Article Text

Abstract
Background Bariatric surgery reduces cardiovascular risk in obese patients. Heart failure (HF) is associated with an increased perioperative risk following bariatric surgery. This systematic review aimed to assemble the evidence on bariatric surgery in patients with known HF and the potential effect of bariatric surgery on incident HF in obese patients without prevalent HF.
Methods We performed a comprehensive literature search up to 30 September 2017 and included studies comparing bariatric surgery to non-surgical treatment in patients with known presurgical HF. To assess whether bariatric surgery has any effect on incident HF, we also assembled studies looking at new-onset HF among patients without HF prior to surgery.
Results We found five observational studies (0 randomised trials) comparing bariatric surgery with non-surgical treatment in patients with a diagnosis of HF prior to surgery. A review of the available studies (n=676 patients) suggested reduced admission rates for HF exacerbation and increased left ventricular ejection fraction after bariatric surgery. No meta-analysis was possible due to the heterogeneous nature of these studies. Seven studies (one randomised trial) reported data on new-onset HF in obese patients without HF prior to bariatric surgery (n=111 127 patients). When comparing surgical to non-surgical treatment groups, the pooled univariable and multivariable HRs for incident HF were 0.28 (95% CI 0.13 to 0.55) and 0.44 (95% CI 0.36 to 0.55), respectively.
Conclusion In this systematic review, no randomised trial assessed the benefits and risks of bariatric surgery in obese patients with concomitant HF. Available studies do, however, show that surgery might prevent incident HF.
- bariatric surgery
- heart failure
- incidence
- meta-analysis
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Bariatric surgery is known to reduce cardiovascular risk in obese patients.
There is evidence that obesity leads to increased rates of heart failure (HF). Bariatric surgery has been a valuable option for the treatment of metabolic disease like diabetes mellitus type 2 and has been shown to lead to more durable outcomes than conventional treatment.
Small studies have shown that bariatric surgery might also be used for the treatment of HF in obese patients.
What does this study add?
We strived to review the available data on patients with HF undergoing bariatric surgery.
We focused on the different outcomes such as mortality, major cardiovascular events, hospitalisations for HF and quality of life.
Furthermore, we meta-analysed the data available for the development of HF in obese patients without established HF undergoing bariatric surgery.
The results showed a significantly lower risk of developing HF in patients undergoing surgery when compared with non-surgical management.
How might this impact on clinical practice?
We showed the necessity of further randomised controlled trials for bariatric surgery as the treatment of HF in obese patients.
Additionally, as there is no current known treatment for HF with preserved ejection fraction, we showed the importance to further investigate bariatric surgery as a possible alternative to medical treatment in obese individuals.
Introduction
Heart failure (HF) is estimated to affect 23 million individuals worldwide.1 In the USA, the prevalence of obesity is 35% among men and 40% among women.2 3 Recent data from the European Union report an obesity prevalence of 15%, while an additional 50% are reported to be overweight.4 In the general population, a higher body mass index (BMI) is a strong and independent predictor of HF, with an attributable risk for HF of 14% in women and 11% in men.5 In a study from 2009, overweight participants had a 49% (95% CI 32 to 69) and obese participants had a 180% (95% CI 124 to 250) increase in HF risk compared with lean participants.6 In a previous meta-analysis of 23 prospective studies, a 5-point increment in BMI led to a summary relative risk (RR) for HF of 1.41 (95% CI 1.34 to 1.47).7
There is inconsistent evidence on whether obesity is associated with a specific type of HF. Some studies have reported HF with preserved ejection fraction (HFpEF) and HF with reduced ejection fraction (HFrEF) to occur to the same extent in obese patients,8 while others found a stronger positive association of obesity with HFpEF than with HFrEF.9 In the Candesartan in Heart Failure-Assessment of Reduction in Mortality and Morbidity (CHARM) programme, patients in the CHARM-Preserved Trial had a higher baseline BMI compared with those in CHARM-Alternative and CHARM-Added (29 kg/m2 vs 27 kg/m2 and 28 kg/m2, respectively).10
Bariatric surgery has become a valuable option in treating obesity due to its effect in achieving disease remission and durable outcomes compared with conventional treatment, especially for type 2 diabetes.11–14 Small studies suggest that bariatric surgery has a positive impact on heart morphology in obese individuals without HF.15 16 In small case series among patients with HF, bariatric surgery improved ejection fraction and has been used as a bridge to transplantation.17 18 In the STAMPEDE (Surgical Treatment and Medications Potentially Eradicate Diabetes Efficiently) trial, bariatric surgery was shown to be safe in patients using cardiovascular medication, suggesting some level of pre-existing cardiovascular disease.19 On the other hand, a history of HF has been reported to be a strong risk factor for mortality after bariatric surgery,20 21 such that the benefit risk ratio in patients with HF is currently unknown. As the risk of bariatric surgery in patients with HF is unknown, there is a possibility that bariatric surgery in patients with established HF may be underused. The lack of data in this field may also lead to very subjective decision making on whether a patient is considered fit to undergo surgery.
