Article Text

Abstract
Background To assess the current state of patient information and decision-making in congenital aortic and pulmonary valve disease, we conducted a survey among patients, parents and physicians.
Methods A questionnaire was sent by ground mail to 157 adults and 32 parents of children who previously underwent surgery for congenital aortic or pulmonary valve disease at 0–40 years of age between January 2005 and February 2014 at the Erasmus University Medical Center and to all paediatric and adult congenital cardiologists and congenital cardiac surgeons in the Netherlands (n=88).
Results 73 patients/parents (39% response rate, 62 adult patients, 11 parents of paediatric patients) and 35 physicians (40% response rate) responded. Median patient age at the time of surgery was 25.7 years. Basic disease-specific knowledge was adequate in 42% of patients/parents and numeracy was sufficient in 47%. Patients/parents reported that they rely heavily on their physicians for information and often experience difficulty in finding reliable information elsewhere. They lack information on psychosocial aspects of disease (29% of respondents) and risks and benefits of treatment options (26%). They feel less involved in decision-making than they would prefer to be (p=0.014). Decisional conflict at the time of surgery was experienced by 31% of patients/parents. If they had to do it again, 72% of patients/parents would want the same treatment. Quality of life is often impaired due to various valve-related anxieties and lifestyle changes. Physicians reported that they are unable to fully inform and sufficiently involve patients, due to limited patient/parent knowledge and understanding (56%) and limited time during consultations (32%). Patients/parents (98%) and physicians (97%) agree that they should have shared roles in decision-making.
Conclusion The substantial shortcomings in our current practice of patient information and decision-making underline the need for innovative solutions, such as careful implementation of patient information tools and shared decision-making in the care path.
- congenital heart disease
- cardiac surgery
- valvular disease
- surgery-valve
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
It has been previously described that disease-specific knowledge among patients with congenital heart disease and their parents is often limited. However, it remains poorly understood which factors may play a role in this limited knowledge and little is known about patient involvement, decision-making and anxiety in these patients. Furthermore, prior investigations have focused mainly on patient and parent perspective and thus the perspective of the physician remains poorly described.
What does this study add?
This study, capturing both patient/parent and physician perspective, provides a unique and valuable insight into how we currently inform and involve patients and their parents in congenital cardiac care. It demonstrates that patients, parents and physicians alike currently experience important shortcomings in patient information and decision-making and succeeds in identifying patient-related, physician-related and healthcare-related areas for improvement.
How might this impact on clinical practice?
Our findings are of crucial importance in informing clinicians and policymakers on how we currently inform and involve patients and serve to guide efforts to improve this. They underline the urgent need for innovative solutions, such as careful implementation of patient information tools and shared decision-making in the care path and provide specific areas of focus for the development and implementation of such solutions.
Introduction
Due to major advances in the management of congenital heart disease over the past decades, approximately 90% of patients with congenital heart disease currently reach adulthood.1–3 This increasingly allows patients to live full, active and longer lives. However, congenital heart disease often has consequences that impact many facets of life, both clinical and personal.1 4 Furthermore, it often requires important decisions to be made about treatment, both in choosing between treatment or a conservative approach and choosing between different treatment options such as the choice for a mechanical or a bioprosthetic valve replacement. These decisions may have important implications for the patients’ further lives with regard to, for instance, longevity, pregnancy, career planning and daily life, especially in younger patients with more dynamic lifestyles.4 Congenital aortic and pulmonary valve diseases, in particular, usually allow for a relatively long and active life, but often with important consequences for lifestyle and life planning and requiring multiple crucial decisions about treatment to be made along the way.2 3 5
To allow patients to better understand, cope with and adhere to the lifestyle changes imposed by their heart defect and to allow treatment to be tailored to their personal values and preferences, it is essential to inform patients and their relatives and involve them in the decision process.6–19 However, patients may not always be sufficiently informed and involved in their own care, which has been previously shown to lead to substantial impairments in quality of life, anxiety, depression, poor treatment adherence, poor health behaviour, suboptimal treatment decisions and poorer clinical outcome, and also poorer healthcare utilisation and higher healthcare costs.6–19
To investigate the current state of patient information and decision-making in congenital aortic and pulmonary valve surgery in the Netherlands, we conducted a cross-sectional survey among adult patients, parents of paediatric patients and physicians involved in the care for these patients.
