Article Text

Abstract
Objective Heart failure (HF) impairs survival post coronary artery bypass grafting (CABG), but little is known about the postoperative quality of life (QoL) in patients with HF. We derived a patient-centred QoL surrogate and assessed the impact of different HF subtypes on this surrogate in the year post-CABG.
Methods We surveyed 3112 cardiovascular patients to derive a patient-centred disability outcome and studied this outcome in a population-based cohort. We defined preserved ejection fraction as ≥50% and reduced ejection fraction as <50%. The primary outcome was disability, defined according to compiled patient-derived values. The secondary outcomes consisted of each individual component of disability, and death. The incidence of disability was calculated using cumulative incidence functions, with death as a competing risk. We identified predictors of disability using cause-specific hazard models.
Results Patient-derived disability outcome consisted of stroke, nursing home admission and recurrent hospitalisations. When applied to 40 083 CABG patients (20.6% women), the incidence of disability was 5.4% while the incidence of death was 3.7% in the year post-CABG. Female sex was associated with an adjusted HR of 1.25 (95% CI 1.13 to 1.37) for disability. Women with HF with preserved ejection fraction had an adjusted HR of 1.73 (95% CI 1.52 to 1.98) for disability.
Conclusions Disability was a more frequent complication than death in the year post-CABG. Women experienced higher burden of disability than men, and female sex and the presence of HF were important disability risk factors. Efforts should be dedicated to disability risk prediction to enable patient-centred operative decision-making and to developing sex-specific treatment strategies to improve outcomes.
- coronary artery bypass grafting
- heart failure
- quality of life
- disability
- survival
- Patient-centered outcomes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- coronary artery bypass grafting
- heart failure
- quality of life
- disability
- survival
- Patient-centered outcomes
What is already known about this subject?
Current revascularisation trials are sometimes termed ‘tombstone trials’ as they focus on mortality instead of outcomes that may be more important from a patient’s perspective.
What does this study add?
We conducted a survey to derive a patient-centred disability outcome and assessed the impact of sex and heart failure on this outcome in the year post coronary artery bypass surgery.
We found that disability was a more frequent complication than death, and women experienced higher rates of disability than men.
How might this impact on clinical practice?
Our findings highlight the importance of sex-specific medical and surgical therapy to improve outcomes in patients with coronary artery disease.
Introduction
Heart failure (HF) is a sequela of severe coronary artery disease (CAD) and an important comorbidity in patients presenting for coronary artery bypass grafting (CABG). HF with reduced ejection fraction (HFrEF) is a widely regarded risk factor for morbidity and mortality following cardiac surgery,1–5 but HF with preserved ejection fraction (HFpEF) remains poorly characterised in the cardiac surgery literature. Furthermore, revascularisation trials have largely focused on mortality and major adverse cardiac events (MACE),6 and few surgical studies have been dedicated to patient-centred outcomes such as quality of life (QoL) or have used patient-derived QoL instruments. There is no universal agreement on the definition of disability as a surrogate of QoL in cardiovascular research.7 In a survey of patients with stroke, patients prioritised ‘home time’ (time spent alive, outside of hospital and free from recurrent stroke).8 9 Stroke is an important complication of CABG, the second most common reason for hospitalisation in older adults and the most common cause of long-term disability.10 11 Building on these previously identified elements, we surveyed a large group of cardiovascular patient alumni to explore the relative importance of longevity versus proposed disability-defining events such as stroke (due to its association with disability and loss of ‘home time’), recurrent non-elective hospitalisations (loss of ‘home time’) and nursing home admission (loss of independence of living). We then investigated the impact of HF on disability in women and men in the year following CABG in a population-based cohort.
Methods
Development of a relevant disability outcome
Following approval from the University of Ottawa Heart Institute (UOHI) Research Ethics Board, we partnered with the UOHI Patient Alumni Association to perform a survey of all current cardiovascular alumni members (N=3112). The UOHI Patient Alumni Association is a self-governing body that has been in place for over 40 years to provide support for patients and families living with cardiovascular diseases, as well as being a strategic partner with the UOHI in its delivery of patient-centred research and clinical care. The alumni communications officer first emailed the confidential survey link to all medical and surgical alumni members on 15 August 2017, followed by two reminders on 15 October 2017 and 1 January 2018. Survey results were collected anonymously using SurveyMonkey (San Mateo, California). The details of the survey are outlined in online supplementary appendix 1.
