Article Text

Abstract
Objectives Determine whether an ultrathin biodegradable polymer sirolimus-eluting stent (‘Orsiro’—BP-SES) has clinical benefits over second-generation durable polymer drug-eluting stents (DP-DES).
Methods We conducted a prospective systematic review and meta-analysis of randomised clinical trials comparing Orsiro BP-SES against DP-DES (PROSPERO Registration: CRD42019147136). The primary outcome was target lesion failure (TLF): composite of cardiac death, target vessel myocardial infarction (TVMI) and clinically indicated target lesion revascularisation (TLR)) evaluated at the longest available follow-up.
Results Nine trials randomised 11 302 patients to either Orsiro BP-SES or DP-DES. At mean weighted follow-up of 2.8 years, the primary outcome (TLF) occurred in 501 of 6089 (8.2%) participants with BP-SES compared with 495 of 5213 (9.5%) participants with DP-DES. This equates to an absolute risk reduction of 1.3% in TLF in favour of Orsiro BP-SES (OR 0.82; 95% CI 0.69 to 0.98; p=0.03). This was driven by a reduction in TVMI (OR 0.80; 95% CI 0.65 to 0.98; p=0.03). There were no significant differences in other clinical endpoints: cardiac death, TLR and stent thrombosis.
Conclusion The Orsiro BP-SES shows promising clinical outcomes in patients undergoing percutaneous coronary intervention compared with contemporary second-generation DES at a short to medium term follow-up. More research is warranted to evaluate performance over a longer follow-up period and in different clinical and lesion subsets.
- coronary artery disease
- interventional cardiology
- coronary intervention (PCI)
- coronary stenting
- acute coronary syndrome
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- coronary artery disease
- interventional cardiology
- coronary intervention (PCI)
- coronary stenting
- acute coronary syndrome
Key questions
What is already known about this subject?
Recent randomised trials support non-inferiority of Orsiro ultrathin-strut biodegradable polymer sirolimus-eluting stent (BP-SES) compared with contemporary durable polymer drug-eluting stents (DP-DES).
What does this study add?
Patients randomised to percutaneous coronary intervention with Orsiro ultrathin-strut BP-SES had almost one-fifth less target lesion failure compared with contemporary DP-DES at mean follow-up of 2.8 years. This was largely due to a significant reduction in target vessel myocardial infarction. There were no differences in other clinical and safety endpoints between the two group: cardiac death, target lesion revascularisation and stent thrombosis.
How might this impact on clinical practice?
Ultrathin-strut BP-SES designs may further improve clinical outcomes over contemporary second-generation durable polymer DES. Future research is warranted with more randomised trials powered to compare modern generation stent platforms focusing on utility in different patient subgroups.
Introduction
Contemporary second-generation durable polymer drug-eluting stents (DP-DES) have proven safety resulting in excellent clinical outcomes following percutaneous coronary intervention (PCI).1 2 Historical concerns from first-generation DES regarding the effects of durable polymer on delayed vessel healing and peristrut inflammation drove stent iterations incorporating biodegradable polymer sirolimus-eluting stents (BP-SES) with thinner struts.3 4 Indeed, thinner stent strut designs have recently been shown to reduce in-stent restenosis and target lesion revascularisation (TLR) in a pooled meta-analysis.5
The Orsiro BP-SES (BIOTRONIK, Buelach, Switzerland) has gained significant traction as one such ultrathin strut (60 µm in stents <3.0 mm diameter) sirolimus-eluting stent with a large clinical evidence base in contemporary studies.4 6–8 Many studies have shown non-inferiority of the Orsiro when compared with DP-DES, however, recent data from BIOFLOW V and BIOSTEMI studies support lower target lesion failure (TLF) in patients randomised to the Orsiro BP-SES over DP-DES.9 10 In light of the evolving evidence base, we performed a prospective meta-analysis of randomised controlled trials (RCTs) comparing Orsiro BP-SES versus DP-DES.
