Article Text

Abstract
Objective To conduct a large-scale, single-centre retrospective cohort study to understand the impact of prior percutaneous coronary intervention (PCI) on long-term survival of patients who then undergo coronary artery bypass graft (CABG).
Methods Between 1999 and 2017, a total of 11 332 patients underwent CABG at a hospital in the UK. The patients were stratified into those who received PCI (n=1090) or no PCI (n=10 242) prior to CABG. A total of 1058 patients from each group were matched using propensity score matching. Kaplan-Meier estimates were used to assess risk-adjusted survival in patients with prior PCI. Cox proportional hazards (CoxPH) model was then used to assess the effect of prior PCI and other variables in patients undergoing CABG.
Results The immediate postoperative outcome showed no difference in number of grafts per patients, blood transfusion, hospital stay or 30 days mortality between the groups. There was no significant difference in 5 years (90.8% vs 87.9), 10-year (76.5% vs 74.6%) and 15-year (64.4% vs 64.7%) survival between the non-PCI versus PCI groups. The Cox proportional hazards model further supports the null hypothesis as the PCI variable was found to be non-significant (CoxPH=1.03, p=0.75, CI=0.87–1.22) implying there was no difference in hazard of death for CABG patients with or without previous PCI. However, the model did yield information on the covariates that do affect the hazard of death.
Conclusion There is no difference in 5-year, 10-year and 15-year survival between patients undergoing CABG with or without prior PCI. However, certain patient, preoperative and intraoperative risk factors were identified with high hazard of death which needs to be investigated further.
- cardiac surgery
- cardiopulmonary bypass
- surgery-coronary bypass
- coronary artery disease
- coronary stenting
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- cardiac surgery
- cardiopulmonary bypass
- surgery-coronary bypass
- coronary artery disease
- coronary stenting
Key questions
What is already known about this subject?
Percutaneous coronary intervention (PCI) is the intervention of choice for treating most single vessel diseases, however, coronary artery bypass graft (CABG) is superior for patients with complex multivessel disease and diabetes.
PCI stents have been documented to cause local inflammatory changes, thus, patients with PCI are at risk of restenosis for which CABG is often conducted.
However, there is heterogeneity in current literature about the outcome in patients with prior PCI that undergo CABG.
What does this study add?
This single-centre large retrospective cohort study supports the finding that prior PCI has no impact on 5-year, 10-year and 15-year survival compared with patients without prior PCI.
However, we have discovered certain risk factors that are associated with prior PCI which requires further investigation.
How might this impact on clinical practice?
Our finding is reassuring for patients, allowing clinicians to offer CABG as an alternative revascularisation intervention in these cohort of patients.
Introduction
An estimated 10% of the population in the UK presently live with cardiovascular disease of which 66 000 deaths are attributed to coronary heart disease (CHD).1 When medical management is unsatisfactory in alleviating the ischaemic symptoms, surgical options are considered. Coronary artery bypass graft (CABG) has remained the gold-standard surgical intervention. CABG involves the use of a vascular conduit, commonly the saphenous vein, as a graft. Although it is becoming increasingly common to use arterial conduits such as the internal mammary artery as studies have found that long-term patency rate with arterial grafts are higher.2–4 CABG has been demonstrated to be a highly effective coronary reperfusion strategy for symptom relief of severe angina as well as reducing mortality in this cohort of patients.5 However, CABG is not a cure for CHD as it does not stop disease progression and the grafts can calcify with restenosis occurring if lifestyle changes are not made. Furthermore, being highly invasive, CABG also carries risks of myocardial infarction, stroke, arrhythmias and death.6
The advent of percutaneous coronary intervention (PCI) has advanced the survival of patients with CHD along with reducing the need for CABG.7 PCI involves percutaneous access, under local anaesthetic, of the femoral, radial or brachial artery to conduct wire guided inflation of an angioplasty balloon.8 This compresses the plaque and reopens the vessel, followed by stent deployment to maintain vessel patency.9
Unfortunately, the stents are at risk of restenosis through fibrocellular proliferation triggered by the denuded vascular endothelium, leading to a 17%–41% restenosis rate with bare metal stents. In-stent restenosis has been reduced to <10% with the introduction of drug-eluting stents (DES),10 which release drugs to inhibit local cellular proliferation.11
There are multiple reasons why prior PCI could lead to worse surgical outcomes. Coronary stenting can induce chronic histopathological changes to the vascular endothelium: multiple imaging and histological studies have reported chronic inflammation with endothelial dysfunction.12 This is associated with potential induction of neointimal atherosclerosis inside bare and DES, increasing the risk of in-stent thrombosis or restenosis.13 In addition, prior PCI can also increase the technical difficulty of the surgery, including limiting the number of distal anastomoses grafted.14 These changes complicate outcomes and the efficacy of repeat revascularisation.
