Article Text

Abstract
Aims Long-term oral anticoagulant (LTOAC) reduces ischaemic stroke recurrences. Because of bleeding history, frailty, cognitive impairment, comorbidities or patient refusal, many cannot be discharged from stroke unit on LTOAC. Proportion and outcome of these patients is not well known.
Methods The Warfarin Aspirin Ten-a inhibitor Cerebral infarction and Haemorrhage and atrial fibrillation (AF) prospective registry enrolled consecutive patients with an acute stroke associated with AF. Scales to evaluate stroke severity, disability, functional independence, cognition, risk of fall, ischaemic and haemorrhagic risk stratification were systematically collected at admission, discharge, 3 and 12 months poststroke. The two main 12-month endpoints were death or dependency (modified Rankin Scale >3) and recurrent stroke.
Results Among 400 patients (370 brain infarctions, 30 brain haemorrhages), 274 were discharged on LTOAC, 31 died before discharge and 95 (24%) were not discharge on anticoagulant (frailty, bedridden or demented, EHRA/ESC contraindication to anticoagulant). Death or dependency and recurrent stroke occurred in 19.8% and 9.9%, respectively, in patient on anticoagulant, and 33.5% and 27.2% in those not on anticoagulant (both p<0.001). Patient not anticoagulated at discharge had a 1.6-fold increase in the risk of death or dependency at 12 months (HR 1.65; 95% CI 1.05 to 2.61; p=0.032) and a 2.5-fold increase in the risk of stroke (HR 2.46; 95% CI 1.36 to 4.44; p=0.003).
Conclusions One-fourth of patients with stroke associated with AF are not discharged on anticoagulation and have a dramatic increase in the risk of death or dependency at 12 months as well as recurrent stroke. Alternative treatments should be trialled in these patients.
- stroke
- atrial fibrillation
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Patients admitted to hospital with stroke and atrial fibrillation (AF) (known before or discovered at admission) have a high risk of death, dependency and recurrent stroke.1–4 The treatment of choice to prevent another ischaemic stroke is a long-term oral anticoagulant strategy.5 6 However, many of these patients cannot be on oral anticoagulant because of contraindication to long-term oral anticoagulant, comorbidity, frailty, cognitive impairment, severe walking difficulties with frequent falls and patient refusal.2 The proportion of these patients among patients presenting with a stroke and AF in stroke units is not precisely known.
The risk of death or dependency as well as the risk of recurrent stroke in this group is not well known either. Given that recent alternative treatment to long-term oral anticoagulant has been proposed, such as left atrial appendage closure,7 8 we designed the Warfarin Aspirin Ten-a inhibitor Cerebral infarction and Haemorrhage and AF (WATCH-AF) prospective registry in which we collected consecutive patients admitted with an acute stroke within 72 hours of symptom onset in two busy stroke centres with thorough evaluation regarding risk stratification (CHA2DS2VASc, HAS-BLED, ATRIA scores), stroke severity, disability and functions (NIHSS, Rankin score, independent activity of daily living (IADL), Mini-Mental Status), risk of fall (STRATIFY score) as well as glomerular filtration rate, international normalised ratio (INR) and time in therapeutic range (TTR) while on vitamin K antagonist (VKA) before stroke. Based on these scores, we aimed to evaluate the proportion of patients not on a long-term oral anticoagulant after discharge from the stroke unit and during a 1-year follow-up. We also evaluated the 1-year risk of death or dependency, and of recurrent brain infarction/brain haemorrhage.
Material and methods
Study subjects were consecutive stroke patients with AF admitted to the Bichat Stroke Centre and the Lyon Stroke Unit. Inclusion criteria were ischaemic or haemorrhagical stroke as well as transient ischaemic attack associated with AF hospitalised in both stroke unit within 72 hours of stroke onset. AF could be diagnosed before the stroke, at admission or up to 30 days after the stroke. Inclusions were prospective, consecutive and exhaustive during the accrual period, with verification that all patients with AF have been included. We had no exclusion criteria. Patients were then followed for 1 year. At the time of accrual, these two busy stroke centres had limited access to left atrial appendage closure facilities. Informed consent has been obtained from the subjects (or their legally authorised representative).
Clinical data 1 and 6 months before stroke were recorded, including: prestroke antiarrhythmic and antithrombotic treatments, prestroke AF stroke risk scales (CHA2DS2-VASC, ATRIA haemorrhage score, HAS-BLED) and pre-stroke functional scores (Rankin score evaluating disability, IADL- evaluating functional independence and STRATIFY Risk Assessment Tool, evaluating the risk of fall). In case the patient was not under anticoagulant, the treating physician was interviewed to understand the reasons. If the patient was under VKA, prestroke INR values over the 6 months before were collected.