Methods
The data, analytical methods and study materials have been made available to other researchers for the purposes of reproducing the results or replicating the procedure. The full study protocol was registered with the International Database of Prospectively Registered Systematic Reviews in Health and Social care (PROSPERO—CRD42019147136) and data is made available within this manuscript. This study was performed according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines.11 Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Eligibility criteria
The inclusion criteria for the studies in our meta-analysis were as follows: RCTs comparing the Orsiro ultrathin strut, biodegradable polymer, sirolimus-eluting stents versus durable polymer second-generation drug-eluting stents, irrespective of the specific antiproliferative drug, with the availability of clinical or angiographic follow-up. Data on TLF had to be available in the publication or authors were approached for this data. Publications were excluded if they only compared two biodegradable polymer stents to each other and, for the biodegradable arm, were non-sirolimus eluting or had a strut other than an ultrathin strut. To minimise heterogeneity, we included only the studies that used the Orsiro BP-SES. Non-randomised trials, publications not in English and those with outcomes of interest less than 12 months follow-up were excluded.
Quality assessment
Two reviewers (CFS and MP) independently performed the risk-of-bias assessment of the included trials using the Cochrane Collaboration framework: bias arising from the randomisation process, bias due to deviation from intended intervention, bias due to missing outcome data, bias in measurement of the outcome and bias in selection of the reported results. Discrepancies were resolved by consensus with a third independent reviewer (TF). The risk-of-bias summary according to the risk-of-bias tool of the Cochrane collaboration framework is provided (figure 1). We planned to assess publication bias according to funnel plot asymmetry using standard error as the measure of study size and OR of treatment effect if we yielded over 10 studies.12

Risk-of-bias summary for trials included in the meta-analysis.
Search strategy
A systematic search of online databases of PubMed, EMBASE and Cochrane Central Register of Controlled Trials was performed until 26 August 2020. Peer-reviewed RCTs were selected using combinations of keywords, and their variations, pertinent to our intervention of interest and comparison with ‘biodegradable polymer’, ‘drug-eluting stent’, ‘sirolimus’, ‘orsiro’, ‘durable polymer’, ‘everolimus’ and ‘zotarolimus’. Two reviewers (MRM and CFS) independently screened abstracts against the inclusion and exclusion criteria while reference lists of relevant articles and previous meta-analyses were reviewed to identify other relevant studies. They then screened the full text of potentially relevant trials. Disagreements were resolved by consensus involving a third reviewer (PB). Conference abstracts from major cardiology scientific sessions were searched for completeness.
Outcomes and definitions
The primary outcome was TLF. TLF was defined as a composite index of cardiac death, target vessel myocardial infarction (TVMI) and clinically indicated TLR. Secondary outcomes included cardiac death, TVMI, clinically indicated TLR and definite or probable stent thrombosis (ST). Definite or probable ST was determined according to the academic research consortium definition.13 Outcomes data were extracted by two independent authors (MRM and RS). Differences in opinion were resolved by consensus involving a third reviewer (TF).
Data and statistical analysis
Follow-up duration was calculated as mean weighted duration according to study size. Pooled mean data were used to compare procedural aspects between the groups using an unpaired t-test. The study hypothesis was prespecified and tested with a two-tailed alpha of 0.05.
The statistical analysis was performed using R V 4.0 using the metaphor package14 and RevMan V 5.3.5 (the Cochrane Collaboration). Analyses for all outcomes were done on an intention-to-treat basis. The random-effects method was selected on account of inherent heterogeneity related to the different types of stents and patient or lesion types enrolled. We also performed a fixed-effect (Mantel-Haenszel) approach for completeness. We summarised the estimate of effect incorporating the clinical outcomes as OR with 95% CIs for our dichotomous data. Prespecified meta-regression was performed to assess the interaction between acute coronary syndrome (ACS) presentation and the primary endpoint. A leave-one-out sensitivity analysis was performed by iteratively removing one study at a time to assess whether any single study was driving our findings. Heterogeneity testing with Higgins I2 was performed with a threshold of >50% taken as evidence of significant heterogeneity between studies.15 To assess the risk of type I and II errors, we conducted a trial sequential analysis (TSA) to calculate the required information size which is a summation of sample sizes from a given number of included trials, 5% overall type I error and power of 80%.16
Results
Study selection and characteristics
An initial search yielded 332 citations. Applying inclusion criteria defined in the methods, we evaluated 45 abstracts of which we assessed 26 full-text publications with the longest available follow-up. The search flow diagram can be found in figure 2. Nine randomised trials met the inclusion criteria and reported primary outcome of TLF follow-up of 12 months or greater.10 17–26

PRISMA flow chart for studies included in the meta-analysis. BP-EES, biodegradable polymer everolimus-eluting stent; DP-DES, durable polymer drug-eluting stents; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT, randomised controlled trial; SES, sirolimus-eluting stent.
