Article Text

Abstract
Objectives To describe the dynamics of N-terminal pro-B-type natriuretic peptide (NT-proBNP) from preoperative evaluation to 6-month follow-up in patients undergoing aortic valve intervention, and to evaluate NT-proBNP with regard to 1-year mortality.
Methods At preoperative evaluation, we prospectively included 462 patients accepted for aortic valve intervention. The median time to surgical aortic valve replacement (SAVR; n=336) or transcatheter aortic valve implantation (TAVI; n=126) was 4 months. NT-proBNP was measured at enrolment for preoperative evaluation, on the day of surgery, postoperatively on day 1, day 3 and at the 6-month follow-up. Subgroups of patients undergoing SAVR with aortic regurgitation and aortic stenosis with and without coronary artery bypass were also analysed.
Results NT-proBNP remained stable in all subgroups during the preoperative waiting period, but displayed a substantial transient early postoperative increase with a peak on day 3 except in the TAVI group, which peaked on day 1. At the 6-month follow-up, NT-proBNP had decreased to or below the preoperative level in all groups. In the SAVR group, NT-proBNP preoperatively and on postoperative days 1 and 3 revealed significant discriminatory power with regard to 1-year mortality (area under the curve (AUC)=0.79, P=0.0001; AUC=0.71, P=0.03; and AUC=0.79, P=0.002, respectively). This was not found in the TAVI group, which had higher levels of NT-proBNP both preoperatively and at the 6-month follow-up compared with the SAVR group.
Conclusions The dynamic profile of NT-proBNP differed between patients undergoing TAVI and SAVR. NT-proBNP in the perioperative course was associated with increased risk of 1-year mortality in SAVR but not in TAVI.
- heart failure
- surgery-valve
- aortic valve disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
N-terminal pro-B-type natriuretic peptide (NT-proBNP) is a well-established biomarker for heart failure, and it is also a relevant marker for the outcome in cardiac surgery. The predictive value of preprocedural and postprocedural NT-proBNP levels for mortality in selected groups of patients undergoing cardiac intervention has been presented in previous publications.
What does this study add?
To our knowledge, this is the first paper describing the NT-proBNP levels from the preoperative evaluation to the 6-month follow-up in an unselected cohort of patients with aortic valve disease. The inclusion of patients undergoing surgical aortic valve replacement and transcatheter aortic valve intervention enables a comparison of the two different procedures.
How might this impact on clinical practice?
Our results may aid the decision on the timing of intervention for aortic valve disease. They also provide the postoperative levels and dynamics for NT-proBNP in the different subgroups of patients undergoing intervention for aortic valve disease as well as for patients with aortic stenosis undergoing surgical aortic valve replacement and transcatheter aortic valve intervention, which may serve as reference when in clinical practice.
Introduction
Aortic valve intervention has evolved to be one of the most common cardiac procedures in the Western world today.1 Prior to the transcatheter aortic valve intervention (TAVI) era, patients found unfit for open heart surgery were predestined for an early death due to aortic stenosis.2 The results in aortic valve surgery are excellent. However, severe morbidity and mortality postoperatively, both in the short and long term, are still hazards that need to be taken into account.3 In patients undergoing TAVI, being older and with more comorbidity, the periprocedural morbidity and mortality are even higher.4
N-terminal pro-B-type natriuretic peptide (NT-proBNP) has attracted growing interest as a marker for postoperative outcome, not just in cardiac surgery.5 It is a well-established diagnostic and prognostic biomarker for heart failure and acute coronary syndromes.6 Most studies reporting on natriuretic peptides in cardiac surgery are small and relate to short-term outcome.7 The dynamics of NT-proBNP over time from preoperative evaluation to postoperative follow-up remain to be delineated. Also, only addressing the association of preoperative levels of biomarkers such as NT-proBNP to outcome fails to take into account any periprocedural event that might affect outcome. Studies reporting on NT-proBNP and outcomes after both cardiac and non-cardiac surgery show a substantial variety in preoperative NT-proBNP cut-off levels with regard to best predictive value.8 The underlying pathophysiology and the type of intervention probably influence the NT-proBNP levels associated with adverse outcome.9
Thus, our aims were to describe the levels of NT-proBNP, from enrolment at preoperative evaluation to the 6-month follow-up in patients undergoing aortic valve intervention, to compare the levels between patients with aortic regurgitation, aortic stenosis, and with the combination of aortic stenosis and coronary artery disease, to compare the NT-proBNP dynamics in patients with aortic stenosis undergoing surgical and transcatheter intervention (SAVR), to relate the preprocedural and postprocedural levels of NT-proBNP to 1-year mortality, and to find factors related to the early postprocedural NT-proBNP elevation.