During the hospitalisation, data collected were: clinical demographics at baseline, medical history, antiarrhythmic and antithrombotic treatment. NIHSS was recorded at baseline. MRI was analysed (or CT, in case MRI was not performed). Other diagnostic tests collected were 12-lead ECG, continuous intrahospital cardiac monitoring (telemetry), Holter-EKG, transthoracic and transoesophageal echography, intracranial and extracranial artery assessment. If ischaemic stroke was diagnosed, the underlying causes were graded according to the ASCOD classification.9 10 In case of haemorrhagic stroke, the aetiology was also recorded, as well as the number and topography of microbleeds. Treatment, including thrombolysis and thrombectomy, other antithrombotic drugs, blood pressure lowering, lipid-lowering and glycaemia lowering drugs, was recorded. NIHSS, modified Rankin Scale (mRS) score, STRATIFY risk assessment tool and MMS were evaluated at discharge.
Based on this assessment and on ESC/EHRA guidelines,11–13 for each patient, two vascular neurologists (EM, EO, CG, PA and Delphi method) discussed the preventive strategy at discharge. We then defined one group on a long-term oral anticoagulant strategy, one other not on a long-term oral anticoagulant strategy for various reasons (eg, patient refusal, contraindication to long-term oral anticoagulant, comorbidity, frailty, patient bedridden or with severe dementia, history of bleeding precluding a long-term oral anticoagulant strategy or adherence to treatment).
Follow-up was performed at 3 and 12 months by a vascular neurologist (EM, EO, CG, LC and PA) in a face-to-face visit or by phone call, in case the patient could not come to the visit. Current place of residency, rehabilitation facilities, visit to healthcare physician and loss of productivity, if applicable, were recorded. Medication was collected as well as vital signs. Barthel Index, NIHSS, mRS, STRATIFY risk assessment tool and MMSE were performed at 3 and 12-month visits.
Main outcomes were death or dependency, and cerebrovascular recurrence (ischaemic or haemorrhagic); other outcomes were cardiac events, revascularisation procedure, major bleeding, aspiration pneumonia, deep venous thrombosis or pulmonary embolism, left atrial appendage closure and death. These outcomes were collected during initial hospitalisation, at 3 months and 12 months
Statistical analysis
Quantitative variables were expressed as means (±SD) in case of normal distribution or median (IQR) otherwise. Qualitative variables were expressed as counts (percentage).
Events rates were estimated at 12 months of follow-up from Kaplan-Meier estimates. Cumulative event curves were constructed using the Kaplan-Meier method. The 12-month event rates were compared according to treatment at discharge using the Cox proportional hazard model. For a given endpoint, deaths that were not included in the endpoint were treated as censoring events. Patients with no information at 12 months were treated as censored cases on the basis of the last follow-up available. Patients dead before discharge were not included in this analysis.
Univariate comparison between the primary outcome and brain infarction or brain haemorrhage and patient characteristics (ie, baseline demographics, risk factors, biological factors, main investigation findings and treatments) was done using the Student’s t-test for continuous and the X2 test for qualitative variables. For variables with skewed distributions, Student’s t-test was performed using log-transformed values.
All factors associated with the primary endpoint and brain infarction or brain haemorrhage in univariate analysis (at nominal p<0.10) were implemented in a stepwise multiple Cox-regression analysis with an entry and removal values set to 0.10. MMS score, ratio E/Eal, left atrium surface and aortic atheroma ≥4 mm were not considered candidate variables due to the high rate of missing data (>25%). Owing to missing data on glucose, haemoglobin A1C, ejection fraction and pulmonary arterial pressure, multiple imputation of missing values by means of chained equations was done (10 imputed data sets were generated with the use of all patient characteristics described below).
For each imputed data, the complete model (ie, containing all significant factors with a p<0.10) was implemented. Then the 10 estimates coefficients of each variable were combined and the least significant factor was removed from the model. The process was continued until the final model was obtained. The proportional-hazards assumption was verified with the use of Schoenfeld residuals.
All statistical tests were done at the two-tailed α level of 0.05. All statistical analyses were generated using SAS V.9.3 for windows.