All trials included were published between 2017 to 2020. Nine trials randomised 11 302 patients to either Orsiro BP-SES or DP-DES. The mean weighted follow-up for the included studies was 2.8±1.4 years (table 1). The DP-DES included everolimus-eluting stents (6 trials) and zotarolimus-eluting stents (3 trials). A total of 6089 patients were randomised to BP-SES strategy and 5213 patients to the DP-DES strategy. The mean age of the population was 64.2±1.0 years with baseline patient characteristics shown in table 2. Risk-of-bias and quality of evidence assessment is summarised in figure 1.
Baseline characteristics of included trials
Main baseline patient characteristics
Efficacy outcome: TLF
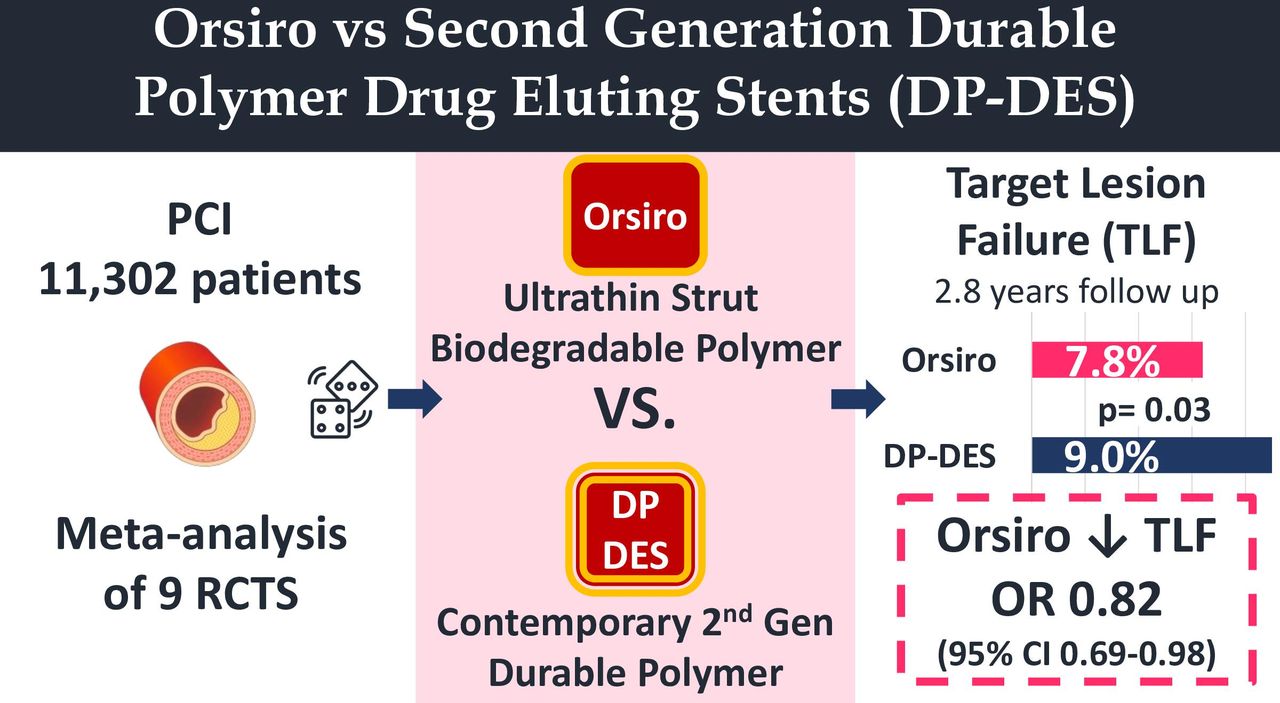
There was a statistically significant reduction in the primary outcome (TLF) among patients randomised to Orsiro BP-SES (501/6089 (8.2%)) compared with DP-DES (495/5213 (9.5%); OR 0.82; 95% CI 0.69 to 0.98; p=0.037). The outcomes from the analysis are summarised in table 3 and figure 3. Forrest plots are summarised in figure 4. Our findings remained significant using the Mantel-Haenszel fixed effects model (OR 0.86; 95% CI 0.75 to 0.98, p=0.02). The key findings of the study are provided in a visual summary (figure 5.
