Article Text

Abstract
Objectives To enhance adherence to cardiac rehabilitation (CR), a patient education programme called ‘learning and coping’ (LC-programme) was implemented in three hospitals in Denmark. The aim of this study was to investigate the cost–utility of the LC-programme compared with the standard CR-programme.
Methods 825 patients with ischaemic heart disease or heart failure were randomised to the LC-programme or the standard CR-programme and were followed for 3 years.
A societal cost perspective was applied and quality-adjusted life years (QALY) were based on SF-6D measurements. Multiple imputation technique was used to handle missing data on the SF-6D. The statistical analyses were based on means and bootstrapped SEs. Regression framework was employed to estimate the net benefit and to illustrate cost-effectiveness acceptability curves.
Results No statistically significant differences were found between the two programmes in total societal costs (4353 Euros; 95% CI –3828 to 12 533) or in QALY (–0.006; 95% CI –0.053 to 0.042). At a threshold of 40 000 Euros, the LC-programme was found to be cost-effective at 15% probability; however, for patients with heart failure, due to increased cost savings, the probability of cost-effectiveness increased to 91%.
Conclusions While the LC-programme did not appear to be cost-effective in CR, important heterogeneity was noted for subgroups of patients. The LC-programme was demonstrated to increase adherence to the rehabilitation programme and to be cost-effective among patients with heart failure. However, further research is needed to study the dynamic value of heterogeneity due to the small sample size in this subgroup.
- cardiac rehabilitation
- education
- heart failure
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Many patients with ischaemic heart disease or heart failure do not succeed in sustaining lifestyle improvements, and only a fraction of the relevant patient group completes cardiac rehabilitation.
What does this study add?
To enhance adherence to cardiac rehabilitation, a patient education programme called ‘learning and coping’ was implemented in three hospitals in Denmark. Learning and coping programme increased adherence to cardiac rehabilitation; however, it did not appear to be cost-effective compared with standard cardiac rehabilitation.
How might this impact on clinical practice?
We observed substantial heterogeneity among subgroups of patients; the learning and coping programme was highly cost-effective among patients diagnosed with heart failure. However, due to small sample size of patients in this subgroup, investigation of dynamic value of heterogeneity is recommended for this subgroup.
Introduction
Exercise-based cardiac rehabilitation (CR) for patients with ischaemic heart disease (IHD) and heart failure (HF) has been investigated, and is considered cost-effective.1–3 However, many patients with IHD or HF do not succeed in sustaining lifestyle improvements, and only a fraction of the relevant patient group completes CR.4 5 In light of the beneficial effects of CR, it is important to develop patient education strategies which can help patients to improve adherence to CR and make lasting changes towards a healthier lifestyle.4 6 7
In Denmark, the standard CR-programme was an 8-week group programme which included physical training and patient education. To increase adherence to CR, improve health-related quality of life and reduce mortality and readmission, a patient education programme called ‘learning and coping’ (LC-programme) was added to the standard CR-programme and implemented within a randomised controlled trial (RCT) in three hospital units in Regional Hospital, West Jutland, Denmark4 (for programme details, see online supplementary table A1, appendix A). The LC-programme is a health pedagogical strategy that builds on situated and inductive teaching with high involvement from the participants and co-teaching with experienced patients.8 The main finding of the Danish LC-REHAB trial was that addition of the LC-programme to the standard CR-programme improved adherence to rehabilitation both in terms of exercise training and education. Patients with HF and low socioeconomic status appeared to benefit most from this intervention.9 However, no difference in return to work status was found 1 year after participation among a subsample of patients from both programmes.10
Supplemental material
Economic evaluations provide a useful comparative approach for considering costs and consequences on patient outcomes, and contribute to evidence-based policy and decision-making.11 Therefore, in addition to investigating the clinical effect of LC, we also conducted a cost–utility analysis for the present RCT after 5 months of follow-up, which demonstrated no statistically significant differences in costs or quality-adjusted life years (QALY) between the two programmes. However, a longer follow-up period seems to be essential in order to assess whether LC-programme yields higher utility or a decrease in long-term healthcare utilisation.12 The current study investigates the cost–utility of the LC-programme in CR compared with the standard CR-programme among patients with IHD and HF after 3 years of follow-up.