Results
Characteristics of patients
A total of 400 patients were enrolled in the WATCH-AF registry. Per protocol, 300 (75%) patients were included at the Bichat Stroke Centre (Paris) between 25 March 2014 and 10 April 2016 and 100 (25%) at the Lyon Stroke Unit between 27 December 2015 and 14 May 2016, and followed 1 year. Baseline characteristics of patients are presented in tables 1 and 2. A total of 370 patients (92.5%) had an ischaemic stroke as qualifying event and 30 patients (7.5%) had haemorrhagic stroke. Overall, the mean age of patients was 79 years (SD, 11). Male represented near half of the population. A large proportion of patients had hypertension (79.3%).
Baseline characteristics according to treatment groups
Clinical scores at discharge according to treatment groups: long-term oral anticoagulant strategy (LTOAC) versus not on an LTOAC (no LTOAC)
Among patients on VKA before baseline, only 43% of patients had a TTR ≥70%.
Among 400 patients enrolled, 31 patients died before discharge (7.8%), 274 patients belonged to the group on a ‘long-term oral anticoagulant therapy’ strategy (68.5%), and 95 patients belonged to the group ‘not on a long-term oral anticoagulant therapy’ strategy (23.8%) for various reasons, mainly contraindications to long-term oral anticoagulant therapy, listed in table 3.
Reasons for not being on a long-term oral anticoagulant strategy after discharge (n=95)
Outcomes
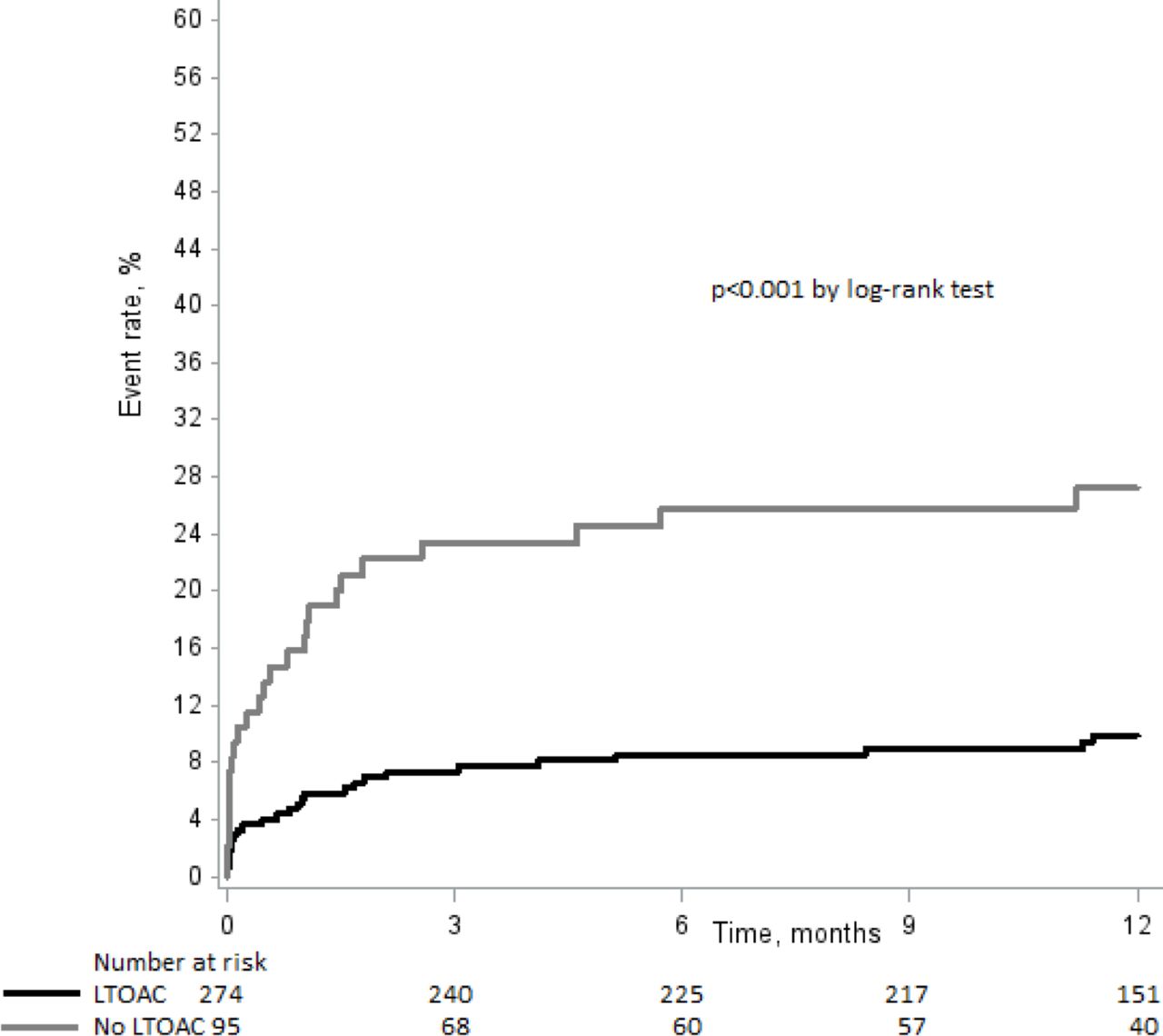
At 12 months, death or dependency occurred in 19.8% of patients on a long-term oral anticoagulant strategy and in 33.5% of patients not on a long-term oral anticoagulant strategy (p=0.002).figure 1 At 12 months, brain infarction or brain haemorrhage occurred in 9.9% of patients on a long-term oral anticoagulant strategy and in 27.2% of patients not on a long-term oral anticoagulant strategy (p<0.001) (table 4).