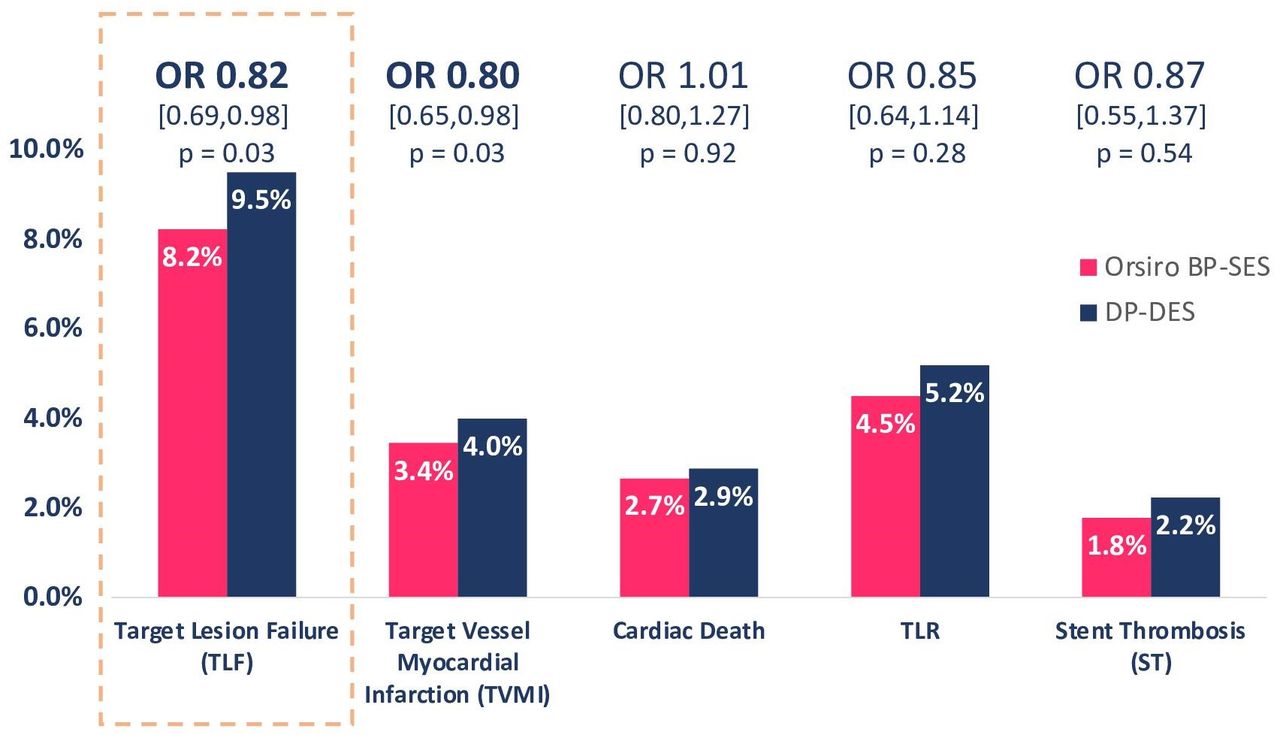
Target lesion failure and secondary end points. BP-SES, biodegradable polymer sirolimus-eluting stent; DP-DES, durable polymer drug-eluting stents; TLR, target lesion revascularisation.

Forest plots of primary outcome (A) and secondary outcomes (B–E) for Orsiro BP-SES versus DP-DES. BP-SES, biodegradable polymer sirolimus-eluting stent; DP-DES, durable polymer drug-eluting stents.

11 302 participants randomised across 9 RCTs between the Orsiro BP-SES and DP-DES groups showed a significant reduction in TLF in participants with the Orsiro BP-SES. BP-SES, biodegradable polymer sirolimus-eluting stent (Odds ratio 0.82; 95% CI 0.69-0.98; P=0.03); DP-DES, durable polymer drug-eluting stents; RCTs, randomised controlled trials; TLF, target lesion failure.
Odds ratios comparing clinical outcomes for Orsiro BP-SES and DP-DES
Safety endpoints: TVMI, cardiac death, TLR and ST
Safety endpoints were reported in all studies. TVMI occurred in 201 of 5832 participants (3.4%) randomised to the Orsiro BP-SES group and 203 of 5088 participants (4.0%) randomised to the DP-DES group. This was a statistically significant reduction in TVMI with BP-SES over DP-DES (OR 0.80; 95% CI 0.65 to 0.98; p=0.03). Other safety endpoints were not statistically different between the groups: Cardiac death (2.7% vs 2.9%; OR 1.01 (95% CI 0.80 to 1.27); p=0.92), clinically driven TLR (4.5% vs 5.2%; OR 0.85 (95% CI 0.64 to 1.14); p=0.28) and ST (1.8% vs 2.2%; OR 0.87 (95% CI 0.55 to 1.37); p=0.54).