Supplemental material
Population-based cohort study
We conducted a population-based, retrospective cohort study in Ontario, Canada, between 1 October 2008 and 31 March 2015 to evaluate the impact of sex and HF on the patient-derived disability outcome. Included were adult patients ≥40 years of age who underwent primary isolated CABG. We excluded patients who were non-Ontario residents, who had previous cardiac surgery, or who had missing information on age, sex and EF (online supplementary figure S1).
Supplemental material
Data sources
We used the clinical registry data of CorHealth Ontario and population-level administrative healthcare databases with information on all Ontario residents available at the Institute for Clinical Evaluative Sciences. Individuals who underwent isolated CABG were identified from the CorHealth Ontario registry. CorHealth Ontario is a network of 20 hospitals that maintains a detailed prospective clinical registry of all patients who undergo invasive cardiac procedures in Ontario. It captures demographic, comorbidity and procedural-related information and has been validated through selected chart audits. In addition, CorHealth Ontario EF and angiographic data undergo core laboratory validation.12
Administrative databases were linked deterministically by using encrypted codes that preserved patient confidentiality. We first linked the CorHealth Ontario registry (date and type of cardiac procedures, left ventricular (LV) function data) with the Ontario Congestive Heart Failure (CHF) database to classify CABG patients by baseline EF and HF status. The CHF database was derived from physician billings based on either one documented HF admission or two outpatient claims for HF within 1 year. This algorithm has been previously validated and shown to have 85% sensitivity and 97% specificity in identifying HF events.13 These data were then linked to the Canadian Institute for Health Information’s Discharge Abstract Database (DAD; comorbidities and hospital admissions) and Same Day Surgery (SDS) database (comorbidities), Ontario Health Insurance Plan (OHIP) database (physician service claims), Registered Persons Database (RPDB; ascertainment of vital statistics), the Continuing Care Reporting System (CCRS; admissions to long-term care facilities) and Canadian census. These administrative databases have been validated for many outcomes, exposures and comorbidities.14–17
Classification of HF by LV function
Diagnosis of HFpEF is based on the presence of HF and LV ejection fraction (LVEF) of ≥50%.18 Preoperative EF was obtained from the CorHealth Ontario registry and classified as preserved (pEF) if ≥50% and reduced (rEF) if EF was <50%.3 18 The authors then categorised the patients into HFpEF, HFrEF, pEF without HF and rEF without HF using previously described methods.3 19
Comorbidities
Comorbidities were identified from the CorHealth Ontario clinical registry and supplemented with data from DAD, SDS and OHIP using the International Classification of Diseases 10th Revision CA codes20 within 5 years prior to CABG and using validated algorithms.14 16 21 22 We estimated the socioeconomic status based on patients’ neighbourhood median income in the Canadian census and determined their residence (rural vs urban) using Statistics Canada definitions.23 Emergent procedural status was ascertained from the CorHealth Ontario registry and supplemented with OHIP claims data, where the anaesthesia provider identified the surgery as emergent under the American Society of Anesthesiologists physical status classification. Height, weight and body mass index (BMI) identified from the CorHealth Ontario registry were used to define morbid obesity (weight >159 kg or BMI ≥40 kg/m2). Frailty status was identified using the Johns Hopkins Adjusted Clinical Groups frailty-defining diagnoses indicator, which is an instrument designed and validated for research of frailty-related outcomes and resource utilisation using administrative data.24–28
Outcomes
The primary outcome was disability, defined as patient-derived composite of stroke, nursing home admission and recurrent non-elective hospital admissions of ≥3 episodes occurring within 1 year of surgery. The secondary outcomes consisted of each individual component of the disability outcome, and death. Mortality was ascertained using the RPDB. Stroke was identified using a validated algorithm with 70% sensitivity and 99% specificity, based on either one stroke hospitalisation or two physician billings.29 Non-elective hospital admissions were ascertained using the DAD, and long-term care admissions were ascertained using the CCRS.
Statistical analysis
All analyses were performed in the overall cohort and then stratified by sex. Continuous variables were expressed as mean (SD) and categorical variables as number (proportions). Disability-free survival was defined as survival time from the date of index surgery until the date of a disability-defining event, death or last follow-up. For patients experiencing recurrent non-elective hospitalisations, disability was considered to occur on the date of the third admission. Patients were censored if they were ineligible for OHIP for >2 consecutive quarters (ie, have left Ontario).