Numerous literatures exist that compare the efficacy of PCI against CABG. Comparison of mortality and morbidity has frequently been drawn between PCI and CABG. PCI is the ideal revascularisation strategy in a single vessel disease although CABG is the superior intervention for multi-vessel disease and diabetics15 16; longer survival and lower rates of major postoperative cardiovascular complications are observed in this group.17 18
At present, many patients who had a prior PCI require repeat revascularisation, due to restenosis or progression of coronary disease elsewhere in the coronary circulation, even with DES, are undergoing CABG.19 Initial PCI is found to have significantly higher rates of repeat revascularisation (25.9%) in comparison to initial CABG (13.7%).20 Despite this, numerous studies have reported there is no difference in short to mid-term survival.14 However, the adverse effect on long-term survival is not effectively established. There is incongruence in the results found across studies that have been conducted looking at long term follow-up. Some long-term studies found having multiple previous PCI increases major adverse cardiac outcomes after CABG21 22 while other studies conclude prior PCI has no significant effect on long term survival post-CABG.23
Therefore, a large-scale study needs to be conducted to effectively establish the impact of prior PCI on long-term survival of patients who then undergo CABG.
Aim
To conduct a large-scale retrospective cohort study to understand the impact of prior PCI on long-term survival of patients who then undergo CABG.
Methodology
Data collection
We conducted a retrospective cohort study consisting of 11 332 patients who underwent isolated CABG from 1999 to 2017 at the Blackpool Victoria Hospital. Isolated CABG is defined as having no other simultaneous cardiac intervention performed during the operation.
These patients were categorised into two groups of either prior PCI (n=1090) or no PCI (n=10 242). PCI includes balloon angioplasty followed with stent insertion, however, patients who did not require stent insertion following balloon angioplasty were not included in this group. Elective, urgent and emergency cases were included. However, we excluded patients who underwent subsequent CABG due to unsuccessful PCI, patients undergoing PCI and CABG in the same admission and patients who had concurrent cardiac surgery apart from CABG, for example, valve repair or replacement. One further patient with misrecorded dates implying death prior to surgery was also excluded.
Data were extracted from the hospital database validated for National Institute for Cardiovascular Research Outcomes (NICOR) database.24 The NICOR database contains clinical data of cardiovascular patients across different hospitals in the UK, including Blackpool Victoria Hospital, and is updated annually. We accessed the NICOR database with the dendrite clinical systems; the information collection system. The NICOR database provides extensive information detailing patient demographics with risk factors, operative and postoperative outcomes including hospital stay, morbidity and mortality. Long-term survival was obtained from National Health Service strategic tracing service and was defined as patients living 15 years after surgery, without further coronary surgical interventions. Information regarding patient demographic are presented in table 1.
Statistical analysis
The data were analysed by the research statistician based within Blackpool Victoria hospital’s Clinical Research Centre and took two main approaches: first, propensity matching was used to create a matched data set of 2116 patients (previous PCI, n=1058 and no previous PCI, n=1058) such that preoperative patient characteristics were balanced across the two groups and Kaplan-Meier estimates of long-term survival could then be compared with minimal bias from confounding patient attributes. Matching was performed with MatchIt package in R,25 26 using a greedy method based on propensity scores derived from a logistic regression. No calliper was used. The 16 patient covariates included in the matching process, in table 1, which were chosen as they are preoperative risk factors affecting survival in CHD patients. A log-rank test was used to determine the statistical significance of any difference in the Kaplan-Meier estimate of survival between the PCI and non-PCI groups.