We, therefore, performed a systematic review and meta-analysis to assess the existing evidence on the effects of bariatric surgery on mortality rates, the number of major adverse cardiovascular events, clinical outcomes and cardiac function in patients with HF prior to bariatric surgery. Additionally, we aimed to assess the potential impact of bariatric surgery on incident HF.
Methods
Search strategy
With the help of an experienced research librarian, we established a search strategy for publications using MeSH terms and keywords such as ‘bariatric surgery’ and ‘heart failure’ and systematically searched PubMed, EMBASE and Cochrane databases from the inception date until 30 September 2017. The complete search strategy is displayed in the online supplementary file 1 and online supplementary file 2. We searched ClinicalTrials.gov for current studies involving patients with HF undergoing bariatric surgery. We did not impose any restrictions on topic language, publication date, sample size or study type and included abstracts as well as poster presentations from scientific conferences. In addition, we scanned the reference lists of articles of eligible studies and of previous reviews for further relevant articles. Finally, we contacted authors of scientific presentations from conferences and of published papers in the field to check for unpublished relevant results.
Supplemental material
Supplemental material
Study selection
All titles and abstracts of the studies identified by the literature search were independently evaluated by two reviewers (SeB and SB). If one reviewer deemed the article to be potentially relevant, a full-text review was conducted. Disagreements on the inclusion of the full-text article were settled by a consensus discussion between the two reviewers. In case of remaining discrepancies, a third reviewer (PM) made a final decision. Criteria considered were (1) appearance of HF either as a prevalent comorbid condition or incident HF as an outcome in patients without HF prior to undergoing bariatric surgery, (2) outcomes measured in patients with HF undergoing bariatric surgery including mortality rates, the number of major adverse cardiovascular events, clinical outcomes such as rehospitalisations due to HF or reduction of exertional dyspnoea and change in cardiac function, (3) the presence of a control group being treated with intensive medical therapy.
Assessment of study quality
Two reviewers (SeB and SB) assessed the risk of bias and study quality in all eligible studies using the modified Newcastle Ottawa Quality Assessment Scale for observational studies22 and the Cochrane Risk of Bias Tool for randomized controlled trials (RCTs).23
Data extraction
Data from the included studies were extracted by one reviewer (SeB) into a preformatted spreadsheet and checked by another reviewer (SB). We extracted the number of incident HF events, person-years of follow-up and HRs, where available. In addition, we gathered information on sample size, duration of follow-up and a set of predefined characteristics, including gender, age, BMI, hypertension, coronary heart disease and diabetes. Endpoints considered were incidence of HF, hospitalisation for HF, symptoms of HF, quality of life, left ventricular mass, left atrial size and left ventricular function.
Statistical analysis
Due to the lack of uniform clinical outcomes such as mortality or major adverse cardiac events, we decided not to meta-analyse the findings of our search on patients with pre-existing HF. The same applied to studies on clinical outcomes, heart function and morphology before and after bariatric surgery, as the reporting on these outcomes was heterogeneous and could not be statistically compared due to lack of uniform measures. The data for incident HF among patients without HF prior to surgery are presented quantitatively. We calculated the RR from all available studies. Most adjusted HRs were used in these analyses. For the quantitative analysis, random effects meta-analysis was conducted with STATA software V.13 (Stata, College Station, Texas, USA) for the RR and HR. Heterogeneity of the included studies was assessed by Q statistic and quantified using I2 measure. Values of >50% were considered to indicate substantial heterogeneity while values of <25% were considered to indicate low heterogeneity.24 We performed a sensitivity analysis comparing the estimates from observational studies to the estimates of the available RCT.