Meta-regression
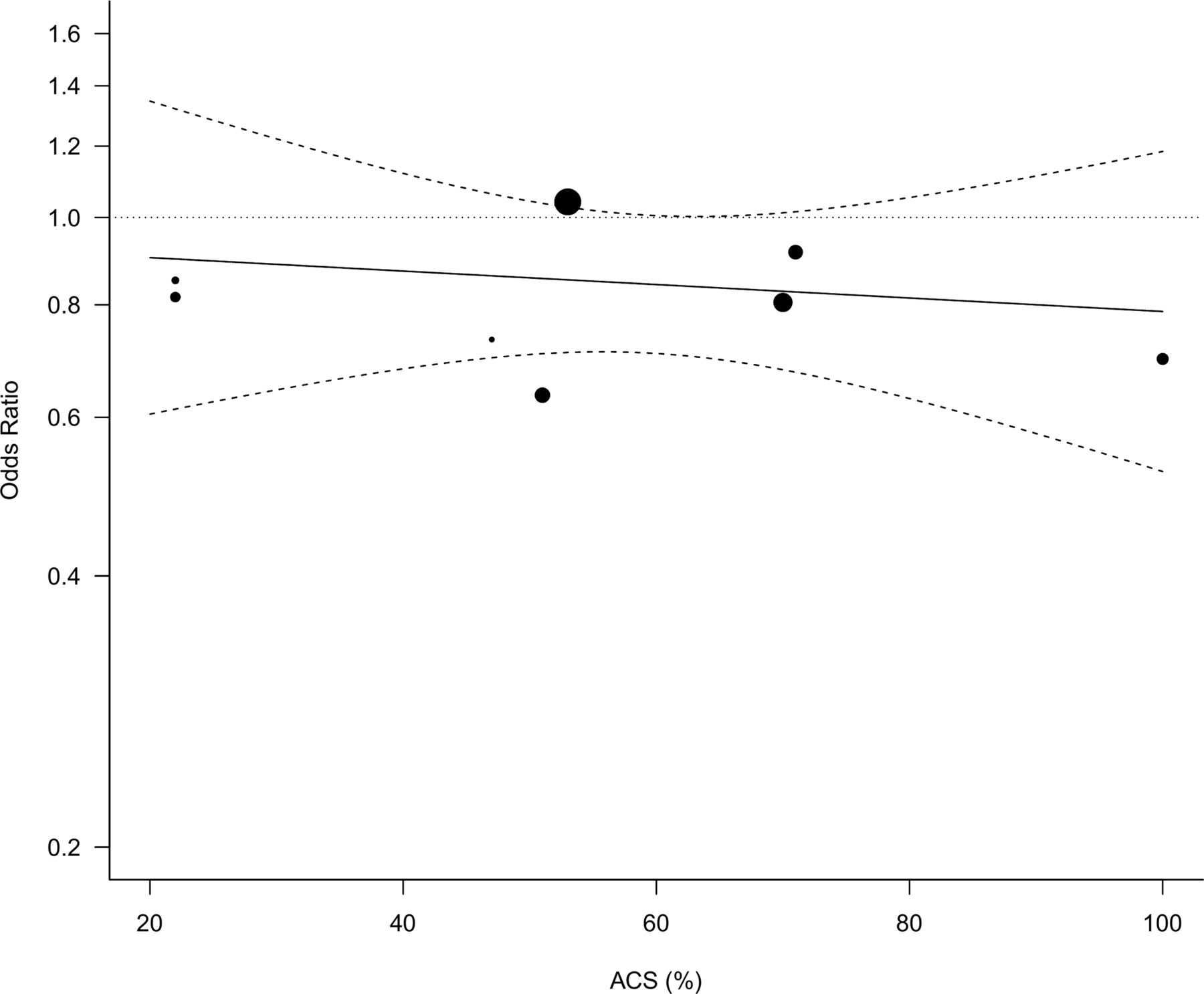
There was no statistically significant interaction between ACS and treatment effect (TLF) at study level between the groups (OR=0.983 (per 10% increase in ACS) (95% CI 0.898 to 1.077); p=0.626; figure 6)).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Interaction of ACS and treatment effect (TLF) at study level between BP-SES and DP-DES groups. ACS, acute coronary syndrome; BP-SES, biodegradable polymer sirolimus-eluting stent; DP-DES, durable polymer drug-eluting stents; TLF, target lesion failure.