We estimated the cumulative incidence of post-CABG disability over time using the cumulative incidence functions (CIFs) to account for death as a competing event. We plotted direct adjusted CIF curves for disability and each of its individual endpoints, stratified by sex and HF status. Direct adjustment was made for each of the covariates listed in table 1, by adopting the Fine-Gray model as the underlying regression model to compute the adjusted CIFs.30 We identified predictors of disability using multivariable cause-specific hazard models, with death as a competing risk. We then explored the modifying effect of sex using multiplicative interaction terms of sex with each of the covariates from the multivariable model, and identified sex-specific disability risk factors by stratifying the main regression analysis by sex.
Multivariable predictors of disability at 1 year post-CABG in the pooled analysis
We performed two sensitivity analyses. First, we used generalised estimating equations (GEE) to determine the adjusted association of patient-level characteristics with disability while accounting for clustering of patients within hospitals. Next, we added the completeness of revascularisation to this GEE model to evaluate the impact of incomplete revascularisation on disability. Incomplete revascularisation was defined as the presence of ≥1 ungrafted vessels with ≥70% stenosis in the left anterior descending, circumflex or right coronary artery territories.
The measure of association was HR with 95% CI. Analyses were performed using SAS V.9.3, with statistical significance defined by a two-sided p value of <0.05.
Results
Survey of patient-centred disability outcomes
A total of 1015 (32.6%) cardiovascular alumni responded to the survey (27.6% women, 68.5% over the age of 65). Of those who responded, 87.4% had a previous hospitalisation (33.0% for HF and 42.6% for myocardial infarction (MI)), 8.5% had stroke and 0.8% were nursing home residents. Due to the anonymous nature of the survey, demographic information was not available for the non-respondents. The majority of respondents (82.1%) indicated they would sacrifice longevity for treatments that would likely lead to improved QoL. Their specific preferences were to be free from stroke (81.0%); hospital admissions, including those for HF (77.7%) and MI (78.8%); and nursing home admission (67.6%). Although many (55.5%) would be tolerant of a single hospital admission, 21.9% would be intolerant of 2, while the majority (60.7%) would be intolerant of ≥3 non-elective admissions per year. When asked to prioritise these outcomes, patients ranked freedom from stroke as most important, followed by staying alive for as long as possible, freedom from hospitalisation and nursing homes (online supplementary figure S2). We therefore defined disability as the composite of stroke, nursing home admission and recurrent non-elective hospital admissions of ≥3 episodes per year.
Prevalence and patient characteristics by HF subtype
A total of 40 083 CABG patients were included in the study (20.6% women). Overall, 22 231 (55.5%) had pEF without HF, 10 284 (25.7%) had rEF without HF, 2752 (6.9%) had HFpEF and 4816 (12.0%) had HFrEF. Table 2 summarises the demographics and comorbidities of these patients by HF status.
Baseline characteristics by HF status
Table 3 summarises the baseline and operative characteristics of patients with HF, stratified by EF and sex. Of the patients with HFpEF, 873 (31.7%) were women. Women with HFpEF were more likely than men to be older, of lower socioeconomic status, to have emergent surgery, recent MI, hypertension, chronic lung disease, diabetes, hypothyroidism and anaemia, but less likely to have previous percutaneous coronary interventions, remote MI, atrial fibrillation, morbid obesity, chronic renal disease and dialysis. Of the patients with HFrEF, 1090 (22.6%) were women. Women with HFrEF were more likely than men to be older, to be of slightly lower income status, to have emergent surgery, recent MI, hypertension, chronic lung disease, diabetes, hypothyroidism and anaemia, but less likely to have remote MI, atrial fibrillation and morbid obesity.
Baseline characteristics of men and women with HFpEF and HFrEF
Disability and HF status
Table 4 summarises the rates of disability and individual disability-defining events by HF status. One year post-CABG, 2152 (5.4%) developed disability and 1466 (3.7%) died. In addition, 1215 (3.0%) developed stroke, 865 (2.2%) had recurrent non-elective hospitalisations and 254 (0.6%) were admitted to long-term care facilities.
Event rates within 1 year following coronary artery bypass grafting, by heart failure status
Cumulative incidence of disability was higher in patients with HF compared with those without HF (Gray’s test, p<0.001). At 1 year, disability occurred in 11.4% of patients with HFpEF, 10.7% of HFrEF, 4.7% of rEF without HF and 3.8% of pEF without HF. The rates of individual disability-defining events were also higher in patients with HFpEF. One-year mortality rates were highest in the HFrEF group (11.1%), followed by HFpEF (8.3%), rEF without HF (2.9%) and pEF without HF (1.8%). Overall, patients with HFpEF experienced higher rates of disability, while patients with HFrEF experienced higher rates of death. After multivariable adjustment of all risk factors listed in table 1, the cause-specific HRs for disability were 1.11 (95% CI 0.99 to 1.25) for rEF without HF, 1.81 (95% CI 1.61 to 2.04) for HFpEF, and 1.68 (95% CI 1.46 to 1.93) for HFrEF.