Results
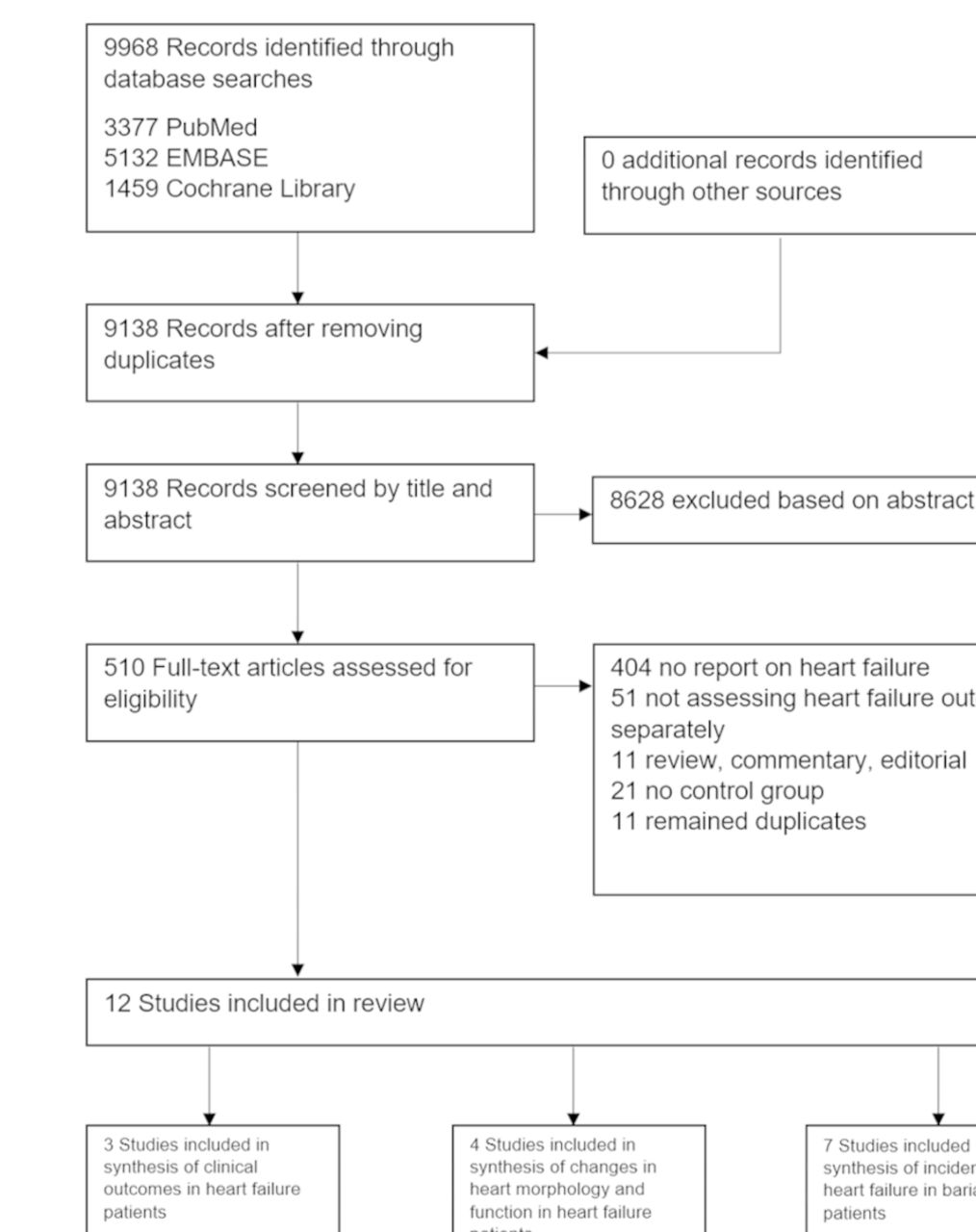
Our search identified 9968 publications, as shown in figure 1. We conducted a full-text search of 510 publications. Most of the remaining studies were not considered because patients with HF were excluded or no information on patients with HF was available. Two publications were excluded because they focused on HF as a cause of death rather than presenting the incidence of HF.11 25 At the end, 12 studies were retained for further analysis, including 1 RCT and 11 observational studies, 2 of them abstracts. The included studies and their characteristics are shown in table 1. Further details are provided in figure 1. Additional searches of ClinicalTrials.gov and the reference list of included publications did not yield any further studies not included in the initial search. Of the 12 studies, 318 26 27 compared clinical outcomes in patients with HF undergoing bariatric surgery, 418 26 28 29 investigated heart function and morphology changes in patients with prevalent HF and 730–36 assessed incident HF in obese patients without HF prior to surgery.