Methods
Patient survey
This study was approved by the institutional review board (MEC-2015–099) and written informed consent was obtained from all participants.
Participants
Between January 2005 and February 2014, 198 consecutive patients aged between 0 and 40 years underwent valve repair or replacement for congenital aortic and/or pulmonary valve disease at the Erasmus University Medical Center. On 1 March 2015, patients ≥18 years old and parents of patients <18 years old at the time of the survey who were alive and residing in the Netherlands (total n=189, 157 adult patients and 32 parents) were approached by ground mail and asked to complete and return a printed questionnaire.
Questionnaire
An example of the patient questionnaire is listed in online supplementary appendix 1.
Supplemental material
Basic knowledge on postoperative outcome was assessed by asking respondents what the largest risk is after mechanical valve replacement (only aortic valve surgery patients), biological valve replacement (aortic and pulmonary valve surgery) and valve repair (only aortic valve surgery patients) using multiple choice questions for each. Possible answers were (1) thromboembolism and bleeding, (2) reoperation and (3) I don’t know. Knowledge was also assessed by asking respondents which procedure they/their child had undergone using a multiple choice question and comparing their answers with their medical records. Possible answers in this question were (1) mechanical valve replacement, (2) biological valve replacement and (3) valve repair.
Numeracy (ie, the understanding of numerical information, such as quantitative probabilities) was assessed using the validated Numeracy Scale20 and respondents were asked to indicate which form of risk visualisation (bar chart, pie chart or icon array) they preferred for presentation of risk information.
Experiences and views with regard to patient information and (shared) decision-making were assessed using multiple choice questions, 5-point Likert scales, open questions and the validated Control Preferences Scale.21
Uncertainty about treatment decision-making was assessed using the Decisional Conflict Scale.22
Postoperative valve-specific quality of life was assessed with a validated valve-specific questionnaire.5
Physician survey
Participants
All board registered paediatric cardiologists, adult congenital cardiologists and congenital cardiac surgeons in the Netherlands (n=88) were approached by email via the Dutch Associations for Pediatrics, Cardiology and Thoracic Surgery and asked to complete an electronic questionnaire.
Questionnaire
An example of the physician questionnaire is listed in online supplementary appendix 2. Physician age, specialty and years of experience were recorded. Experiences and views with regard to patient information and (shared) decision-making were assessed using multiple choice questions, 5-point Likert scales, open questions and the Control Preferences Scale.21
Supplemental material
Analyses
Analyses of clinical data were performed in Microsoft Office Excel 2011 (Microsoft, Redmond, Washington, USA) and in the R statistical software (V.3.3.3, R Development Core Team, R Foundation for Statistical Computing, Vienna, Austria). Continuous data are presented as mean±SD or median (range) and categorical data (including Likert scales) are presented as proportions and/or counts. Paired comparisons of Likert scale responses were done using Wilcoxon signed-rank test. All tests were two-tailed and statistical significance was inferred at a p<0.05.
Results
Patients
A total of 73 patients/parents responded and gave informed consent and were subsequently included in the study (39% response rate). Patient and respondent characteristics are shown in table 1.
Patient/respondent characteristics
Knowledge, numeracy and risk visualisation preference
Considering all knowledge questions collectively, 42% of respondents answered all questions correctly. Specifically, 51% of respondents answered all questions on postoperative risks correctly and 89% of respondents knew which procedure they/their child had undergone.
Forty-seven per cent of respondents answered all three numeracy questions correctly, 27% answered two out of three correctly, 16% 1 out of 3, and 10% 0 out of 3. Patients/parents indicated a strong preference for pie charts (61%) over bar graphs (29%) and icon arrays (10%) for visualisation of risk information.
