Article Text

Abstract
Objective Postmarketing observational studies report that a substantial percentage of patients with atrial fibrillation (AF) receive a reduced non-vitamin K antagonist oral anticoagulant (NOAC) dose without a clear indication. Recently, increasing evidence has become available to explore the clinical consequences of such off-label reduced dosing (OLRD). This study aims to systematically review and meta-analyse observational studies that report clinical outcomes associated with OLRD of NOACs compared with on-label non-reduced dosing (OLNRD) of NOACs in patients with AF.
Methods and analysis We performed a systematic literature review and meta-analysis of observational studies reporting clinical outcomes in AF patients with OLRD of an NOAC compared with AF patients with OLNRD of an NOAC. Using random effects meta-analyses, we estimated the risk of stroke/thromboembolism, bleeding and all-cause mortality.
Results We included 19 studies with a total of 170 394 NOAC users. In these studies, the percentage of OLRD among patients with an indication for an on-label non-reduced NOAC dose ranged between 9% and 53%. 7 of these 19 studies met the predefined criteria for meta-analysis (n=80 725 patients). The pooled HR associated with OLRD of NOACs was 1.04 (95% CI 0.83 to 1.29; 95% prediction interval (PI) 0.60 to 1.79) for stroke/thromboembolism, 1.10 (95% CI 0.95 to 1.29; 95% PI 0.81 to 1.50) for bleeding and 1.22 (95% CI 0.81 to 1.84; 95% PI 0.55 to 2.70) for all-cause mortality.
Conclusion This meta-analysis shows no statistically significant increased risk of stroke/thromboembolism, nor a decreased bleeding risk, nor a difference in risk of all-cause mortality in patients with OLRD of NOACs. Future research may focus on differences between NOACs.
- Atrial Fibrillation
- Epidemiology
- Pharmacology, Clinical
- Meta-Analysis
- Systematic Reviews as Topic
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information. The statistical code and full dataset are available from the corresponding author at S.vanDoorn@umcutrecht.nl.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Postmarketing studies reported that many patients with atrial fibrillation receive a reduced dose of non-vitamin K antagonist oral anticoagulants (NOACs) without a clear indication.
To what extent patients experience clinical consequences of such off-label reduced dosing (OLRD) is not yet known.
WHAT THIS STUDY ADDS
While other studies have compared patients with OLRD to patients with on-label dosing (ie, both on-label reduced and on-label non-reduced), we compared OLRD to on-label non-reduced dosing (OLNRD), which is clinically the most relevant comparison.
Our systematic review and meta-analysis showed that there is no statistically significant increased risk of stroke/thromboembolism, nor a decreased bleeding risk, nor a difference in risk of all-cause mortality in patients with OLRD of NOACs compared with OLNRD of NOACs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study summarises all observational studies on the clinical outcomes of OLRD of NOACs, thereby informing clinicians that they, in close discussion with their patients, should decide on the best treatment regimen in the specific situation of each patient.