Twelve-month risk of death or dependency (from stroke onset to 12 months) according to treatment groups: long-term oral anticoagulant strategy (LTOAC) versus not on an LTOAC (no LTOAC).
Outcomes events rates according to treatment groups: long-term oral anticoagulant strategy (LTOAC) versus not on an LTOAC (no LTOAC)
Predictors of outcomes
Death and dependency
Online supplementary table 1 shows variables associated with the risk of death or dependency in univariable analysis.
Supplemental material
In multivariable analysis, Rankin score ≥2 (almost threefold increase for mRS 2 and 3, and 14-fold increase for mRS 4 and 5), haemoglobin level, treatment groups (long-term oral anticoagulant strategy vs not on a long-term oral anticoagulant strategy), age, total cholesterol level and presence of small vessel disease (with a fourfold increase) were predictors of death or dependency (online supplementary table 2). The adjusted risk of death or dependency was onefold and half higher in patients not on a long-term oral anticoagulant strategy as compared with patients on a long-term oral anticoagulant strategy (HR 1.65; 95% CI 1.05 to 2.61; p=0.032).
Recurrent brain infarction/brain haemorrhage
Online supplementary table 3 shows variables associated with brain infarction or brain haemorrhage in univariable analysis.
In multivariable analysis, Rankin score 4 or 5 (with a fivefold increase), glucose level, haemoglobin A1C, diastolic blood pressure, abnormal aortic valve, C reactive protein level, presence of atherothrombosis and treatment groups were predictors of brain infarction or brain haemorrhage (online supplementary table 4).
As compared with patients on a long-term oral anticoagulant strategy, the adjusted risk of brain infarction/brain haemorrhage was twofold and half higher in patients not on a long-term oral anticoagulant strategy (HR 2.46; 95% CI 1.36 to 4.44; p=0.003).
Discussion
The WATCH-AF registry shows that, among patients with stroke and AF, one-fourth cannot receive a long-term oral anticoagulation strategy. One-third of these patients were dead or dependent at 12 months with an adjusted risk multiplied by 1.65 compared with patients who received a long-term oral anticoagulant strategy, and one-fourth had a recurrent brain infarction or brain haemorrhage with an adjusted risk multiplied by 2.5. The new finding of this prospective registry is the proportion of patients with contraindication to long-term oral anticoagulation after a stroke, based on precise assessment using scores of disability, severity, cognitive functions and functional independence after the stroke event, as well as the 1-year risk of this group. These high proportions and risks question the necessity of finding therapeutic alternatives to long-term oral anticoagulant for these patients.
Beside treatment groups, independent predictors of death or dependency included the presence of small vessel disease (either multiple small deep infarcts or severe—Fazekas III—leukoaraiosis or microbleeds) with a fourfold increase and, not surprisingly, a Rankin score more than 1 (any degree of disability) with an almost threefold increase for a discharge mRS of 2 or 3 (needing some help but functionally independent), and a 14-fold increase for a mRS of 4 or 5 (needing permanent help or bedridden). Apart from not being on a long-term oral anticoagulant strategy, discharge Rankin score 4 or 5 was also the best independent predictor of recurrent brain infarction or brain haemorrhage.