Sex differences in disability
Female sex was associated with an increased risk of disability (adjusted HR 1.25 (95% CI 1.13 to 1.37)), and this association remained robust in sensitivity analyses that accounted for clustering of patients within hospitals and completeness of revascularisation (table 1).
The sex-specific rates of disability and disability-defining events are summarised in table 5 and figure 1. Women had higher rates of disability than men across most HF categories except HFrEF, and women with HFpEF constituted a high disability risk group. Sex modified the association between disability and HF, age, MI, cerebrovascular disease and chronic renal disease (table 6). Specifically, rEF and HFrEF were associated with disability in women but not men, and HFpEF posed a greater risk of disability in women. Additionally, in patients aged 65–74 years, male sex alone was associated with an increased risk of disability, while in the ≥85 age group women had a higher risk of disability than men. Cerebrovascular and chronic renal diseases were also associated with higher disability risks in women.
Event rates within 1 year following coronary artery bypass grafting, stratified by sex
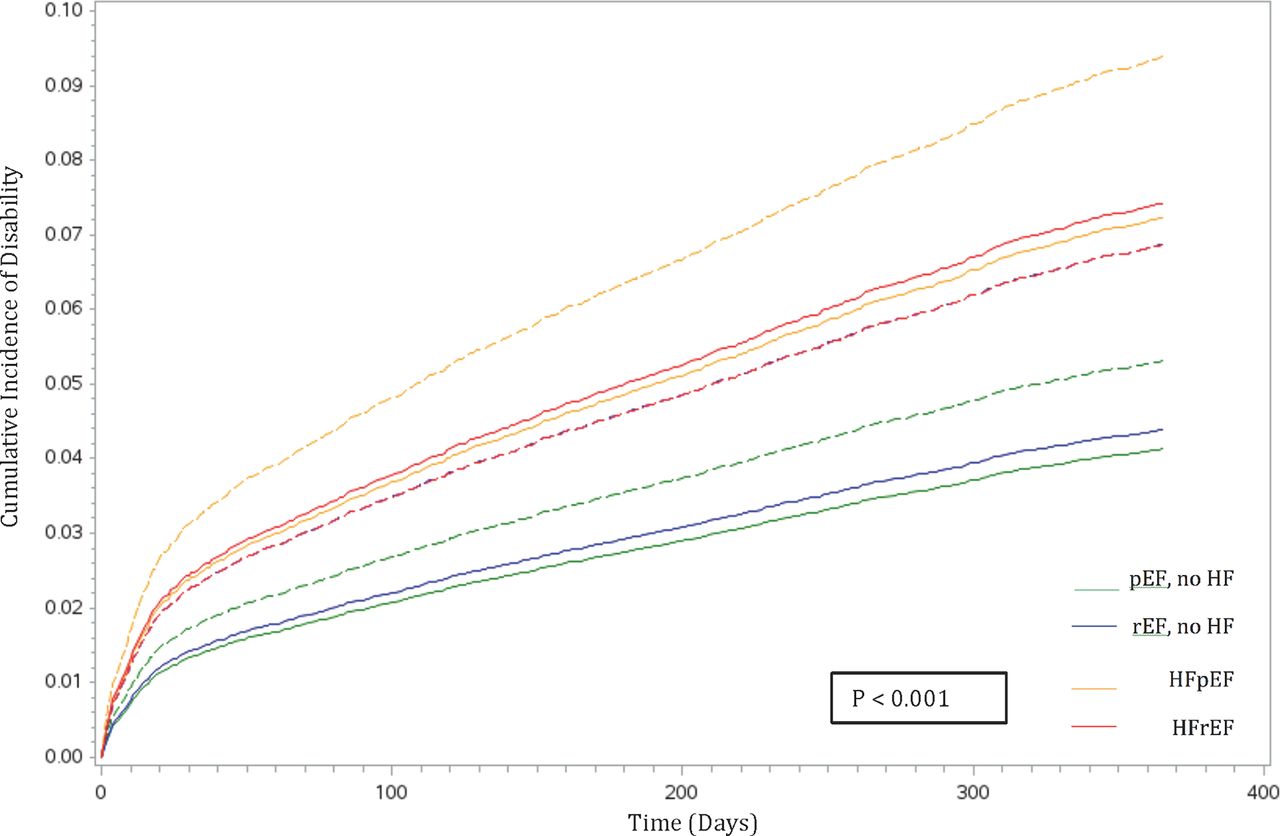
Adjusted cumulative disability incidence by sex and heart failure status. The solid lines represent adjusted cumulative incidence in men. The dotted lines represent adjusted cumulative incidence in women. HF, heart failure; HFpEF, HF with preserved ejection fraction; HFrEF, HF with reduced ejection fraction; pEF, preserved ejection fraction; rEF, reduced ejection fraction.