Second, to make most efficient use of the full available data (n=11 332), a Cox Proportional Hazards model was created in order to quantify the effects of a previous PCI, and other preoperative, intraoperative and postoperative variables, on the hazard of death for CABG patients. Stepwise regression was used to determine variables with a statistically significant (p<0.05) effect on the hazard, while retaining the PCI/non-PCI indicator throughout. Summary data in the form of simple percentage survival rates were also calculated for both the matched data set and the full data set and compared using a χ2 test.
Results
Patient demographics and risk factors
Patient demographics including risk factors are presented in table 1. Non-PCI cohort appeared to be younger, male dominant (80%) and more symptomatic (grade 4 CCS score for angina and dyspnoea NYHA), exhibiting more comorbidities. PCI cohort appeared to have significantly greater number of previous MI but better ejection fraction in comparison to the non-PCI cohort. Greater number of patients in the prior PCI group were classed as emergency. Body mass index and Euroscore were similar in both groups.
Following propensity matching, we have identified 1058 patients from each cohort whose preoperative characteristics match sufficiently to give a similar propensity score: the mean distance (probability of prior PCI) was 0.159 in both groups, compared with 0.159 in the PCI group and 0.092 in the non-PCI group before matching (see table 1 and figure 1). The immediate outcomes did not differ in blood loss, chest infection, stroke and in-hospital mortality (1.4% vs 1.5%) between the two matched groups (Table 2). There was minimal variation in the surgical priority between PCI and non-PCI. Up to six distal arteries were grafted in both cohorts.

Histograms of the distributions of propensity scores, before matching (left-hand two) and after matching (right-hand two). ‘Treated’ indicates a prior PCI, ‘control’ had no prior PCI. We see the two right-hand histograms are satisfactorily similar and have mitigated the differences observed in the full data set, as shown by the two left-hand histograms. PCI, percutaneous coronary intervention.
Postoperative complications before matching between PCI versus non-PCI patients
Patient demographics and preoperative characteristics in both the full data set and the reduced, matched data set
Survival
There was no difference in 5 year (90.8% vs 87.9), 10 year (76.5% vs 74.6%) 15 year (64.4% vs 64.7%) survival between the non-PCI vs PCI group (table 3). χ2 tests of homogeneity (for categorical variables) or Mann-Whitney tests (for non-normal continuous variables) revealed that none of these differences are statistically significant. Additionally, long-term survival does not reveal any difference between the groups (64.7% vs 64.4%). This is further supported by the Kaplan-Meier survival curve presented on figure 2. The log-rank test of the null hypothesis that survival in the two groups is the same, giving p=0.9. This implies strongly that there is no evidence of a difference between the two groups.
Comparison of postoperative mortality and survival

Kaplan-Meier plot of survival probabilities for PCI (red) and non-PCI (blue) groups in the matched set. There is no difference in survival between PCI and non-PCI groups here, graphically represented by the Kaplan-Meier curves sitting almost on top of each other. Log-rank test p=0.93. PCI, percutaneous coronary intervention.
Approach 1: propensity matching and Kaplan-Meier estimates
A total of 1058 of the possible 1080 PCI patients were matched to 1058 non-PCI patients from the full database using propensity score matching. The balance of propensity scores, shown in figure 1, is visibly improved after matching (matched group propensity scores shown in the bar charts; ‘treated’ denotes the previous PCI group).