Introduction
Oral anticoagulants are of critical value for stroke prevention in atrial fibrillation (AF). Despite the effectiveness of the oldest form of anticoagulation, vitamin K antagonists (VKAs), studies have repeatedly shown that historically patients with AF often do not receive anticoagulants or antiplatelet therapy instead. Such ‘underuse’ of anticoagulants in patients with AF at high risk of stroke was in the order of 50%.1 With the introduction of non-VKA oral anticoagulants (NOACs) in 2009, underuse of anticoagulants for AF decreased considerably given that randomised trials showed that NOACs are at least as effective as VKAs, have fewer drug and food interactions, and overall a lower risk of serious bleeding, notably intracranial bleeds.2 Moreover, NOACs do not require INR monitoring; a fixed dose can be used.3 Currently, four NOACs have been approved for patients with AF,4–8 and these agents rapidly became recommended as first-line agents for most AF patients in clinical guidelines. While this initially alleviated the concerns about ‘underuse’ of anticoagulants, a new pitfall has arisen. For each NOAC, besides a non-reduced dose, a reduced dose is available for specified subgroups of patients. However, accrual of postmarketing evidence showed that many patients (in the order of 20%–30%) receive a reduced NOAC dose without any clear indication, likely to mitigate a presumed high risk of bleeding.9–14 This so-called ‘off-label reduced dosing’ (OLRD) may put patients in need of oral anticoagulants at unnecessary risk of thromboembolism, while the anticipated attenuation of bleeding risk may in fact be negligible, or at least does not justify this OLRD.15
Several systematic reviews have evaluated the clinical consequences of such OLRD.14 16–18 However, the included studies in these reviews are highly heterogeneous, suffer from confounding and/or compare patients with OLRD to all patients receiving an on-label dose (ie, both on-label reduced and on-label non-reduced). A more clinically relevant comparison is the comparison of OLRD to on-label non-reduced dosing (OLNRD) only. After all, clinicians wonder what happens if they reduce the dose in patients who are presumed to be at high risk of bleeding (ie, the most common incentive for clinicians to opt for OLRD of NOACs), but who do not formally meet the dose reduction criteria and should, therefore, receive an on-label non-reduced NOAC dose. We; therefore, systematically reviewed all observational studies that report clinical outcomes associated with OLRD of NOACs compared with OLNRD of NOACs in patients with AF and estimated the risk of stroke/thromboembolism, bleeding and all-cause mortality performing meta-analyses only in studies meeting predefined criteria (in order to reduce the impact of confounding).
Materials and methods
Search strategy
We performed a systematic search to identify all observational studies reporting on clinical outcomes associated with OLRD of NOACs for stroke prevention in AF patients from 1 January 2009 to 10 July 2022. We searched PubMed and Embase using search terms for ‘dose reduction’ and ‘NOAC’, including synonyms and MeSH headings where appropriate, and without language restrictions. For the full search syntax, see online supplemental file 1.
Supplemental material
Definitions and study selection
We defined OLRD of NOACs as the use of an NOAC dose lower than the recommended on-label non-reduced NOAC dose in absence of a clear indication for dose reduction as formulated either by the Summary of Product Characteristics (SPC),19–22 the Food and Drug administration (FDA),23–26 the European Society of Cardiology (ESC),27 the European Heart Rhythm Association (EHRA),28 the landmark NOAC trials5–8 (see table 1) or other guidelines. Clinical outcomes under consideration were stroke/thromboembolism (defined as (ischaemic) stroke and/or transient ischaemic attack (TIA) and/or thromboembolism), bleeding (defined as (major) bleeding), all-cause hospitalisation, all-cause mortality and major adverse clinical events (MACE) (defined as cardiovascular mortality, and/or myocardial infarction, and/or a composite of cardiovascular diseases, such as stroke/thromboembolism and bleeding).
Indications for dose reduction of NOACs used for stroke prevention in atrial fibrillation patients
We selected all original observational studies on stroke prevention in patients with AF without a mechanical heart valve and/or severe mitral valve stenosis, describing the use of any of the registered NOACs (ie, dabigatran, rivaroxaban, apixaban and/or edoxaban), and presenting data on clinical outcomes of treatment with an off-label reduced NOAC dose compared with treatment with the on-label (ie, the recommended) non-reduced NOAC dose. We excluded studies including patients below the age of 18 years or including patients with venous thromboembolism (unless it was possible to analyse AF patients separately), and studies in highly selected patient populations (eg, patients with a highly specific age, only patients with cancer, severe kidney disease, obesity or COVID-19, or those on haemodialysis or after major surgery or arrhythmia surgery). Four reviewers (LJ, RvM, CJvdD and SvD) independently screened the total of selected articles based on title and abstract in duplicate and resolved any uncertainties by discussion. Of all potential studies, three reviewers (LJ, RvM and SvD) independently evaluated the full text for eligibility in duplicate and resolved any disagreements by discussion. Reasons for exclusion were recorded. For each included study, the reference list was evaluated for any additional relevant studies.
Critical appraisal and risk of bias assessment
Three reviewers (LJ, RvM and SvD) critically appraised all included studies and independently performed a risk of bias assessment in duplicate using the Newcastle-Ottawa quality Scale (NOS) for cohort studies29 supplemented by an item for handling missing data (see online supplemental file 2), and resolved any disagreements by discussion.