Patient information
Patient/parent experiences and opinions with regard to patient information are presented in figure 1. Additionally, patients/parents report cardiologists (89%) and cardiac surgeons (26%) as their main sources of information, whereas patient information leaflets (8%) and the internet (5%) were less frequently reported as important information sources. The advantages and drawbacks of treatment options were discussed with the cardiologist in 93% of cases and with the cardiac surgeon in 42% of cases. This consultation took place >1 week prior to surgery in most cases (89%), but sometimes also between 1 day and 1 week prior to surgery (3%) or <1 day prior to surgery (8%).

Patient/parent (n=73) experiences and opinions with regard to patient information and decision-making. The graphs are centred on the response category ‘Neutral’ (vertical grey line in the centre of the graph). *Wilcoxon signed-rank p=0.014.
The most important topics patients/parents reported to lack information on (open question) were implications for personal life, life planning, prognosis and psychosocial aspects (29% of respondents), risks, benefits and drawbacks of treatment (options) (26%) and practical information on (early) postoperative care (17%).
Decision-making
Patient/parent experiences and views with regard to decision-making are presented in figure 1. Respondents felt less involved in decision-making than they would prefer to be (figure 1, Wilcoxon signed-rank p=0.014). The vast majority of patients/parents (98%) agree that they should have shared roles in decision-making (figure 2).
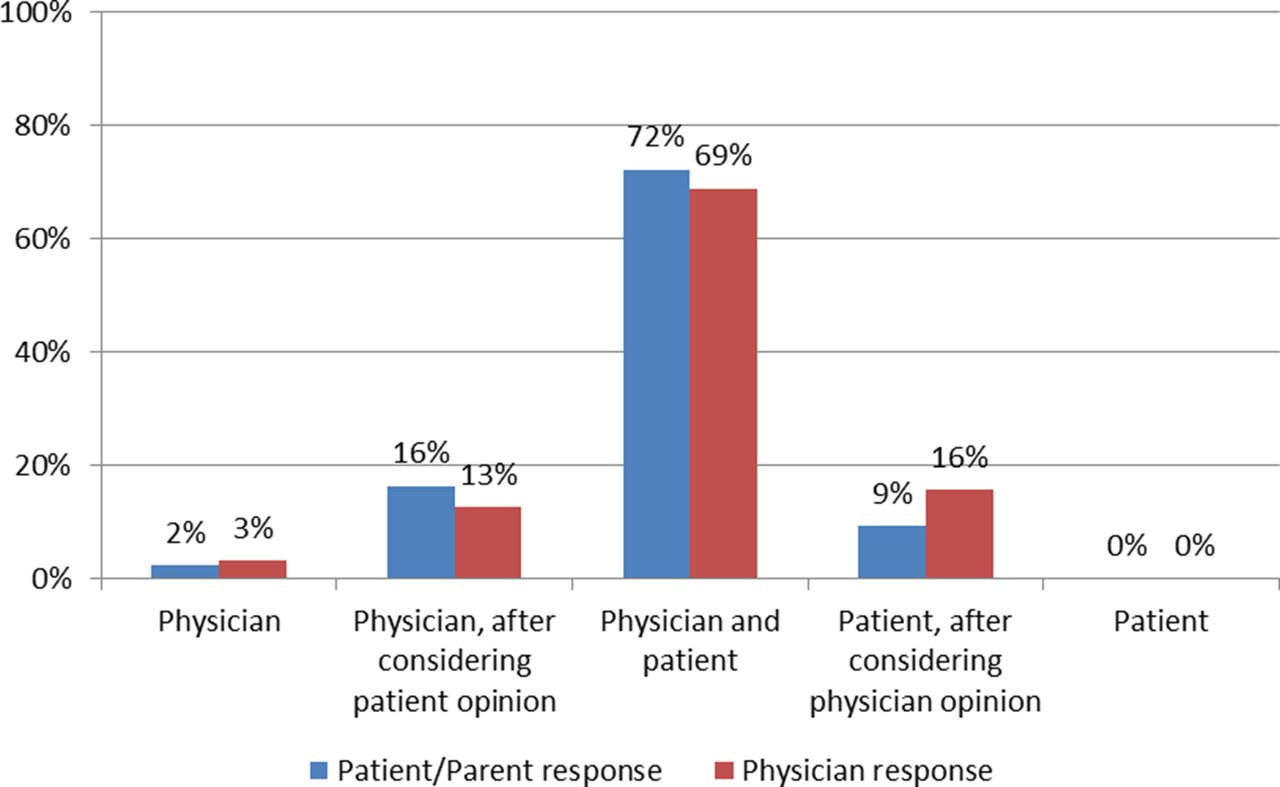
Control Preferences Scale: Who should make the final decisions about treatment? (73 patients/parents and 35 physicians responded). The sum of the middle three response categories represents the respondents that think that patients/parents and physicians should have shared roles in decision-making (98%).