Methods
Target population
In total, 825 patients were included in the study between November 2010 and December 2012. Inclusion criteria were patients aged above 18 years referred to CR after hospitalisation with either IHD or HF. Included patients were randomly allocated to the intervention arm (LC-programme, n=413) or the control arm (standard CR-programme, n=412). The patients were allocated in a 1:1 ratio stratified for hospital unit, gender and diagnosis, in blocks of two to four, using a web-based system that was implemented independently of the research team.9
Intervention
The standard CR-programme was characterised by a structured deductive teaching style with use of identical pre-written slides in all hospital units. The LC-programme consisted of the standard CR-programme with addition of two individual clarifying interviews and co-teaching by experienced patients and health professionals with a theory-based, situated and inductive teaching approach4 8 (online supplementary table A1, appendix A). Detailed information on the trial and components of LC-programmes and standard CR-programmes has previously been published4 and is available in online supplementary appendix A.
Costing
The economic evaluation applied a societal perspective incorporating intervention cost, follow-up costs in the healthcare sector (primary and secondary care) and societal costs with regard to productivity loss due to sick leave.
Intervention costs
A micro-costing approach was used to calculate the cost of intervention for each programme, which is available in online supplementary appendix B (table A2). Briefly, this included the costs of both formal and informal time of the professionals and patients involved. Valuation of formal care was based on the average gross salary of nurses and physiotherapists involved in CR. The valuation of informal time (time spent by patients and experienced patients) was undertaken using the opportunity cost method, in which the value of a person’s time is reflected by his or her salary. National average gender-matched and age-matched salaries were used to value productive time (gross salary) and leisure time (net salary). These data were obtained from Statistics Denmark.13
To estimate transportation costs, we assumed that patients spent 20 min of time (10 km distance) to reach the hospitals. Time spent in transportation was valued by multiplying the assumed time by the patients’ net salary, and valuation of the cost of transport was performed by multiplying the assumed distance by the government tariff for transportation by private car for 2015. To value the transportation time of experienced patients, a journey of 20 min each way was again assumed and the same method of valuation was applied.
Primary healthcare costs
Data for resource use in primary healthcare were derived from the Danish National Health Service Register (number of primary care visits and related activity-based tariffs).14 The main categories of primary care included general practitioners, medical specialists, therapists (physiotherapists and chiropractors) and other services.
Secondary healthcare costs
Data for resource use of secondary healthcare were extracted from the Danish National Patient Registry15 and valued using tariffs of the diagnostic-related grouping for inpatient admissions and the Danish Ambulatory Grouping System for outpatient admissions.
Productivity loss costs
The National Labour Market Authority database (DREAM),16 containing information on all social benefits, was searched for data on weeks of sick leave taken. Productivity losses were calculated using weeks of inability to work for those who were part of the labour market at baseline, and valued using national age- and gender-matched gross salaries.
All cost estimates were adjusted for time preference and were inflated to 2015 Euro values using the common consumer price index, and a currency conversion rate of 1 Euro=7.45 DKK was applied.
Outcome parameter
In the trial, the SF-6D questionnaire, which is a generic health-state preference measure,17 was completed by patients. Data were collected at baseline, after intervention (2 months), 5 and 36 months. A regression-based analysis was applied in estimation of differences in QALY, as well as the prediction of adjusted QALY while controlling for baseline utility values.18
Handling of missing data
We observed missing data in the utility scores at baseline and all follow-up points (online supplementary table A3 in appendix C). The missing data did not follow a monotonic pattern; for example, there were some individuals with intermittent missing data at 5 months which returned to follow-up at 36 months.