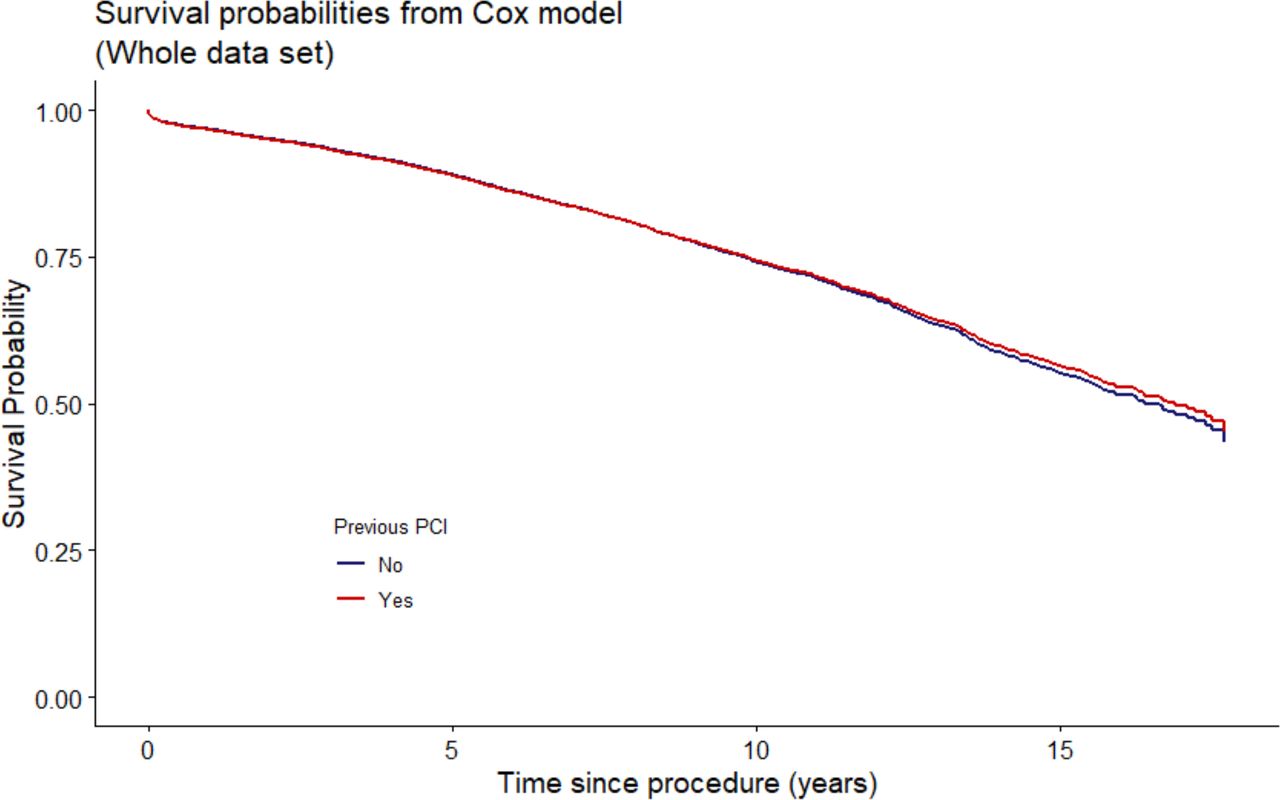
The Cox proportional hazards model further supports the null hypothesis because the PCI variable was found to be non-significant (HR 1.058, p=0.59), even after considering all the available 11000+ patients in the analysis, implying there was no difference in hazard of death for CABG patients with or without previous PCI. Additionally, we also conducted adjusted survival curves using from the Cox proportional hazards model which mirrors the results of Kaplan-Mier Estimates of no difference in survival between PCI versus non-PCI cohort (figure 3). However, the Cox proportional hazards model did yield information on the covariates that do affect the hazard of death. The variables significantly associated with hazard of death are listed in table 4.
{kind=link}
{kind=link}
{kind=link}
Adjusted survival curves calculated from the Cox proportional hazards model described in table 4. An average of the survival estimates for patients in each of the PCI groups is taken using the parameters of the Cox model. Again, we see no difference in survival between groups. PCI, percutaneous coronary intervention.