Furthermore, at the time of surgery, 31% of patients/parents experienced decisional conflict (Decisional Conflict Scale score >25) and 13% experienced severe decisional conflict (score >37.5). Decisional conflict was highest in the subscales uncertainty about the best choice (35%, severe: 30%), clear about personal values for benefits and drawbacks (30%, severe: 23%) and feeling informed (23%, severe: 16%), followed by feeling supported (21%, severe: 16%) and decision effectiveness (16%, severe: 12%).
At the time of survey, 80% of patients/parents were satisfied with their replaced or repaired heart valve (10% neutral, 10% not satisfied) and 72% of patients/parents would want the same treatment if they had to do it all over again (18% neutral, 10% different treatment).
Valve-specific quality of life
Patients/parents experience impairments to quality of life due to various valve-related anxieties and lifestyle changes (figure 3), most frequently related to fear of reintervention (38% ‘frequently’ or ‘always’), anticoagulation use (34%), fear of thrombosis (31%) or bleeding (26%), valve sound (22%), fear of valve failure (22%) or the regular doctor visits and blood tests (9%).
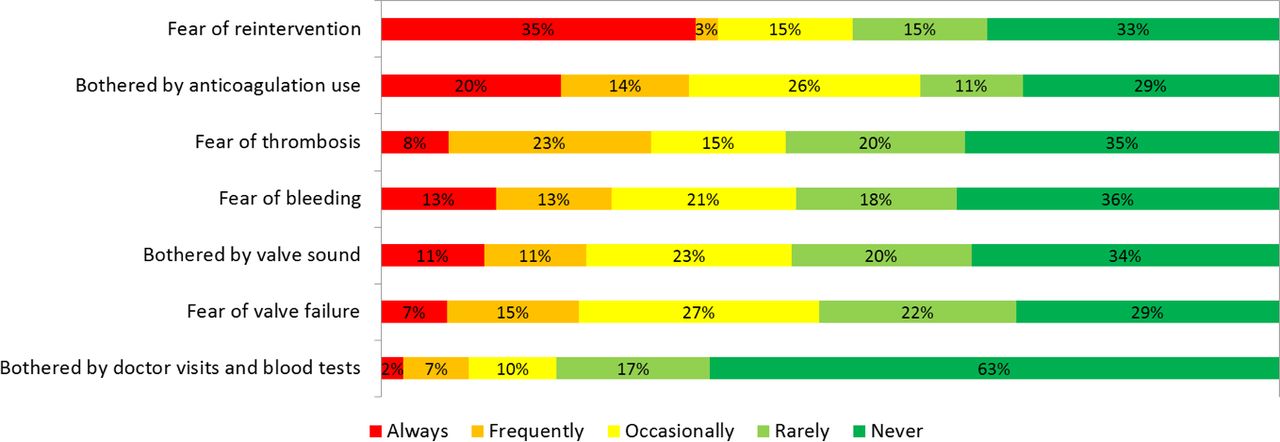
Factors that patients/parents (n=73) report as impairments of their quality of life. Always=more impairment=unfavourable.