Sex-specific disability risk factors post coronary artery bypass grafting
The direct adjusted CIFs of stroke, recurrent non-elective hospitalisations and long-term care admissions were higher in women than men across most HF categories (figure 2). Women with HFpEF were at higher risk of stroke and recurrent hospitalisations, while women with HFrEF were at higher risk of entering long-term care.

{kind=link}
{kind=link}
Adjusted cumulative incidence of stroke, by sex and heart failure status. The solid lines represent cumulative incidence in men. The dotted lines represent cumulative incidence in women. HF, heart failure; HFpEF, HF with preserved ejection fraction; HFrEF, HF with reduced ejection fraction; pEF, preserved ejection fraction; rEF, reduced ejection fraction.
Discussion
We derived a patient-centred disability outcome as a meaningful surrogate for postoperative QoL and demonstrated the feasibility of applying it in population-based data. We found that sex and HF were important risk factors for disability in the year following CABG. Specifically, disability was a more frequent complication than death. HFpEF was associated with higher rates of disability, while HFrEF was associated with higher rates of death. In addition, disability rates were higher in women, especially women with HF. Our findings highlight the need for personalised disability risk prediction tools to empower shared surgical decision-making, and for future clinical trials to develop sex-specific medical and surgical strategies.
Need for patient-centred outcomes in cardiovascular research
Clinicians sometimes make decisions that are misaligned with patient preferences and values.31 The lack of patient-oriented data from existing revascularisation trials, sometimes termed ‘tombstone trials’,32 plays a role. These trials focus primarily on mortality and MACE33 as these endpoints are easier to measure and are perceived to be more objective than QoL.7 33–35 CABG is an advancing field where operative mortality has steadily declined over the years.36 As CABG candidates (online supplementary appendix 1) advance in age and medical complexity, their expectations often shift towards how treatments would affect their personal freedom and mobility, rather than longevity alone.6 31–33 37
The advent of population-based administrative databases and clinical registries offers efficient means for identifying disparities in healthcare systems. Long-term QoL outcomes are difficult to study prospectively and have so far been infeasible using administrative data due to lack of validated QoL elements in these repositories. We derived a working definition of ‘disability-free survival’ based on input of a large mixed cardiac medical and surgical cohort. This measure could be further developed through cardiovascular studies using administrative data.
Sex differences in post-CABG disability
Health-related QoL at 1 year post-CABG has been reported using the short form 36 (SF-36) in several smaller observational studies. In a single-centre study assessing the QoL of 112 patients from 2005 to 2008, patients reported higher than normative scores in the subscales of social functioning, role physical and role emotional, and lower scores in physical function, bodily pain, general health, vitality social function and mental health. Additionally, men reported higher postoperative physical function and role emotional scores compared with women.38 In a study of 186 patients from 1995 to 1996, poor QoL at 1 year post-CABG was associated with poor preoperative health status, while high levels of social support were associated with improved postoperative QoL.39 Using a patient-derived QoL surrogate, we were able to examine post-CABG outcomes at the population level. Our findings highlight the compounding risk of female sex, older age (≥85 years), cerebrovascular and chronic renal disease on disability and point to the importance of these factors in the perioperative risk stratification process.