Data extraction
From each included study, three reviewers (LJ, RvM and SvD) extracted (1) study and patient characteristics (see online supplemental file 3), (2) the absolute number of patients receiving an off-label reduced NOAC dose and the absolute number of patients receiving the on-label non-reduced NOAC dose and (3) the exact definition of each clinical outcome (stroke/thromboembolism, bleeding, all-cause hospitalisation, all-cause mortality and MACE), its associated relative risk for OLRD compared with OLNRD (stratified by dabigatran, rivaroxaban, apixaban and edoxaban if possible) and the method used to adjust for confounding.
Data analyses
First, we described the results of the systematic search, the main study and patient characteristics, and the results of risk of bias assessment. We calculated the percentage of patients with OLRD of NOACs as the number of patients with OLRD relative to the total number of patients with an indication for an on-label non-reduced NOAC dose (ie, the sum of patients receiving OLRD and OLNRD).
Finally, where possible, we meta-analysed studies meeting predefined criteria. Foremost, observational studies often suffer from confounding (ie, factors that influence both the use of OLRD and the risk of adverse clinical outcomes) that should always be taken into account in the analyses. Patients who receive a reduced dose without a clear indication do so for a reason. Therefore, only studies that aimed to reduce the impact of this confounding by indication by applying propensity scoring methods (for at least sex and age) in the analyses of all predefined clinical outcomes in