Physicians
A total of 35 physicians responded (40% response rate), 14 paediatric cardiologists, 14 adult congenital cardiologists and 7 congenital cardiac surgeons. Median physician age was 44 years (range 33–64) and median experience in their respective fields was 9 years (range 0.3–32).
Patient information
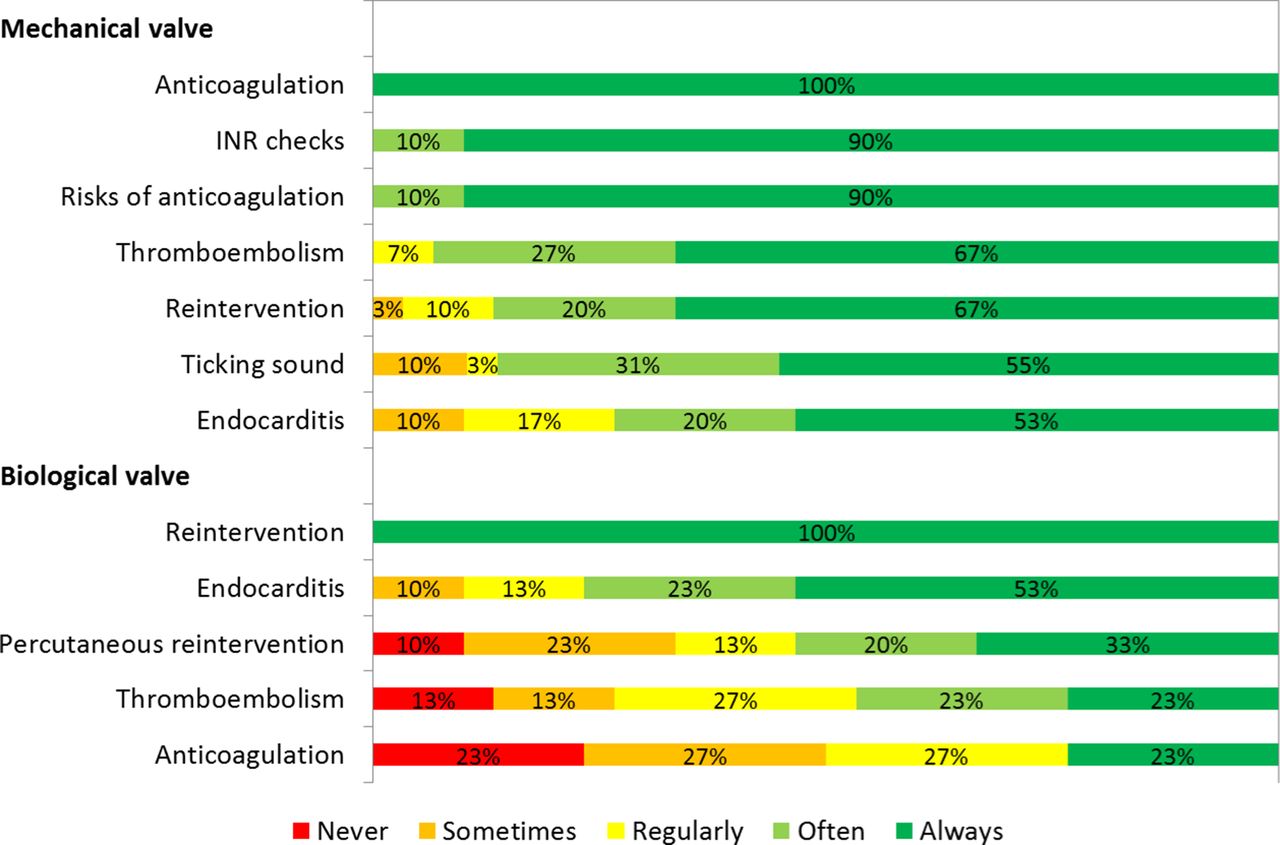
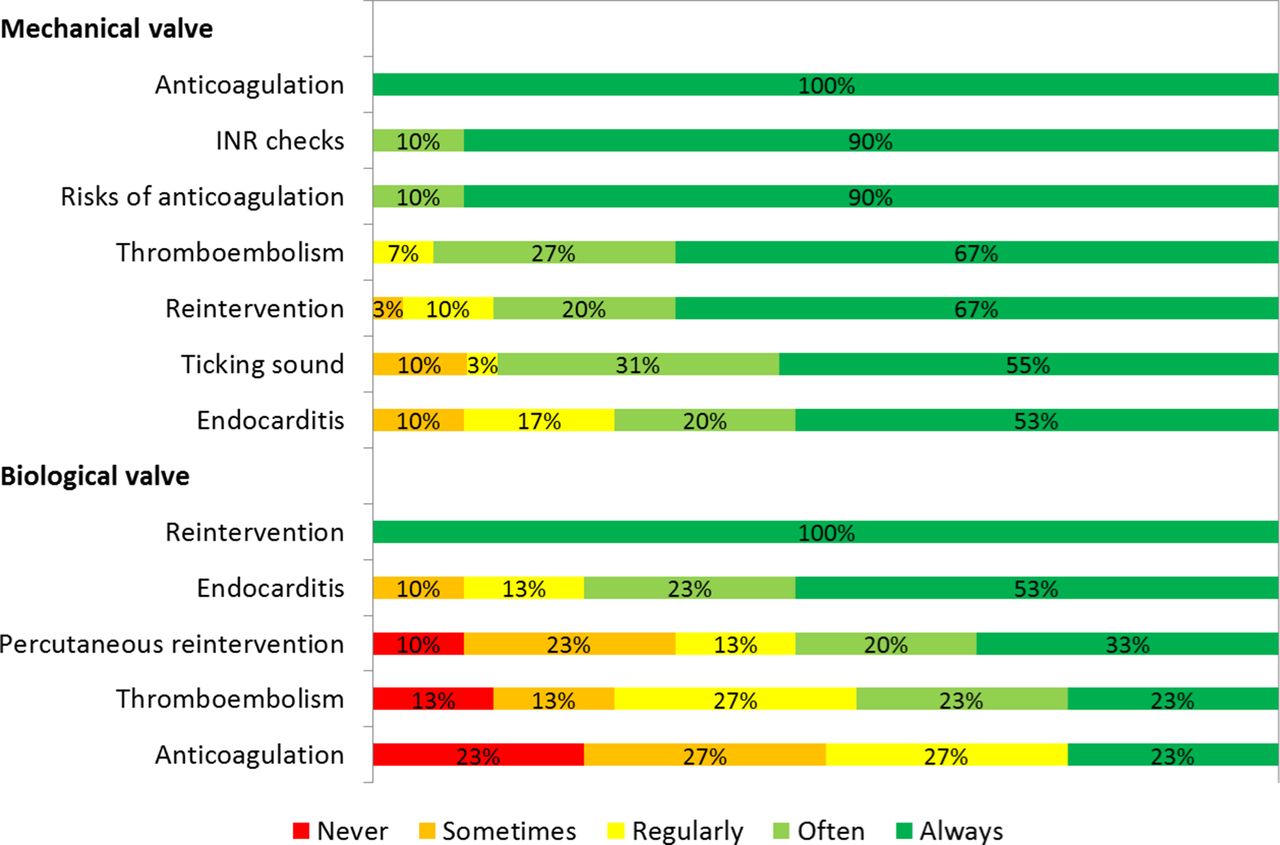
Physician experiences and opinions with regard to patient information are presented in figure 4. Additionally, physicians report cardiologists (94%) and cardiac surgeons (19%) as the main sources of information for patients/parents and the internet (3%) less so. Physicians report that do not always fully inform patients/parents of all the implications of their treatment (figure 5).