Rates of short-term (30-day) readmissions have been reported in various population-based cohorts and range from 0% to 27% following CABG.40–42 Long-term post-CABG readmissions have mostly been reported as part of composite outcomes such as in the case of the Surgical Treatment for Ischemic Heart Failure (STICH) trial.1 43 In STICH, 65% of patients were dead or hospitalised at 5 years of follow-up,43 89% at 10 years.1 In a historical cohort of 8910 patients who underwent primary isolated CABG between 1980 and 1993, 1-year survival without cardiac readmissions occurred in 93%.44 Although lacking in detailed sex-specific analyses, these authors reported a higher rate of cardiac readmissions in women.44 Our study reports on modern 1-year hospital readmission rates and adds to the literature that female sex and HF (especially HFpEF) are important risk factors for recurrent non-elective hospitalisations. Our findings suggest that extended postoperative follow-up should be tailored to women with signs and symptoms with HF and not based on EF alone.3
Our reported rates of stroke are consistent with the literature.45–47 In addition, our finding of higher rates of stroke in women and those with HFpEF expanded our knowledge of this complication. Consistent with previous reports,19 48 49 we found a higher prevalence of HFpEF in women presenting for CABG surgery. This is likely due to HFpEF being a disease of older women and those with chronic arterial hypertension, whose rightward cerebral autoregulation shift predisposes them to cerebral ischaemia when exposed to even mild degrees of intraoperative hypotension.50 Women and those with HFpEF may therefore benefit from individualised perioperative haemodynamic management to mitigate the risk of perioperative stroke.50
In summary, our findings highlight an important care gap in that current delivery of medical and surgical therapies for CAD are insufficiently specific to women. Women are under-represented in clinical trials, and much of the practice guidelines are based on extrapolated trial data from male patients. Future trials could focus on evaluating the specific effect of pharmacological and surgical techniques (such as multiple arterial grafting and off-pump CABG) in women as well as in men. Furthermore, our findings point to women with HF as a specific group that is likely to benefit from targeted medical and social interventions.
Limitations and strengths
This study has several limitations. First, our disability measure needs to be prospectively validated against established QoL instruments. However, our study is a first step towards describing the burden of disability post-CABG at the population level. Second, data pertaining to stroke severity are unavailable in the databases used. As some patients with stroke experience full functional recovery, our findings may have overestimated the burden of stroke-related disability. Third, the lack of natriuretic peptides measurements precluded the use of this biomarker as a third diagnostic criterion for HFpEF.18 However, brain natriuretic peptide (BNP) measurements are not a routine practice in Ontario, and whether BNP would further improve risk stratification in patients with HF, above and beyond physician-diagnosed HF, remains to be determined. Finally, cohort studies are by nature subjected to residual confounding.
Conclusions
We used a patient-derived disability measure to identify gaps in health outcomes in a large cohort of patients who underwent isolated CABG. We found disability to be a more frequent complication than death in the year postsurgery, and in addition we identified female sex and the presence of HF as important disability risk factors. Future research should be dedicated to personalised disability risk prediction to guide patient-centred operative decision-making, and to sex-specific medical and surgical strategies to improve outcomes in patients with CAD.
Acknowledgments
This study was supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The authors acknowledge that the clinical registry data used in this analysis are from participating hospitals through CorHealth Ontario, which serves as an advisory body to the MOHLTC, is funded by the MOHLTC, and is dedicated to improving the quality, efficiency, access and equity in the delivery of the continuum of adult cardiac, vascular and stroke services in Ontario, Canada. The authors also acknowledge the usage of data compiled and provided by the Canadian Institute for Health Information. These data sets were linked using unique encoded identifiers and analysed at the ICES.
References
Footnotes
Contributors LYS contributed to the conception and design of the work, and obtained funding for the study. All authors contributed to the design of the work. LYS and ABE contributed to the acquisition and analysis of data. All of the authors contributed to the interpretation of data. LYS contributed to drafting of the manuscript, which all of the authors revised. All of the authors agree to be accountable for all aspects of the work, including the accuracy and integrity of the data presented.
Funding We acknowledge support from an operating grant from the University of Ottawa Department of Anesthesiology and Pain Medicine (Grant #4566). JVT was supported by a Canada Research Chair in Health Services Research and a Career Investigator Award from the Heart and Stroke Foundation of Ontario. DSL is supported by a mid-career investigator award from the Heart and Stroke Foundation and is the Ted Rogers Chair in Heart Function Outcomes. PCA is supported by a Career Investigator Award from the Heart and Stroke Foundation. The funders do not have a role in the design and conduct of the study, in the collection, analysis and interpretation of the data, nor in the preparation, review or approval of the manuscript.
Competing interests None declared.
Patient consent Not required.
Ethics approval The University of Ottawa Heart Institute Research Ethics Board approved the survey study. The Research Ethics Board of Sunnybrook Health Sciences Centre, Toronto, Canada, approved the population-based study and waived the need for informed consent.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement The data and study materials will not be made available to other researchers for purposes of reproducing the results or replicating the procedure.