relation to OLRD of NOACs and by reporting an HR were included in the meta-analysis, if in addition the risk of bias was low in the representativeness of the exposed and non-exposed cohort (ie, both awarded with a star according to the NOS) and appropriate guidelines (ie, SPC, FDA, ESC, EHRA or landmark NOAC trial(s)) to determine whether a non-reduced or a reduced NOAC dose is indicated were used. Assuming heterogeneity among studies, we applied random effects meta-analysis of the log transformed HRs using restricted maximum likelihood estimation. We calculated 95% CI by using the Hartung-Knapp-Sidik-Jonkman method.30 Between-study heterogeneity was expressed by the 95% prediction interval (95% PI). This interval indicates the range of occurrence of a specific clinical outcome within patients receiving an off-label reduced NOAC dose that can be expected in future observational studies with similar characteristics as those included in our review.
We performed analyses in R V.1.3.1093,31 with the package ‘metaphor’ V.3.4–0.32
Results
Systematic search
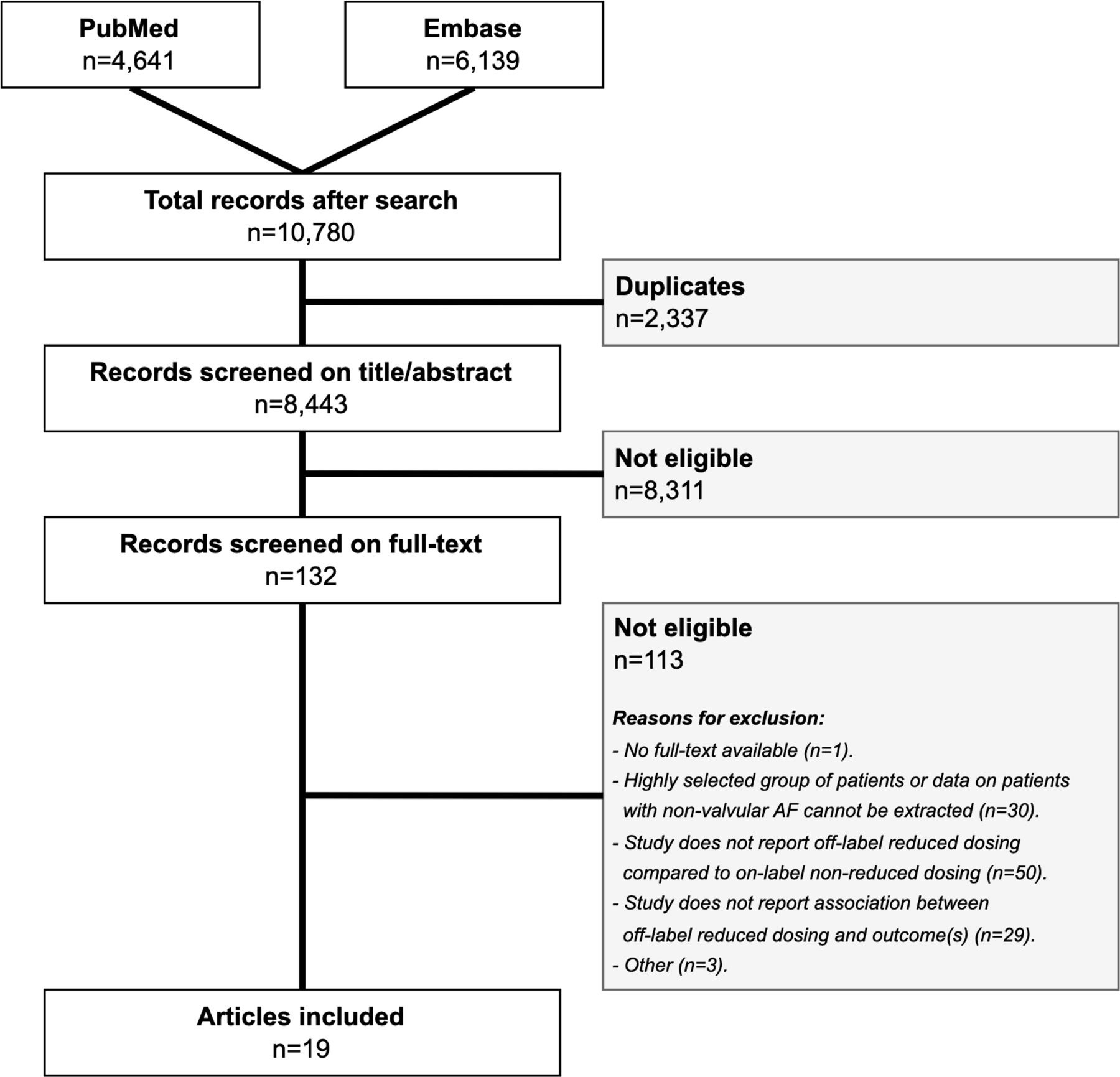
The results of the systematic search are shown in figure 1. The initial search in PubMed and Embase yielded 10 780 records of which we removed 2337 duplicates. Title and abstract screening of the remaining 8443 records resulted in the selection of 132 records. After assessment of the full text, eligibility criteria were met in 19 articles. For an overview of the excluded studies based on full-text screening, including reason for exclusion, see online supplemental file 4. No additional relevant studies were found. Eventually, 19 studies were included in the current systematic review.33–51
