-coronary cusp; PVL, paravalvular leak; RCC, right-coronary cusp; TAVR, transcatheter aortic valve replacement.

Natural course of paravalvular leak (PVL) in a patient with significant PVL reduction over time. Transoesophageal echo images of a patient with moderate PVL before discharge (A) and mild PVL at 6 months follow-up (B).
Predictors of PVL
In a multivariable linear regression model, independent predictors for larger EROA were a shallower implantation depth (r coefficient −1.8 mm2 per mm implantation depth, p=0.02), leaflet calcification (r coefficient 1.1 mm2 per calcification grade, p=0.04) and THV size L (r coefficient 7.6 mm2 more than size S or M, p=0.03) (table 3).
Univariate and multivariable predictors of PVL
Clinical relevance of PVL
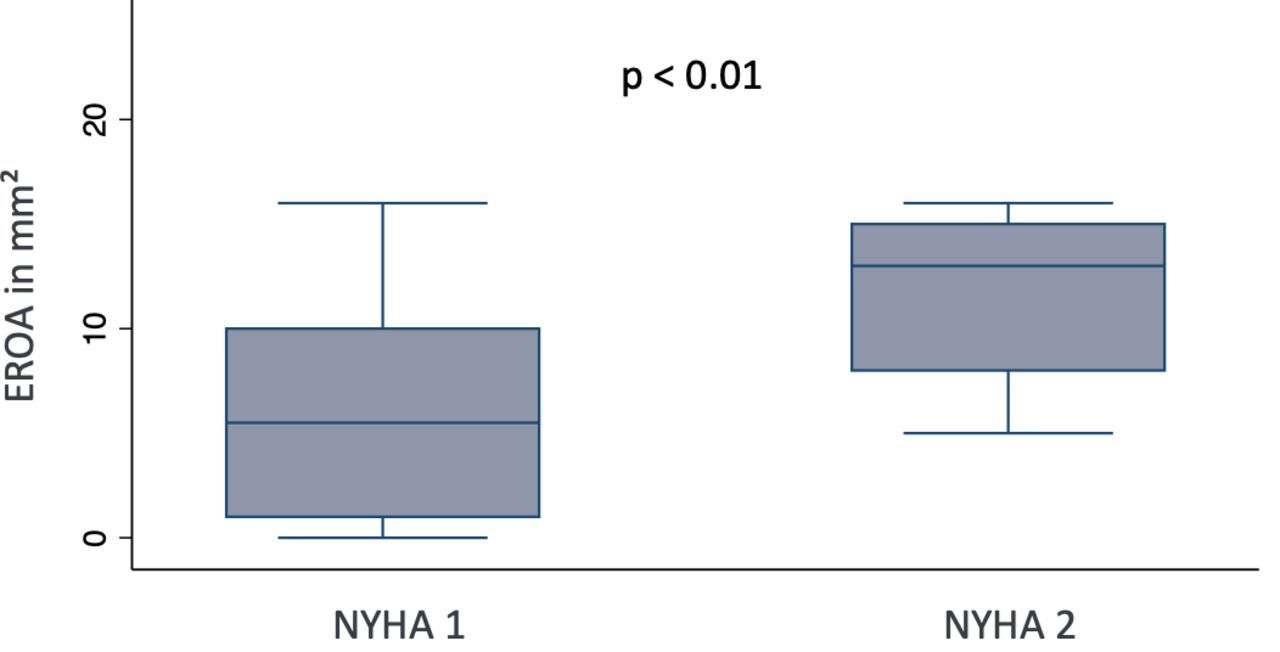
All patients had New York Heart Association (NYHA) class 1 or 2 at 6 months follow-up and there was no mortality and no hospitalisation for heart failure. However, patients with smaller EROAs were more likely to be in NYHA class 1 and patients with larger EROAs were more often in NYHA class 2 (p<0.01)(figure 3).

{kind=link}
{kind=link}
{kind=link}
Clinical importance of PVL: NYHA class and EROA at 6 months follow-up.EROA, effective regurgitant orifice area; NYHA class: New York Heart Association dyspnoea class; PVL: paravalvular leak.
Discussion
Individualising the THV selection accounting for patient and anatomical factors has become standard of care at many sites. The evidence facilitating prediction of the postprocedural results is scarce.11 The ACURATE neo THV has been associated with low rates of conduction disorders, vascular complications and all-cause mortality.5 6 However, PVL has been reported in a substantial proportion of patients treated with this valve. The PREDICT PVL study aimed to identify predictors for PVL and thus to improve patient outcomes. The main findings of the PREDICT PVL study can be summarised as follows: (1) PVL occurred in distinct locations with more than 95% of leaks in the area of the LCC and its adjacent commissures. This finding may be explained by the initial position of the valve and the unique implantation sequence; (2) independent predictors of PVL were implantation depth, ACURATE neo THV size L and leaflet calcification, highlighting the importance of a correct implantation technique and appropriate valve selection; (3) PVL was associated with clinical NYHA class at 6 months follow-up. This finding underscores the importance of PVL for patient’s symptoms; and (4) PVL improved significantly by ~30% during the first 6 months after TAVR.