Physician (n=35) experiences and opinions with regard to patient information and decision-making. The graphs are centred on the response category ‘Neutral’ (vertical grey line in the centre of the graph).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Physicians (n=35): How often do you inform your patients about the various advantages and drawbacks of treatment? INR, international normalised ratio.
Decision-making
Physician experiences and opinions with regard to decision-making are presented in figure 4. The vast majority of physicians (97%) agree that they should have shared roles in decision-making (figure 2). Additionally, physicians report the most important barriers in involving patients/parents in decision-making (open question) to be limited patient/parent knowledge and understanding (56% of respondents), limited time during consultations (32%) and anxiety and uncertainty among patients/parents (24%).
Discussion
This study shows that in contemporary Dutch practice of congenital aortic and pulmonary valve surgery, patient/parent knowledge of basic information on their (child’s) condition is limited and their numeracy is poor. Patients/parents are not satisfactorily informed and rely heavily on their physicians for information. They feel less involved in decision-making than they would prefer to be and often experience substantial decisional conflict and valve-related anxiety. Physicians in turn are unable to inform patients/parents completely in the limited time they have, given the patients’/parents’ limited knowledge and understanding. Subsequently, although both physicians and patients/parents agree that they should have shared roles in decision-making, physicians experience challenges in involving patients/parents in their own care.
In congenital cardiac care, treatment often has a profound impact on lifestyle, life planning, quality of life and longevity, especially in younger patients with more dynamic lifestyles. Our results show that patients and their parents are often insufficiently informed of the consequences of the treatments they undergo. Our findings of limited knowledge among patients and parents are in line with prior research in (parents of) patients with congenital heart disease.16–18 23–28 Limited knowledge and limited availability of information have been previously described to be associated with anxiety, depression and impaired quality of life, which underlines the importance of adequately informing our patients and their parents.29 30
But why are patients/parents currently not satisfactorily informed? Our results show that they rely heavily on physicians to provide them the information they require and often experience difficulty in finding reliable information elsewhere. However, we found that the knowledge gap between patients and physicians along with the limited time reported to be available during consultations presents a challenge to physicians in meeting their patients’ information needs. Subsequently, physicians are not able to discuss all relevant information with all patients.
Furthermore, prior studies have shown that, of the information that is discussed during the consultation, only a small fraction is retained by patients/parents, only about 20%–60% as described in the literature.29 31 32 Our results show that, other than their physicians, there are few sources of reliable information available to patients, and the information that is available is often poorly comprehensible, contradictory and not tailored to their information needs and their specific disease state. Furthermore, current information, including information provided by caregivers, was reported to focus mainly on medical aspects of the disease and patients lack information on practical, psychosocial and lifestyle topics. Also, our findings of limited numeracy among patients/parents shows that the content and the format of patient information should be carefully considered.
Limited patient/parent knowledge also has an impact on treatment decisions and treatment outcome. As treatment decisions have such an important impact on patients’ personal lives, treatment outcome and goals should always be placed in the perspective of each individual patient’s lives and values. Optimal outcome for each patient can only be achieved if treatment is in alignment with patient preferences.5 19 33–35
As evidenced by our results, physicians are often confident that they are capable of reliably determining patient values themselves and sometimes even think they are capable of making value trade-offs on the patients’ behalf. However, prior research in other disease states has shown that there is often a substantial mismatch between patient values and physicians’ estimation thereof.36–38
Consequently, patients often undergo treatments with consequences that they are inadequately informed about and that do not match personal values and preferences. Our results show that this may be associated with substantial potentially avoidable impairments in quality of life. Thus, elucidating patient values and taking these values into account in treatment decision-making is crucial. Fortunately, the patients themselves are seasoned experts on their own values and an integral part of every healthcare setting. Involvement of patients in their own care is therefore essential.