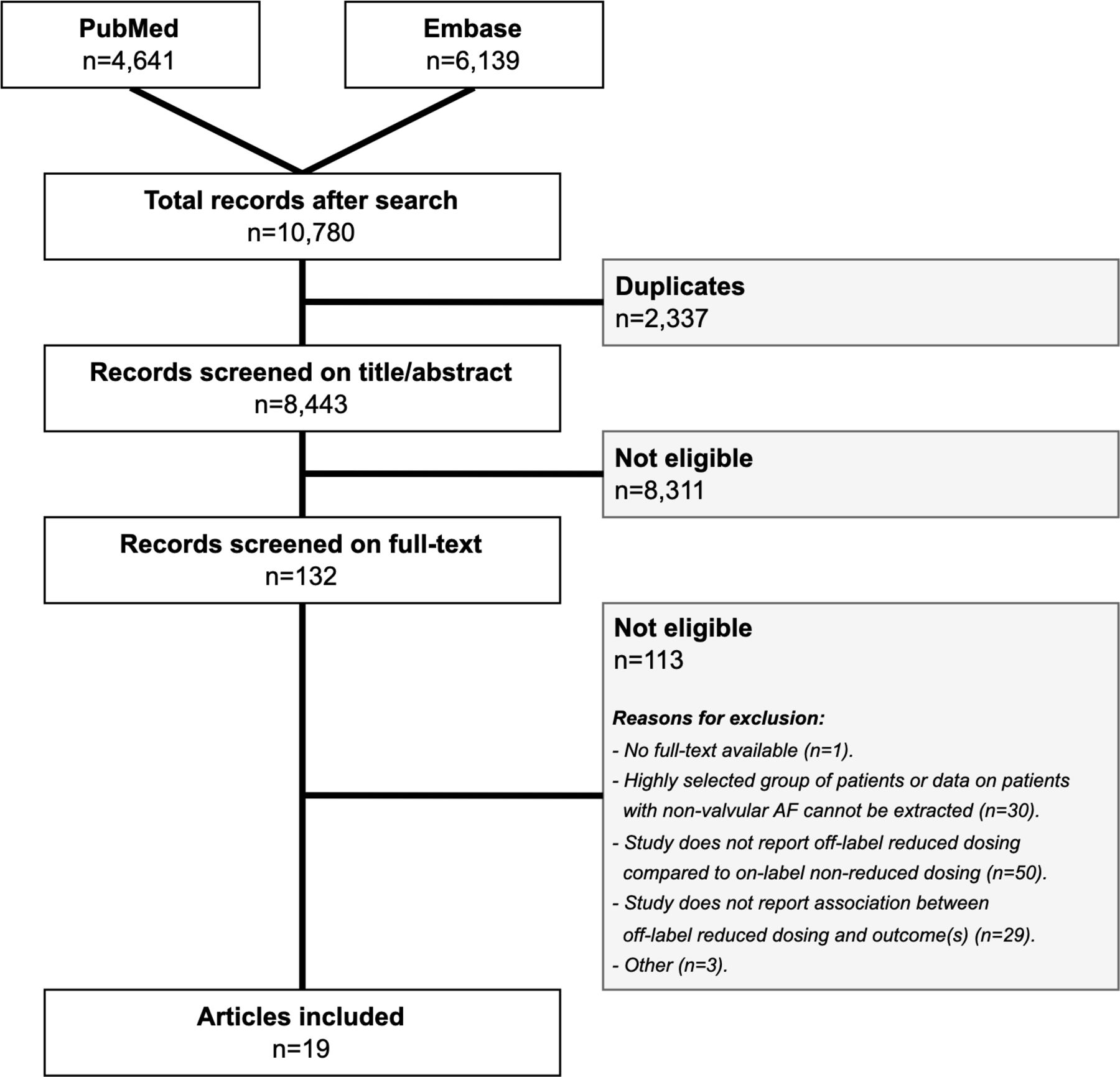
Flow chart with the results of the systematic search. AF, atrial fibrillation.
Study and patient characteristics of all included studies
The 19 included original observational studies, involving 170 394 NOAC-users, showed data from October 2010 to December 2017. The majority of the studies were carried out in Asian countries (most notable in Japan (n=8) and Korea (n=4)) and in the USA (n=4), and showed data on rivaroxaban (n=7), apixaban (n=7), dabigatran (n=4) and edoxaban (n=1). Duration of follow-up ranged from a median of 4.0 months to a median of 39.3 months.
The percentage of male sex ranged from 47.4% to 78.0%; the mean age of study populations ranged from 67.2 to 78.7 years. Overall, hypertension was the most common reported comorbidity, ranging from 54.0% to 95.4%. The percentage of patients with a history of (ischaemic) stroke (and TIA and/or thromboembolism) ranged from 5.9% to 49.8%. The percentage of OLRD ranged from 8.9% to 53.0%. A detailed overview of all extracted study and patient characteristics can be found in online supplemental file 5.
Risk of bias assessment
An overview of the risk of bias assessment can be found in online supplemental file 6. In general, all studies scored well on the selection, comparability and outcome category of the NOS, except for demonstrating that the outcome of interest was not present at the start of the study and adequacy of follow-up of the cohorts.42 Three out of 19 studies reported on the handling of missing data, all using multiple imputation.