Full QALY calculation was performed for a total of 367 participants (45%); of these, 355 participants had no missing data at any point and 12 participants died during the follow-up. Complete case analysis (CCA)—in which individuals with missing data are excluded—contravene the intention-to-treat principle by which all randomised patients should be included in analysis and, hence, lacks efficiency.19 Therefore, we used multiple imputation (MI) technique to include all patients in the analysis.20–22
We used logistic regression to explore the association between missing QALY on a selection of baseline variables (gender, age, body mass index, treatment allocation and SF-6D score at baseline) and observed outcome variables (resource use in primary and secondary sector and number of sick-week leaves). The baseline variables were not statistically significantly associated with participants having missing QALY. Age and gender were significant predictors of QALY. All outcome variables except for outpatient visits were associated with participants having missing QALY at the 5% significance level. The significant association indicates that missing at random (MAR) was a plausible assumption under which to conduct the analysis.
The base case analysis used chained equations (MI-MICE) under MAR.23 The MI model used age, gender and all outcome variables except for outpatient visits to impute missing utility scores. The imputation was conducted 40 times as there were up to 40% missing observations (online supplementary table A3 in appendix C). The utility scores were not normally distributed; therefore, predictive mean matching was used in imputation. To test the validity of the MI model, the distribution of imputed data were compared with observed data.
Cost–utility analysis
Resource use, costs and outcomes were tested for normality and distribution. Due to skewed data, comparative analyses were based on means with bootstrapping SE.24 We applied a non-parametric bootstrapping with 5000 replications.
We estimated the incremental monetary net benefit using a range of hypothetical threshold values for decision-makers’ willingness to pay for a QALY (from 0 to 100 000 Euros), and presented the incremental costs and incremental QALYs visually in a cost-effectiveness acceptability curve (CEAC) using the net benefit regression framework.25 CEAC was used to illustrate the probability of the intervention being cost-effective for a range of threshold values for willingness to pay for a QALY.25–27
To assess the robustness of the study, sensitivity analyses were conducted and the results were presented in the CEAC. The sensitivity analyses included CCA and intention-to-treat analysis of intervention cost. Furthermore, analyses of population heterogeneity were conducted by repeating the base case analysis for subgroups of patients with different diagnoses (IHD or HF). We used the net benefit regression to conduct the subgroup analyses by adding patient-specific baseline variables and a treatment–covariate interaction term to the regression model.
An annual discount rate of 0.03 was applied for both costs and QALY estimation due to the time horizon. All analyses were conducted in Stata V.15.
Results
No statistically significant difference was observed for baseline characteristics between the LC-programme and the standard CR-programme. However, patients were significantly different in adherence to the CR sessions.9 Patients in the LC-programme participated, on average, in 19.6 physical training sessions and in 6.4 education sessions. The numbers are 18.3 and 5.8, respectively, for the standard CR-programme.
Costs
Healthcare resource use in primary and secondary sectors, number of sick-leave weeks, and patient resource use are provided in table 1 and the relevant costs are presented in table 2. No statistically significant differences were observed between the two programmes for healthcare use in primary and secondary sectors, sick-leave weeks or associated costs. However, statistically significant differences were observed for patients’ resource use and the related patient-borne costs.
Resource use of LC-programme and standard CR-programme in cardiac rehabilitation
Mean costs of LC-programme and standard CR-programme in cardiac rehabilitation during 3 years of follow-up (Euros)
The per-protocol intervention cost was estimated to be 682 Euros for the LC-programme and 391 Euros for the standard CR-programme (online supplementary appendix B). The total societal costs per patient were estimated to be 48 365 Euros for the LC-programme and 44 012 Euros for patients in the standard CR-programme, which led to a non-significant difference of 4353 Euros (95% CI –3828 to 12 533) in favour of the standard CR-programme.
Outcome
Forty-five per cent of cases in the LC-programme, and 44% in the standard CR-programme, had complete responses for outcome parameters. No statistically significant differences in SF-6D scores or QALY were observed between the groups based on either complete cases or the imputed data (table 3).