However, our findings indicate that there are several barriers for patient involvement in clinical practice. Our study shows that physicians often experience difficulty in involving patients, most often due to a gap in knowledge and understanding between physicians and patients. This is confirmed by our findings of limited knowledge and numeracy among patients and parents. Thus, patients’ active participation in their own care first requires ample knowledge of medical and psychosocial aspects of their disease. However, this knowledge is currently limited in these patients and physicians are currently not always capable of sufficiently providing them this knowledge.
Our findings represent a major area for improvement in our current practice of congenital cardiac care and provides the potential to substantially improve outcome in these patients.16–18 23–28 Better informed and more activated patients have been found to be associated with improved quality of life, treatment adherence, health behaviour and clinical outcome and also with more efficient healthcare utilisation and lower healthcare costs.6–19 Furthermore, improved information and knowledge may provide patients the confidence and reassurance of knowing what to expect and when and how to act, thereby reducing anxiety.
This underlines the urgent need for innovative solutions in more effectively informing our patients and their parents. A platform easily accessible to users at all times, such as an online information portal, presents promising opportunities. This would ideally allow for a dynamic environment in which information can be tailored to patients’ information needs and their specific disease state. To ensure quality, reliability and acceptance among patients/parents and physicians alike, patient information should be evidence-based and endorsed, supported and actively used by physicians. Furthermore, the content of patient information should not only be focused on medical topics should be tailored to the information needs expressed by patients/parents, which are often broader than expected, as evidenced by our results. Special attention should be paid to the specific needs of different user groups, for instance, patients’ parents, teenage patients, adult patients and relatives. The information should also be formatted to be comprehensible and attractive to users of a wide variety in education level, health literacy and numeracy. In light of our findings of limited numeracy among patients and parents, further research should also focus on how the comprehensibility of patient information can be improved and should explore the effectiveness of supporting tools such as illustrations, animations, risk visualisations and virtual reality. Furthermore, it remains unclear how improved patient knowledge affects anxiety and uncertainty. Further investigation may provide insight into how we may best inform patients/parents to also provide them the reassurance they often need, thereby reducing anxiety. Last, how improved patient information and knowledge relates to patient activation, involvement and concordance of treatment decisions with patient values remains to be elucidated.
Limitations
As this was a Dutch study in which patients/parents were recruited from a single centre, possible international differences in medical practice, culture and language as well as interinstitutional practice variation should be taken into consideration, although our findings are in line with prior studies in other centres and countries.16–18 23–28 Our disease-specific knowledge questionnaire was only aimed at capturing the most basic knowledge of disease, and the level of more in-depth disease-specific knowledge among these subjects remains to be elucidated. Regarding questions about patient/parent personal experiences with decision-making, the time between surgery and survey may have given rise to recall bias. Results may differ for disease states other than aortic and pulmonary valve surgery, which should be taken into account when interpreting our results. The limited sample size did not allow for analysis of the effects of gender, age and prosthesis type. Lastly, as this was a survey, response bias may have had an influence on our results.
Conclusion
Patients, parents and physicians alike experience important shortcomings in patient information and decision-making in congenital aortic and pulmonary valve surgery. Patient knowledge is severely limited due to the limited availability, reliability and comprehensibility of patient information. Furthermore, the provided information often does not meet the patients’ information needs. This may be associated with our findings of suboptimal patient activation and involvement and substantial decisional conflict and valve-related anxiety. This underlines the need for innovative solutions, such as careful implementation of patient information tools and shared decision-making in the care path.
References
Footnotes
Presented at Presented at the Scientific Meeting of the Heart Valve Society, 17–19 March 2016, New York City and at the Annual North American Meeting of the Society for Medical Decision Making, 23–26 October 2016, Vancouver.
Contributors All authors have made substantial contributions to all of the following: (1) the conception and design of the study or acquisition of data or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, (3) final approval of the version to be submitted.
Funding This work was supported by the Dutch Heart Foundation (2013T093).
Competing interests None declared.
Patient consent Not required.
Ethics approval Erasmus University Medical Center Medical and Ethical Review Committee.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement No additional data are available.