Meta-analysis of clinical outcomes associated with OLRD of NOACs
Seven studies met the predefined criteria for meta-analysis (n=80 725) (see online supplemental file 7).34 35 37 43 46 47 50 The percentage of OLRD in these studies ranged from 9.6% to 53.0%. The pooled HR associated with OLRD of NOACs in AF patients was 1.04 (95% CI 0.83 to 1.29; 95% PI 0.60 to 1.79) for stroke/thromboembolism, 1.10 (95% CI 0.95 to 1.29; 95% PI 0.81 to 1.50) for bleeding and 1.22 (95% CI 0.81 to 1.84; 95% PI 0.55 to 2.70) for all-cause mortality (figure 2). Of studies meeting our criteria for meta-analysis no study reported on all-cause hospitalisation, and only two studies reported on MACE, (HR of 1.2 (95% CI 1.05 to 1.37) and 1.4 (0.94 to 2.1).43 47

{kind=link}
{kind=link}
Meta-analyses in atrial fibrillation patients with off-label reduced dosing of an NOAC versus on-label non-reduced dosing of an NOAC. (A) With outcome (ischaemic) stroke (and TIA and/or thromboembolism). (B) With outcome bleeding. (C) With outcome mortality. *Year=starting date of inclusion of patients. NOAC, non-vitamin K antagonist oral anticoagulant; OLRD, off-label reduced dosing; PI, prediction interval; TIA, transient ischaemic attack.
When also including studies that used multivariate regression to adjust for confounding, we could meta-analyse one additional study that did not change our results (data not shown).33
Discussion
In this systematic review and meta-analysis of observational studies, we found no statistically significant increased risk of stroke/thromboembolism, nor a decreased bleeding risk, nor a difference in risk of all-cause mortality in patients with OLRD compared with OLNRD of NOACs.
The effect of OLRD of NOACs
Although all point estimates in our meta-analysis lie above 1, indicating a possible harmful effect, it cannot be concluded from our meta-analysis that OLRD of NOACs overall in fact is harmful, not to mention beneficial. However, it should be realised that NOACs differ. First, plasma levels may be more stable for some NOACs than for others due to once daily (rivaroxaban and edoxaban) versus two times daily (dabigatran and apixaban) dosing. Second, NOACs vary in the percentage by which the dose should be reduced (50% for apixaban and edoxaban; 25%–33% for dabigatran and rivaroxaban). Finally, some NOACs have more extensive dose reduction criteria than others, which might suggest that OLNRD of NOACs with more extensive dose reduction criteria is more tailored to the individual patient and that OLRD of these NOACs might cause more harm. This may explain why data in our study suggest a harmful effect of OLRD specifically for apixaban (of the apixaban studies, almost all HRs for stroke/thromboembolism, bleeding and all-cause mortality are above 1). However, we cannot confirm this, because there were not sufficient studies meeting our inclusion criteria for meta-analysis stratified by the four different NOACs.
Comparison with existing literature
In a recent meta-analysis, Caso et al compared OLRD to on-label dosing (ie, both on-label reduced and on-label non-reduced). This showed that OLRD increased the risk of all-cause mortality (HR 1.28 (95% CI 1.10 to 1.49)) with a null effect on major bleeding (HR 1.04 (95% CI 0.90 to 1.19)).18
In another previous meta-analysis, the authors also compared OLRD to, again, on-label dosing and used less stringent inclusion criteria, which allowed them to include more studies and examine each NOAC separately. This showed that OLRD of rivaroxaban may increase the risk of stroke/thromboembolism (HR 1.31 (95% CI 1.05 to 1.63)) compared with on-label dosing of rivaroxaban, whereas OLRD of apixaban may increase the incidence of all-cause mortality (HR 1.21 (95% CI 1.05 to 1.40)) compared with on-label dosing of apixaban. They reported no differences in outcomes when comparing OLRD versus on-label dosing of dabigatran and edoxaban.16
A third meta-analysis combined the four NOACs in their analyses and showed higher risk of stroke/systemic embolism (risk ratio (RR) 1.24 (95% CI 1.14 to 1.35)) without a reduction in bleeding risk (RR 1.18 (95% CI 0.91 to 1.53)) and a higher risk of all-cause mortality (RR 1.58 (95% CI 1.25 to 1.99)) in patients with OLRD compared with on-label dosing. However, this meta-analysis largely lacked measures to prevent confounding. Moreover, it also compared OLRD to on-label dosing (ie, both on-label reduced and on-label non-reduced) instead of comparing OLRD to OLNRD as we did.17
In contrast to these previous studies, we did not find an increased risk for all-cause mortality in patients with OLDR. The most obvious explanation could be the comparison we choose. Unlike previous meta-analyses, we restricted our included studies to those comparing OLRD to OLNRD. This is the most clinically relevant comparison, as it represents the patient groups—those without an indication for dose reduction—in whom clinicians face a dosing dilemma most often.