Study selection flow diagram.
Baseline characteristics in included studies
Quality of the individual studies according to the Newcastle-Ottawa Scale is shown in table 2. In general, we found a low risk of bias among the included studies. The randomised trial had a low risk of selection bias and selective reporting, but a high risk for performance and detection bias as blinding is difficult to establish (table 2).
Quality of included studies according to the modified Newcastle-Ottawa scale for cohort studies and the Cochrane collaboration tool for randomised trials
Clinical outcomes
Comparison of clinical outcomes in patients with prevalent HF was available from three observational studies, but no RCT (table 1; n=565). In these studies, bariatric surgery effectively improved clinical symptoms and quality of life and reduced admission rates for HF.18 26 27 Ramani et al found significantly lower hospital readmission rates in patients undergoing bariatric surgery than in controls at 1 year (hospital readmissions 0.4±0.8 vs 2.5±2.6, p=0.04). Furthermore, the NYHA class improved in surgical patients while it deteriorated significantly in controls (2.3±0.5, p=0.02 vs 3.3±0.9, p=0.02).18 Another study found significant improvements in quality of life (on a 10 point Likert scale: 3 (0–6) to 7 (7–10) points presurgery and postsurgery, p<0.01), less frequent exertional dyspnoea (on a 10 point Likert scale: 4 (1–5) to 2 (1–5) points in the surgical group and 3 (1–3) to 3 (3–4) points in the control group preintervention and postintervention, p=0.01) and reduction in leg oedema (on a 10 point Likert scale: 4 (1–5) to 3 (1–5) points in the surgical group and 3 (1–4) to 3.5 (1–5) points in the control group preintervention and postintervention, p=0.04) in patients undergoing surgery, while the control group showed no significant changes.26 Last, Shimada et al showed a significant reduction of emergency department (ED) visits or hospitalisations for HF exacerbations (58 ED visits or hospitalisations 13–24 months after surgery compared with 82 ED visits or hospitalisations 13–24 months prior to surgery, adjusted OR 0.57, p=0.003) in a self-controlled study comparing a reference period before surgery to a period 13–24 months after surgery.27 None of the studies assessed mortality or major adverse cardiac events.
Cardiac function
A total of four observational studies provided information on changes in cardiac function and/or morphology in patients with established HF (table 1; n=111). One publication was an abstract. Ramani et al showed a significant improvement in left ventricular ejection fraction (LVEF) in patients undergoing bariatric surgery (p=0.005) while patients who were treated conventionally with diet and exercise counselling did not.18 Another study found a significant increase in LVEF in the bariatric surgery group (p=0.0005) but not in the control group (p=0.056).29 Two studies did not find significant differences in LVEF between groups.26 28 The available preintervention and postintervention LVEF numbers of the included studies are summarised in table 3. We did not pool these results due to the lack of uniform measures used to present the data.