Outcomes comparing LC-programme and standard CR-programme in cardiac rehabilitation
Cost–utility
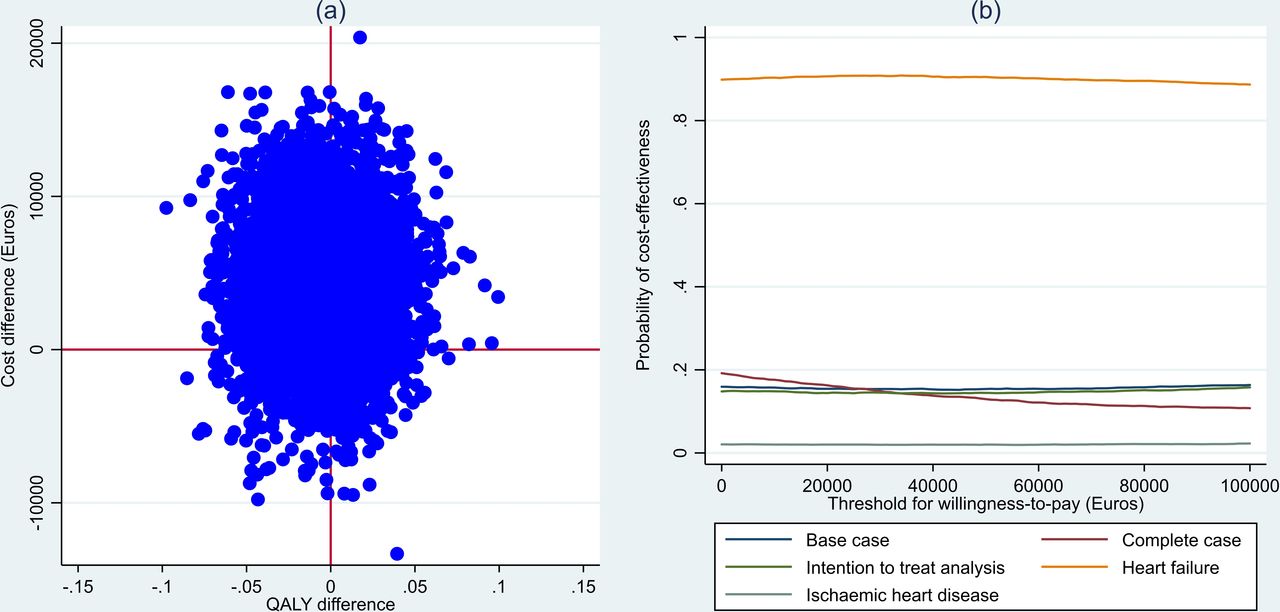
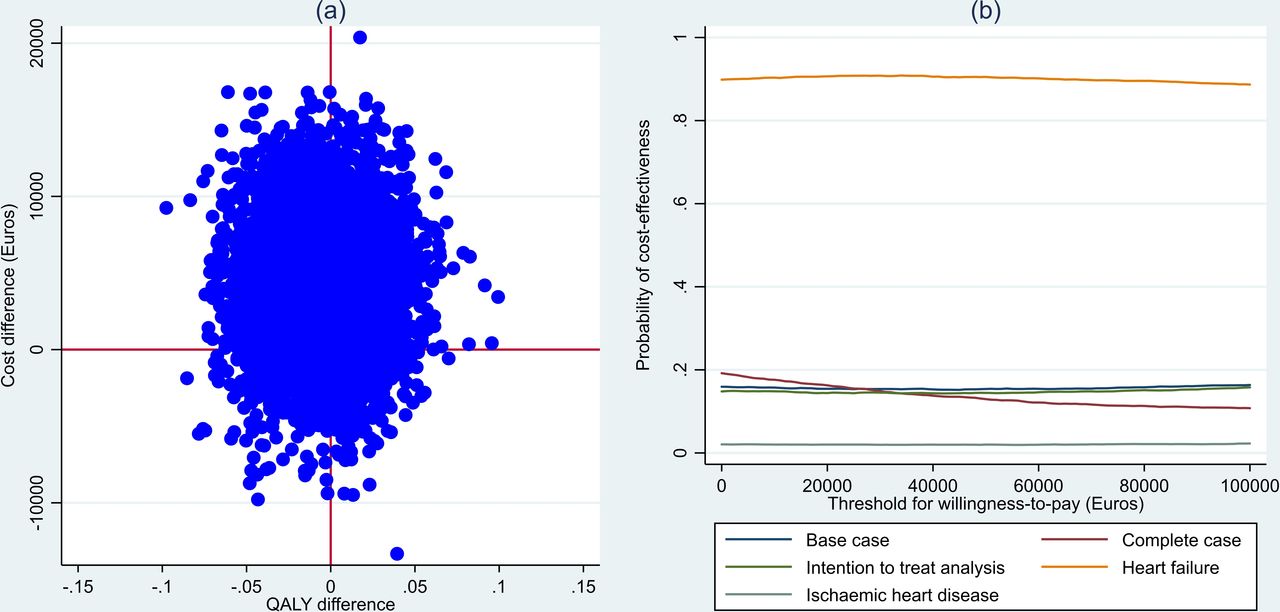
Results of bootstrapped replicates of differences in cost and QALY are located in all four quadrants of the scatter plot, which suggests uncertainty about the cost-effectiveness of the LC-programme (figure 1A). Therefore, CEAC was used as a method to illustrate this uncertainty for different willingness-to-pay threshold values for economic evaluation. The CEACs for the base case analyses demonstrated that the probability of the LC-programme being cost-effective did not exceed 16% for the defined threshold values for willingness to pay. Sensitivity analyses based on intention-to-treat analysis of intervention and the CCA followed a similar trend and confirmed the robustness of the results of the base case model (figure 1B).
{kind=link}
(A) Bootstrapped replicates of differences in costs and quality-adjusted life years (QALY) between LC-programme and standard CR-programme. (B) Cost-effectiveness acceptability curves for base case and alternative scenarios. CR, cardiac rehabilitation; LC, learning and coping.
The analyses of the subgroups for different diagnoses demonstrated that implementation of the LC-programme was cost-saving for patients with HF compared with the standard CR-programme (difference of –12 399 Euros (95% CI –30 016 to 5218), p=0.168), whereas use of the LC-programme was statistically significantly associated with higher costs for patients with IHD (difference of 8936 Euros (95% CI 51 to 17 822), p=0.049). The incremental QALY was 0.021 (95% CI –0.117 to 0.158, p=0.769) for patients with HF and –0.014 (95% CI –0.061 to 0.034, p=0.570) for