Sensitivity analyses and TSA
Our findings for both leave-one-out sensitivity analyses and TSA are provided in the online supplemental appendix. Our sensitivity analysis showed that TLF remained significant after excluding BIOSCIENCE which reduced our pooled TLF by 10.4% (OR 0.773, 95% CI 0.646 to 0.926; p=0.005). Excluding any of the other studies resulted in an insignificant result between the two arms with the highest trend towards an increase in TLF of 7.1% after excluding BIOFLOW V (OR 0.912, 95% CI 0.787 to 1.058; p=0.223). The TSA, however, suggested more trials are needed to achieve the required power for a conclusive meta-analysis.
Supplemental material
Discussion
In this meta-analysis of randomised trials comparing the Orsiro BP-SES and contemporary DP-DES, we found TLF to be significantly lower in participants randomised to the Orsiro BP-SES at a weighted average follow-up of 2.8 years after PCI. There was a similar difference in TVMI but remaining clinical outcomes of cardiac mortality, clinically driven TLR and ST were similar between the two groups.
The most striking finding of reduction in TLF in favour of Orsiro BP-SES is noteworthy but requires careful consideration. Previous studies have reported similar directional trends without establishing statistical significance.6–8 However, the data from three recent trials (BIOSTEMI, BIOFLOW IV and BIOFLOW VI) and longer-term outcomes of trials (BIOFLOW II 5 years outcomes, BIOSCIENCE 5 years outcomes, BIO-RESORT 3 years outcomes, BIOFLOW V 3 years outcomes, ORIENT 3 years outcomes and BIONYX 2 years outcomes) together support a significant reduction in the odds of TLF for Orsiro BP-SES when compared with DP-DES (absolute risk reduction of 1.3%). This is driven predominantly by the significant reduction in TVMI in Orsiro BP-SES patients as the remaining components of the composite index were similar between groups. This may relate to potential advantages of ultrathin strut stents in the treatment of small vessel coronary artery disease (as suggested by subgroup analysis in BIO-RESORT) compared with its other attributes including the polymer location, degradation time of the polymer, the antiproliferation agent and the drug-elution kinetics.27
There are two possible stent factors which could explain our findings. The first and most pertinent stent factor that may explain reduction in TLF and TVMI is the ultrathin strut stent design of the ORSIRO stent. Both the DP-DES have thicker struts (XIENCE=81 µm and RESOLUTE=91 µm) compared with Orsiro BP-SES ‘ultrathin’ strut (60 µm in stents <3.0 mm in diameter and >80 µm in stents >3.0 mm). Previous meta-analysis looking at all-comer ultrathin strut stents versus DP-DES have hinted at benefit in favour of the ultra-thin strut design.5 Thinner struts lead to greater flexibility and deliverability but crucially may be less traumatic to the endothelium and reduce perivascular inflammation promoting better endothelial coverage. Furthermore, they may be less likely to disturb flow in side branches and may decrease stent thrombogenicity with reduced detrimental low shear stress forces post deployment.28 29 These beneficial effects of thinner struts are likely to be enhanced and more favourable in smaller vessels (BIO-RESORT- subgroup analysis).