Localisation of PVL
As the ACURATE neo is positioned in a forward movement, deployment of the valve starts with the device in the outer curvature of the aorta, thus in the commissure between the NCC and the RCC. Therefore, the LCC is the most distant cusp. This may explain why PVL occurred predominantly in the region of the LCC and its adjacent commissures. Furthermore, the long axis of the oval annulus is usually oriented in the same direction. This may also favour the occurrence of PVL. Likewise, Kim and colleagues found that most of PVLs occurred in the region of the LCC and its adjacent commissures after TAVR with the ACURATE neo, however no TEE was used for detailed assessment of PVL.4
Importance of a correct initial position
This is the first study to show that implantation depth is one of the most important predictors for PVL in patients undergoing ACURATE neo TAVR. At the beginning of the implantation sequence, the proximal end of the stent holder is positioned 7 mm below the annulus using a forward movement. Once knob 1 has been turned and the upper crown has been opened, the frame flairs and repositioning becomes difficult, if not impossible. Maintaining tension on the delivery system and ensuring that the system remains in its target position during the whole implantation sequence helps to avoid an upward movement of the THV.
Balancing PVL and trauma to the conduction system
The ACURATE neo is a second-generation device with design features to minimise trauma to the conduction system. Indeed, this valve has been associated with a very low rate of new conduction disorders.1 5 However, balancing PVL and trauma to the conduction system remains a challenge for all THV devices. Our data identified the use of the large (L) ACURATE neo to be an independent predictor for PVL. Most likely, this may be explained by the lower radial force of the L compared with the medium (M) and small (S) valve. Potentially this interesting finding can help to improve future iterations of the ACURATE neo. Our findings indicate that when treating patients with large annuli (perimeter >80 mm) and heavily calcified leaflets, another valve with more radial force such as a Lotus valve (Boston Scientific), a SAPIEN 3 (Edwards Lifesciences) or an Evolut R (Medtronic, Fridley, Minnesota, USA) may result in better sealing.
Calcification as a risk factor for PVL
Finally, leaflet calcifications predicted PVL in our study. As shown by others for different THV types, extensive calcifications of the leaflets or the annulus may result in incomplete sealing and malapposition of the frame.8 12 On the other hand, the implantation of the ACURATE neo in heavily calcified anatomies appears to be safe with a low risk for annular rupture.3 As stated earlier, the ACURATE neo may not be the first choice in heavily calcified valves that have large sinuses of valsalvae and no calcification extending into the left-ventricular outflow tract. The ACURATE neo 2 is currently in the process of receiving Conformite Europeenne mark and the US Food and Drug Administration approval study is enrolling patients. This valve features an improved external sealing skirt that may result in better sealing and a reduction in PVL. The PREDICT PVL study will enrol a second cohort of patients who will be treated with ACURATE neo 2 and we will be able to directly assess the effect of the new sealing skirt.
Improvement of PVL over time
We observed that PVL improved by approximately 30% over time. We believe there are two possible explanations for this. The nitinol stent of the ACURATE neo may further expand resulting in better apposition over time. Concurrently, endothelialisation of the frame may improve sealing. In a previous study from our group analysing PVL after implantation of the self-expanding CoreValve (Medtronic), we found that PVL decreased by 45% at 1-year follow-up.13
Limitations
Various techniques and grading schemes have been proposed to quantify the severity of PVL.14 15 None of them was validated so far. However, we assessed PVL by planimetry combining TEE and TTE assessments to avoid potential underestimation of PVL. Finally, patient number was small and the study was not powered to identify subgroups of patients who are more likely to improve their PVL over time. Nevertheless, detailed analysis with TEE provided deep insights for understanding PVL.
Conclusions
The PREDICT PVL study identified three independent predictors for PVL. According to our findings, initial positioning and maintenance of this position during the implantation sequence is key to achieve an optimal implantation depth. THV selection in patients with heavily calcified aortic valves and larger annuli needs to be well balanced. Finally, PVL was more in patients receiving the L valve, which in its current iteration has less radial force than the S or M valve.
Acknowledgments
We would like to thank Patrick Toggweiler for help with preparation of the first figure.
References
Footnotes
Contributors Conception and design or analysis and interpretation of data, or both: MB, ST. Drafting of the manuscript or revising it critically for important intellectual content: MB, BDB, SFS, MW, FM, AA-T, MB, FC, RK, ST. Final approval of the manuscript submitted: all authors.
Funding This study was supported by an institutional research grant from Boston Scientific.
Competing interests SFS is a consultant for Alnylam, Astra Zeneca and Pfizer. RK has received institutional grants from Abbott, Biosense-Webster, Biotronik, Boston Scientific, Medtronic and SIS Medical. ST is a consultant and proctor for Boston Scientific, Abbott and New Valve Technology, has received institutional research grants from Boston Scientific and Fumedica and is holding equity in Hi-D Imaging.
Patient consent for publication Not required.
Ethics approval The study complies with the Declaration of Helsinki. The PREDICT PVL study was approved by the local ethics committee (Ethikkommission Nordwest- und Zentralschweiz, Project ID 2018-00038). All patients provided written informed consent for the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data and study protocol are available upon reasonable request to the corresponding author Dr. med Stefan Toggweiler.