Covariate estimates produced by Cox pH model of survival, n=6921 (4410 observations not used due to missingness
Discussion
Rise in efficacy of PCI
PCI is thought to be limited mainly to single vessel disease whereas CABG provided better outcomes in complex multivessel CAD. However, since the advancements of DES, it is increasingly common for PCI to be used for multivessel disease with low CAD complexity.27 28 The Synergy Between PCI With TAXUS and Cardiac Surgery (SYNTAX) II trial concluded an enhancement in the efficacy of new generation PCI compared with those in SYNTAX I, demonstrated by reduction in major adverse cardiac and cerebrovascular events: SYNTAX ll 10.6% vs SYNTAX I 17.4%; p=6×10-3 and the need for revascularisation.29 Nevertheless, CABG remains superior to PCI for complex multivessel disease as well as overall reduction in need for repeat revascularisation.19 30 Even with DES, the incidence of repeat revascularisation at 1 year is 12%.31
Survival outcomes in patients with and without prior PCI
Contrasting our results, some studies have reported opposing findings of poor postoperative outcomes in patients with prior PCI, with higher rates of major complication, length of stay and readmission rates.22 32 33 However, at present, there is conflicting evidence in the literature concerning the impact of survival in this cohort of patients: short-term and mid-term mortality reported by some articles are significantly higher in patients with prior PCI, one article reporting 5-year discrepancy in mortality rate among patients with and without prior PCI (PCI=14% vs non-PCI=9%, p=0.12).32 Conversely, recent articles have found no difference in survival between the two groups, therefore stating prior PCI does not negatively impact survival.34 35
In contrast to previous literature, we did not find a significant difference
Although various studies have described survival outcomes, greater than 10-year survival rates have not yet been studied to determine the long-term survival. Our study aims report on survival up to 15 years after the CABG. Our results confirm with the later cluster of studies that found no significant difference in survival at 5, 10 and 15 years between the two groups. However, we acknowledge the smaller sample size of patients at 15 years. While prior PCI was not significantly associated with survival, Cox analysis revealed various patient demographic and preoperative risk factors that were strongly associated with the hazard of death. Some factors must be interpreted with caution as the Cox model only considers all-cause mortality. For example, patients with functioning renal transplant have competing risks of death from infection and renal disease over cardiac reasons, thus in-depth analysis of cause of death is necessary to make concrete statements regarding risk with CABG and transplant.
Limitations
This paper focused was on single-centre, retrospective and matched data. Due to anonymisation of patient data, we are not able to widen the scope of the paper to prove absolute associations of mortality between patient and the intraoperative covariates associated with CABG; this is limited due to lack of information regarding the competing risk of mortality, for example, patients with diabetes might be more likely to have reduced survival due to non-cardiac complications of diabetes rather than a sole cardiac cause. The retrospective design increases susceptibility to selection and observational bias.
Additionally, presence of extraneous variables not factored into the analysis can influence the small discrepancies in the results between the two groups. Our overall sample size was large, however, very few patients in the database had their CABG more than 15 years ago, thus minimising data on 15-year survival. As always, though matching goes some way to imitating a properly randomised controlled trial, we also cannot know whether the decision to perform CABG was related to the knowledge of prior PCI at the time and thus inference should be made with the understanding of the assumption that it was not.
What this study adds
Regardless, this single-centre study has a large sample size, providing a smaller margin of error, with up to 15-year survival period. The range of statistical analysis demonstrates strong acceptance of the null hypothesis. Our results accept the studies that conclude the absence of disparity in long-term survival with prior PCI, adding more clarity to the currently conflicting literature. In addition, the results provide a foundation for future large-scale, prospective multicentre studies to confirm the effect on prior PCI and the association between patient and operative factors on mortality. Finally, the findings are also reassuring for patients who have had prior PCI, undergoing CABG.
Conclusion
Overall, we found no difference in 5-year, 10-year and 15-year survival between patients undergoing CABG with or without prior PCI. Certain patient, preoperative and intraoperative risk factors were identified with high hazard of death which needs to be investigated further.
References
Footnotes
Contributors Planning of the study: PR, RT and MNB. Performance of the analyses: RT. Reporting of the work: PR, RT and MNB. Responsible for the overall content: PR.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as online supplemental information. No additional data are available.