Second, the reduction in TLF seen may be attributable to the more biocompatible biodegradable polymer. The biodegradable polymer matrix of poly-L lactic acid in the Orsiro BP-SES degrades after 12–24 months. While previous meta-analyses included studies with shorter term follow-ups, our mean follow-up was 2.8 years and six out of the nine studies in our TLF analysis reported outcomes at 24 months or more. This finding is novel and one provocative interpretation is reduction in TLF accrues related to better endothelialisation over the thinner struts assisted by polymer degradation.30 Concern about longer-term events with durable polymers are largely historical and were considered related to by-products of first generation DES polymer degradation implicated with immunogenicity and vascular inflammation.9 Crucially, however, no superiority has been noted in other trials of non-ultrathin BP SES versus DP-DES.31
TVMI reflects reinfarction of the stented vessel including both peri-procedural myocardial infarction and spontaneous myocardial infarction. From the data presented, it was impossible to distinguish between these important types of myocardial infarction. Recent debate in the cardiovascular community32 has highlighted the importance of distinguishing between procedural and spontaneous MI and this may have helped us to characterise further important differences between the groups. If the primary outcome difference was driven by periprocedural events then this is less meaningful for patient care given that spontaneous myocardial infarcts are more strongly linked with major adverse cardiovascular events (including death) compared with periprocedural myocardial infarctions.33 It is most likely that the ultrathin design of the Orsiro BP-SES (<3 mm) contributed to reduced periprocedural MI via reduced side branch coverage, rather than the biodegradable polymer, to result in the reduced TVMI, the primary driver of the superior TLF.5 34
Subgroup analysis of participants with ACS did not show any significant effect on TLF which may relate to a lack of power from use of study-level rather than individual patient level data. ACS patients should be identified as a key research group of interest given the BIOSTEMI study and inferences from directional trend in our meta-regression . BIOSTEMI and the STEMI subgroup in BIOSCIENCE trial both had a stronger trend towards reduced TLF in ACS which could signal benefit of thinner struts in the setting of prothrombotic milieu.
Although all studies which reported TLF demonstrated a numerical trend towards a reduction in TLF, the finding was driven predominantly by one study (BIOFLOW V). Our results contrast with previous meta-analyses that show no difference in TLF, or any of the secondary outcomes, between the Orsiro BP-SES and DP-DES.6 8 Our findings are, thus, novel and consistent with result of longer-term follow-up studies of Orsiro in addition to the recent BIOFLOW V trial.
Limitations
There are several limitations to this work. First, four of the trials had short 1-year follow-up. Whether the outcomes seen persist in the longer term after the complete degradation of the polymer is unknown. Second, our meta-analysis was limited to aggregate study-level comparison which provides a less comprehensive comparison than patient-level data. The latter would have increased the power to detect interaction of treatment effect according to key subgroups (ACS or small vessels). Our meta-regression analysis did not show an effect signal for ACS but was underpowered to provide a definitive conclusion on subgroups. A recent patient-level meta-analysis of four of the included trials (BIOFLOW II, BIOFLOW IV, BIOFLOW V and BIOSCIENCE) with 4480 patients showed a non-significant trend towards lower TLF in the Orsiro BP-SES.35 Third, it is important to note that the BIOSTEMI trial (n=1300) incorporated historical data of 407 patients with acute STEMI from the BIOSCIENCE trial and these patients could not be excluded from analysis in both data sets. Fourth, while our study demonstrated low heterogeneity when comparing clinical outcomes (I2=29%), there was lack of uniform data and reporting between the trials. Specifically, one study (PRISON IV) did not report TLF and our direct approach to the corresponding author for this information did not receive a response and hence this trial was not eligible forthe primary endpoint analysis. Fifth, although we performed a meta-regression on ACS status of participants, clinical events were infrequent in all studies, and hence caution should be applied when comparing subgroups. Finally, the absolute difference is small, with large numbers of patients needed to treat. These may be offset by real life challenges of the ultra-thin strut stent platforms including limited radiographic visibility and reduced radial stregnth and maximum diameter stent expansion limits.
Conclusion
In this meta-analysis comparing modern generation DES platforms, patients randomly assigned to PCI with the ultrathin-strut biodegradable polymer stent (Orsiro) had reduced risk of target lesion failure compared with contemporary durable polymer DES with thicker stent struts at mean follow-up of 2.8 years. This benefit was largely driven by reduced target vessel myocardial infarction and supports the clinical utility of ultra-thin strut stent designs. Additional well powered randomised clinical trials with long-term follow-up are required to compare modern generation stent platforms focusing on different patient subgroups including small-vessel disease and acute coronary syndromes.
Acknowledgments
We acknowledge the support of Bets Conway and her team of research nurses at Gosford hospital. We pay credit to the researchers and patients involved in the trials incorporated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MRM contributed to study design, wrote the first draft and performed the statistical analysis. MRM, PB and CFS performed the systematic review. CFS and PB edited the manuscript. MRM and RS extracted the data for analysis. TF checked the data and provided consensus. CFS and MP performed the risk of bias analysis and TF provided consensus. TF devised the study, performed literature review, critically appraised and edited the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethics approval was not applicable for this secondary pooled analysis.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data is all available within this manuscript. Methods registered online with PROSPERO (CRD42019147136).