Strengths and limitations
This selection of studies comparing OLDR only with OLNRD is the major strength of our study. Second, we tried to minimise the influence of confounding by indication as best as possible by including only studies meeting predefined criteria, including applying propensity scoring methods. Finally, we conducted a very comprehensive and thorough search which resulted in a large sample size.
Limitations of our study are: (1) the inclusion of a predominantly Asian population who has shown to have different pharmacokinetics, meaning that our results cannot be generalised on a one-to-one basis to, for example, the Western population; (2) the fact that we could not include enough studies to stratify by NOAC in the meta-analysis; (3) risks of misclassification within studies (eg, when an NOAC dose has been changed by a cardiologist but is not yet recorded in the general practitioner’s file, while the latter has been requested by the study) and significant heterogeneity between studies (eg, in the duration of follow-up (with a median ranging from 4 to 24 months in our meta-analyses)) which is both inherent to using data from observational studies and(4) conducting our research at study level rather than at patient level (as we did not have data on individual patient level).
Clinical implications and areas for future research
Choosing an NOAC dose is all about balancing stroke risk against bleeding risk. Our results indicate that the risk of stroke may not be increased while the risk of bleeding may not be decreased in patients that are prescribed OLRD of NOACs compared with patients with OLNRD of NOACs. This may be considered as an argument to adhere to prescription guidelines in most, if not all, patients. However, our results may also indicate that OLRD of NOACs may not be harmful in specific cases. Physicians, in close discussion with their patients, may use our findings to decide on the treatment regimen in the specific situation of each patient. Future research may focus on these situations and, and perhaps more importantly, on differences between NOACs.
In conclusion, this systematic review and meta-analysis shows that there is no statistically increased risk of stroke/thromboembolism, nor a decreased bleeding risk, nor a difference in risk of all-cause mortality in patients with OLRD of NOACs compared with patients with OLNRD of NOACs. Future research may focus on differences between NOACs.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information. The statistical code and full dataset are available from the corresponding author at S.vanDoorn@umcutrecht.nl.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LJ, RvM, CJvdD, G-JG and SvD conceived and designed this study. LJ, RvM, CJvdD and SvD screened and selected the articles for inclusion. LJ, RvM and SvD performed the data extraction and risk of bias assessment. SvD performed statistical analyses. All authors contributed to the interpretation of the results. LJ, RvM and SvD wrote the first manuscript draft and subsequent revisions. All authors critically revised the manuscript and gave final approval. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. Transparency: The lead author (the manuscript’s guarantor) affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Funding This study did not receive specific funding, but G-JG is supported by a VENI and VIDI grant from the Netherlands Organisation for Health Research and Development (ZonMw numbers 016.166.030 and 016.196.304).
Disclaimer This funder had no role in considering the study design or in the collection, analysis, interpretation of data, writing of the report, or decision to submit the article for publication.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/. FR, MH and G-JG report unrestricted institutional grants for performing research in the field of atrial fibrillation from Boehringer-Ingelheim, Bayer Healthcare, BMS Pfizer and Daiichi Sankyo. CBG reports personal fees from Bayer Healthcare and Boston Scientific; grants and personal fees from Boehringer-Ingelheim, BMS Pfizer and Janssen; and grants from Daiichi-Sankyo during the conduct of the study; personal fees from AbbVie, Espero, Medscape, Medtronic, Merck, the National Institutes of Health, Novo Nordisk, Roche, Rho Pharmaceuticals, CeleCor, Correvio, Philips, Abiomed and Anthos Therapeutics; grants from Akros, AstraZeneca, the US Food and Drug Administration, Glaxo Smith Kline, Medtronic Foundation and Apple; and grants and personal fees from Novartis and The Medicines Company outside the submitted work. SvD reports an unrestricted research grant from Stoffels Hornstra. All other authors (LJ, RvM, CJvdD and AWH) declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear tohave influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.