Changes in left ventricular ejection fraction after bariatric surgery compared with conventional treatment
Incidence of HF after surgery
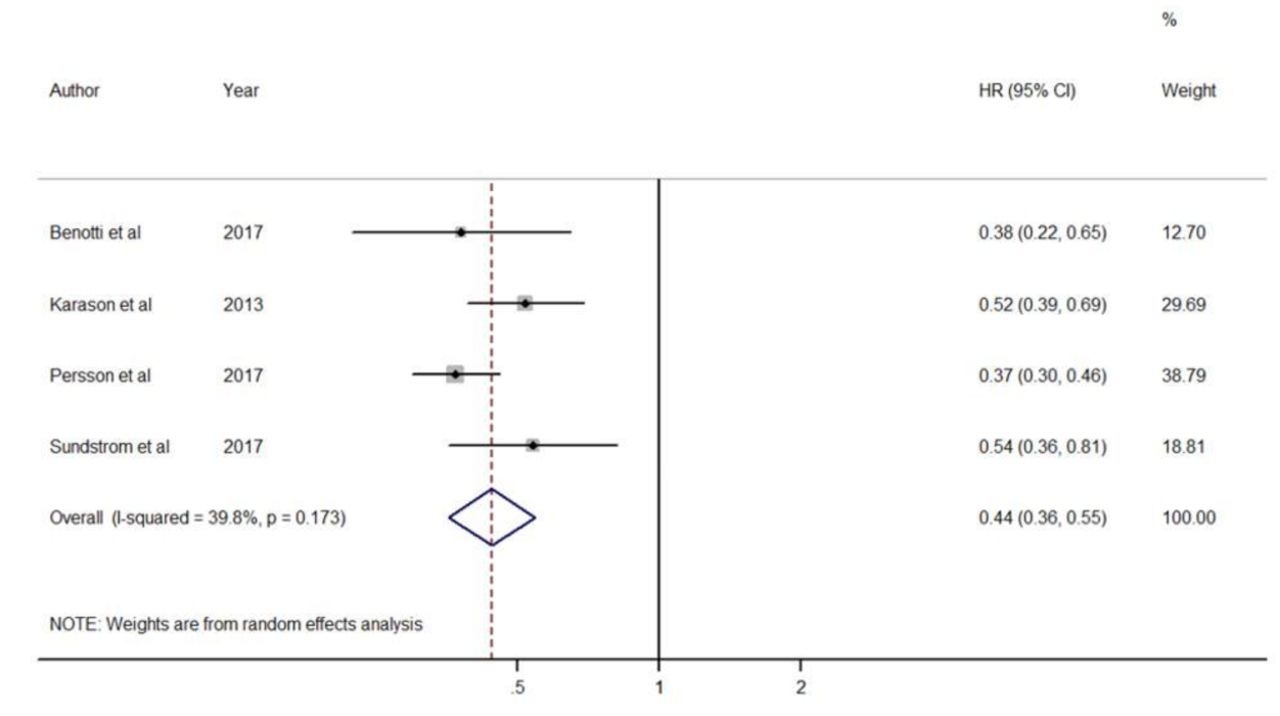
Our search yielded 7 studies that assessed incident HF after bariatric surgery compared with medical management, 1 RCT (n=119) and 6 observational studies (n=111008) (table 1, figure 2). There was a total of 283 cases of incident HF in the surgical groups and a total of 2520 cases of incident HF in the control groups as shown in table 4. The unadjusted summary RR for the observational studies was 0.27 (95% CI 0.13 to 0.6) and the unadjusted RR for the randomised controlled trial was 0.33 (95% CI 0.01 to 8.02). The summary RR for all included studies was 0.28 (95% CI 0.13 to 0.59). The I2 test showed a heterogeneity of 95.3% (p<0.001). A meta-analysis of the most-adjusted HR yielded a summary RR of 0.44 (95% CI 0.36 to 0.55), as shown in figure 3. Heterogeneity for the included studies was 39.8% (p=0.17).

Summary of unadjusted risk ratios for incidence of heart failure in obese patients without pre-existing heart failure undergoing surgery versus conventional treatment by random-effects model. Small black diamonds represent the RR for individual studies with corresponding 95% CI denoted by black lines. Open blue diamond represents the pooled risk ratio and blue line labels the estimated predictive interval. Meta-analysis is computed by random-effects model. RR, risk ratios.