This real-life, prospective registry, without any patient selection, shows that the risk of recurrent brain infarction or brain haemorrhage is still very high, even in the group on a long-term oral anticoagulant strategy with a 9.9% annual risk, showing that beside the antithrombotic treatment, other treatment strategies need to be found to decrease this risk, including risk factors control and strategies to improve adherence to treatments such as therapeutic education programme. The 27.2% annual risk of recurrent brain infarction or brain haemorrhage in patients not on a long-term oral anticoagulant strategy strengthens the case for alternative preventive strategies in these patients to be trialled such as left atrial appendage closure. According to figure 2, this risk is maximum during the first 3-month period postindex stroke. The reasons for not being on a long-term anticoagulant strategy were patient refusal, contraindication to long-term oral anticoagulant, comorbidity, frailty, patient bedridden or with severe dementia, history of bleeding precluding a long-term oral anticoagulant strategy or adherence to treatment (table 3).

{kind=link}
{kind=link}
Twelve-month risk of brain infarction or brain haemorrhage (from stroke onset to 12 months) according to treatment groups: long-term oral anticoagulant strategy (LTOAC) versus not on an LTOAC (no LTOAC).
The strengths of this registry were that (1) both stroke centres were primary care with a dedicated catching area, (2) inclusions have been consecutive and exhaustive with systematic verification that no patient with stroke and AF have been missed, (3) in every individual patient we retrospectively collected information about knowledge of AF, chosen treatment strategies by their primary care physician or cardiologist, risk factor stratification including CHA2DS2VASC, HAS-BLED, ATRIA, STRATIFY, IADL and about treatment adherence to VKA (eg, INR and TTR), over the previous 6 months, (4), using a high level of precision, we thoroughly evaluated patients at baseline and during a 1-year follow-up at four visits concerning concurrent underlying causes of stroke (eg, all patients had a brain MRI, extracranial and intracranial artery assessment, transthoracic and transoesophageal echocardiography) such as associated atherosclerotic disease and cerebral small vessel disease, risk stratification (CHA2DS2VASC, HAS-BLED, ATRIA scores), index stroke severity (NIHSS), disability (mRS), functional independence (IADL), risk of fall (STRATIFY risk assessment tool), cognitive function (MMSE), in order to precisely determine treatment strategy according to ESC/EHRA guidelines and (5) the very large sample size for this kind of precisions.
Generalisability of this study was limited as it involved only two centres, although busy stroke centres acting as primary care centres with a dedicated catching area, however, for the kind of precision that we set up in this registry we needed highly motivated centres, and a multicentre assessment with such a precision and numerous scales would have made the registry not feasible or with a lot of missing data. Our sample size can be viewed as rather small for an AF cohort. However, for the precision in scales and workup that the study needed, a sample size of 400 was an enormous effort. A much larger sample size with additions of other centres could have improve the overall generalisability, but at the expense of lack of precision.
In conclusions, we found that patients with stroke and AF not suitable to a long-term oral anticoagulant strategy represented one-fourth of the cohort and that they were at a very high 1-year risk of death and dependency and of brain infarction/brain haemorrhage recurrence. Alternative treatment options, such as left atrial appendage closure, should be trialled in these patients.
Acknowledgments
This study was conducted by an academic research organisation 'Charles Foix group for clinical trial and registry in stroke' at University of Paris, Paris, France.
References
Footnotes
Contributors CG collected the data, interpreted the data and wrote the first draft of the manuscript. PA designed the study, obtained funding, interpreted the data and wrote the first draft of the manuscript. HC did the statistical analysis, generated tables and figures. Other authors collected the data, revised the draft and contributed for important intellectual content of the manuscript.
Funding This study was funded by SOS-ATTAQUE CEREBRALE (a not-for-profit stroke survivors association) via an unrestrictive grant from Boston Scientific (the maker of a left atrial appendage closure device).
Competing interests NN reports the following relationships: receipt of research grants support from Pfizer, Sanofi, from The French National Research Agency and consultancy fees from Boehringer-Ingelheim, Bayer et Amgen. PA reports receipt of research grant support from Pfizer, Sanofi, Bristol-Myers-Squibb, Merck, AstraZeneca, Boston Scientific and from the French government, and consulting fees from Pfizer, BMS, Merck, Boehringer-Ingelheim, AstraZeneca, Bayer, Daiichi-Sankyo, Edwards, Boston Scientific, Kowa, GSK, Fibrogen, Amgen, Shin Poong, Gilead, and lecture fees from Bayer, St-Jude Medical, Amgen, Pfizer, Sanofi.
Patient consent for publication Not required.
Ethics approval The study complies with the Declaration of Helsinki, the locally appointed ethics committee has approved the research protocol (Comité de Protection des Personnes Ile de France 5).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.