patients diagnosed with IHD. This is illustrated by the cost-effectiveness acceptability curve and indicates that at a threshold of 40 000 Euros the LC-programme has a 91% probability of cost-effectiveness among patients with HF, whereas the curve for IHD did not exceed a 2% probability for the defined threshold values for willingness to pay (figure 1B). Conducting the subgroup analysis on complete cases supported the bidirectional conclusions with respect to the subgroups of patients with IHD and with HF.
Discussion
We investigated the cost–utility of the LC-programme in CR compared with the standard CR-programme among patients with IHD or HF, using data from a RCT. There were no statistically significant differences between the two programmes for costs or QALY. However, substantial heterogeneity was observed among subgroups of patients.
Available literature about economic evaluation of CR mainly focuses on comparing provision of CR versus no CR, comparing the location of service provision (hospital-based CR vs home-based CR) and, recently, comparing tele-health models of providing CR versus standard CR provision. CR is demonstrated to be cost-effective according to extant literature reviews28–30; however, one of the reviews suggested that further research is needed to determine the most cost-effective design of CR.28 In addition, it is recommended by the literature that healthcare professionals should be aware of patients’ reluctance to participate in CR programmes, and should adapt their messages and re-design CR programmes to promote participation and adherence.31 This study addresses this issue and contributes to provide information to decision-makers about using the LC-programme as a component of patient education in CR.