Cases of incident heart failure

{kind=link}
{kind=link}
{kind=link}
Summary of most-adjusted HRs for incidence of heart failure in obese patients without pre-existing heart failure undergoing surgery versus conventional treatment by random-effects model. Small black diamonds represent the HR for individual studies with corresponding 95% CI denoted by black lines. Open blue diamond represents the pooled risk ratio and blue line labels the estimated predictive interval. Most-adjusted HR were used for this analysis. Meta-analysis is computed by random-effects model.
Discussion
Obesity and HF are two interrelated disease epidemics. Bariatric surgery leads to more durable and sustained weight loss and effectively remits at least some of the adverse effects of obesity, such as diabetes, dyslipidaemia and hypertension.11–14 Our review revealed a gap of knowledge about the effect of bariatric surgery among obese patients with HF. We could not identify any RCT of bariatric surgery versus medical management in patients with HF at baseline. Some small studies suggested improvements in LV function, but the results were not consistent. Furthermore, there are several limitations to the identified studies as some of the data we found were from non-peer-reviewed sources such as congress abstracts as well as very heterogeneous in the reporting of different outcomes.
This uncertainty of the effects of bariatric surgery in patients with HF is a problem, as several studies have shown that HF is an important risk factor for mortality after surgery and a considerable risk for other adverse events remains for obese patients undergoing bariatric surgery.20 21 37 The risk of selection bias when choosing subjects with HF to undergo surgery in the mostly retrospective studies must be mentioned as well. Improvements in heart function and morphology after bariatric surgery have been previously shown in obese patients without pre-existing HF.15 There is also evidence in the literature that weight loss results in the reversal of metabolic derangements and is accompanied by a normalisation of left ventricular diastolic function in obese patients.38 Several publications have discussed the effects of obesity on cardiomyopathy. In obese patients, there are various metabolic and neurohormonal alterations which might contribute to abnormalities of cardiac structure and function. Obesity is suspected to induce inflammation and insulin resistance which is associated with negative effects on cardiovascular risk factors. But even in the absence of other forms of heart disease, changes in cardiovascular hemodynamics and ventricular function arise. Sleep-disordered breathing leading to pulmonary arterial hypertension and left ventricular hypertrophy have been discussed as reasons for development of HF in obesity cardiomyopathy.39 40 However, our comprehensive literature search found little evidence as of today that surgery could actually improve heart function in obese patients with overt HF.
We found some data that showed promising effects of bariatric surgery reducing the incidence of HF among patients without HF at prior to bariatric surgery. The summary RR showed a large reduction of incident HF, but the study heterogeneity was high, at least in part explained by bias and confounding. Attenuation of the RR estimate when using the most-adjusted HRs further underscores the importance of confounding in this context. Adequately powered randomised trials are needed to inform clinical practice in this area. Due to these effects, there is a chance that due to similar mechanisms bariatric surgery might be useful in the treatment of overt HF.
Evidence from different trials suggests that obesity is linked to HFpEF and even may produce a distinct obese phenotype of HFpEF.9 10 41 There are no exact numbers of patients with this type of HF and further research is needed to better understand the relationship of obesity with different types of HF. Importantly, no medical treatment, especially no drug therapy,has been shown to be unequivocally effective in patients with HFpEF,42 such that the evaluation of bariatric surgery in this patient population would be particularly important.
In summary, our systematic review and meta-analysis found little high-quality evidence on the benefits and risks of bariatric surgery among patients with established HF. On the other hand, our meta-analysis showed a significant reduction in new onset HF in obese subjects undergoing surgery. Further research is needed to better understand the benefits and risks of bariatric surgery on obese subjects with HF. This would be particularly important for patients with HFpEF, where no effective medical treatment is currently available.
References
Footnotes
Contributors The study concept and design was developed by SeB and DC. Data acquisition was obtained by SeB, PM, SA, SB and DC. SeB, PM and DC drafted the manuscript. All authors contributed to data interpretation and provided critical revision of the manuscript for important intellectual content. The statistical analyses were performed by SeB, MB and PM. DC has been the study supervisor and is the corresponding author.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This paper is a systematic review and meta-analysis and relies on previously published data. Ethics approval was thus not deemed necessary.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.