Decisions based on average measures of cost-effectiveness may lead to incorrect treatment recommendations for specific subgroups of patients because a treatment that is cost-effective for one group of patients may not be so for others.32 This RCT demonstrated some evidence of greater effect of the LC-programme on adherence among patients with HF than those with IHD, which provided the rationale for expecting a subgroup effect in economic evaluation. The LC-programme appeared likely to be cost-effective among patients with HF and unlikely to be so in patients with IHD. For patients with HF, the LC-programme was cost saving, and the probability of cost-effectiveness reached 91% at the threshold for willingness to pay of 40 000 Euros.
As a general principle, a subgroup should be large enough to ensure the reliability of inferences about the efficacy parameter, which is determined by power considerations.33 Thus, the small number of patients who were diagnosed with HF (n=176) introduces uncertainty into the parameter estimates. Further investigation of the dynamic value of heterogeneity (dynamic VoH) is therefore recommended. Dynamic VoH reflects the value derived from collecting new evidence to reduce the sampling uncertainty associated with subgroup-specific parameter estimates.32
We did not expect variability in cost-effectiveness between patients recruited in particular locations because all three hospital units involved in this study were following the same structure of CR provision and other relevant clinical guidelines. Due to ethical and equity considerations, we chose not to conduct subgroup analyses based on age or socioeconomic background as a source of heterogeneity.
Strengths and limitations
The main strengths of this study include the randomised design, which is considered to be of a relatively high standard due to the block randomisation, the stratified randomisation and the fact that the randomisation was implemented independently of the research team.34 In addition, the long follow-up period (3 years) is compatible with chronic conditions and enabled economic assessments of the long-term effects of the programmes.
Complete information on resource use and costs with no missing data, based on various national registries, added to the internal validity of the study. Missing outcome data were handled using multiple imputation technique and the robustness of the results was tested in alternative scenario models. Furthermore, the alternative scenarios of intention-to-treat analysis and CCA did not alter the overall findings.
Due to administrative issues, data on use of prescribed medication outside hospitals were not accessible. In addition, despite extensive Danish registries on primary and secondary sectors, data on social care provided by the municipalities were not available. However, use of other healthcare resources, for which data were available, was not statistically significantly different between the intervention and control arms, and therefore we do not expect that non-availability of medication data outside hospitals or other social care data would significantly impact the results.
Finally, the study was conducted in a Danish context with a specific CR structure, which limits generalisation of the results to other settings unless they share common characteristics.
Conclusion
This study demonstrated that there were no statistically significant differences in either costs or outcomes between the LC-programme and the standard CR-programme from a societal perspective after 3 years of follow-up.
Implementation of the LC-programme in a standard rehabilitation programme was demonstrated to increase adherence to CR. Furthermore, the LC-programme appeared to be a cost-effective strategy among patients diagnosed with HF. However, further research is needed to study the dynamic value of heterogeneity due to small sample size in this subgroup.
Acknowledgments
The authors would like to thank the nurses, physiotherapists and experienced patients, as well as the project co-ordinators, for their contributions to patient recruitment, intervention and data collection.
References
Footnotes
Correction notice This paper has been updated since first published to correct author name 'Bettina Wulff Risør'
Contributors All the authors contributed to conception or design of the study. VL participated in the design, planning and co-ordination of the LC-REHAB trial and provided details of the intervention and results of the programme adherence and other relevant information regarding the trial. NTD and BWR contributed to data analysis. NTD drafted the manuscript and all authors contributed to interpretation of the results, critically revised the manuscript and gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Funding This study was funded by TrygFonden (grant no. 125317); however, the LC-REHAB trial was funded by the Danish Ministry of Health, the Health Research Fund of Central Denmark Region and TrygFonden.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement No data are available. The data contain personal information and are not available.