Methods
Protocol
This prospective, longitudinal, observational study was conducted between June 2008 and January 2013 at the University Hospital in Linköping, which serves a population of over 1 million in the southeast region of Sweden. All patients in the region undergoing preoperative evaluation for aortic valve surgery were screened for the study. Exclusion criteria were: informed written consent not possible, conditions requiring emergency procedure and active endocarditis.
Blood samples of plasma NT-proBNP were collected at preoperative evaluation, preoperatively <24 hours before index procedure, on postoperative day 1, postoperative day 3 and at the 6-month follow-up. Plasma levels of NT-proBNP were analysed using an electrochemoluminescence immunoassay on a Roche Elecsys 2010 automated device (Roche Diagnostics, Basel, Switzerland), and the results were blinded prior to data analyses. One core laboratory was used and the following upper reference limits (URLs) were applied: 450 ng/L for <50 years, 900 ng/L for 50–75 years and 1800 ng/L for >75 years.10 11 Clinical data were prospectively registered in and obtained from our database, Carath (Fujitsu, Tokyo, Japan). Mortality data were collected from the Swedish Civil Registry.
Postoperative heart failure was defined as a haemodynamic state when the cardiac output does not meet the systemic demand without supportive measures other than correction of volume or vascular resistance. Previously reported mixed venous oxygen criteria were used to define the haemodynamic state.12 Supportive measures or treatment consisted of an intra-aortic balloon pump or ventricular assist device, or infusion of one or more inotropes for more than 30 min in dosages as listed below: epinephrine ≥0.033 μg/kg of body weight per minute, milrinone ≥0.375 μg/kg of body weight per minute, dopamine ≥4 μg/kg of body weight per minute, levosimendan regardless of dose or need for two inotropes at any dosage.
Ethics
The study was approved by The Regional Ethical Review Board (M 198-07, T 126-08, 2012/422-32) and patients were recruited after providing written, informed consent in accordance with the World Medical Association’s Helsinki declaration on ethical principles for medical research involving human subjects.
Patients
A total of 548 patients with aortic valve disease eligible for aortic valve intervention were screened and 462 patients were included in the study at the preoperative evaluation. One hundred and 26 patients underwent TAVI for aortic stenosis (AS) and 336 patients had SAVR (All-SAVR). In the All-SAVR group, the indication for surgery was AS (AS SAVR) in 199 patients, AS and coronary artery disease (AS+CABG SAVR) in 75 patients and aortic regurgitation (AR SAVR) in 42 patients. The All-SAVR group also included 20 patients not analysed in separate groups; 5 patients with concomitant mitral valve surgery, 10 patients with other major concomitant procedures, and 5 patients with equal significance of their AS and AR.
Statistics
Continuous variables are presented as median (25th to 75th percentiles) and categorical variables as numbers (%). Fisher’s exact test and χ2 test were used accordingly for dichotomous data and a Mann-Whitney U test for comparisons between two groups. For comparisons for more than two groups, a Kruskal-Wallis test was used for continuous data, taking into account multiple comparisons of mean ranks for all groups P value (two tailed) and post hoc comparisons of mean ranks of all pairs of groups.13 For dichotomous data and multiple group comparison, χ2 test in large contingency table and post hoc χ2 2×2 with Bonferroni correction were applied. A Wilcoxon signed-rank test with Bonferroni correction was used for repeated measurements within groups. Pearson correlation was used when appropriate. Receiver operating characteristic (ROC) analysis was carried out to calculate the area under the curve and to evaluate the prognostic performance of NT-proBNP with regard to 1-year mortality. Equal weight to specificity and sensitivity was given for calculation of best cut-off point by choosing the point on the ROC curve closest to 100% sensitivity and 100% specificity. Linear regression models were used to analyse the influence of age, gender, renal function, New York Heart Association class, congestive heart failure, creatine kinase MB (CK-MB), ventricular function, cross clamp time (CCT), extracorporeal circulation time (ECCT), periprocedural volume load and postoperative heart failure on the rise of NT-proBNP. The rise of NT-proBNP was calculated from preoperatively to the individual postprocedural peak level chosen from the first and the third postoperative day measurements. The independent variables were selected a priori based on clinical relevance. In the collinearity diagnostics with the variance inflation factor, no collinearity was found between the selected variables. Statistical analyses were performed with computerised statistical packages (Statistica V.10.0; StatSoft, Tulsa, Oklahoma, USA) and IBM SPSS Statistics V.22.0 (IBM, Armonk, New York, USA). All tests were performed two sided and P <0.05 was considered to indicate significance.
Results
Patients
The patient’s characteristics are presented in table 1. The EuroSCORE II was found to be higher in both the TAVI group and in the AS+CABG group compared with the AS (SAVR) group and the AR (SAVR) group. The patients with AR were younger and a higher proportion were men compared with the other groups. The median time from inclusion to intervention was 126 (81–179) days for the cohort as a whole. No patient died during the waiting time.
Patient preoperative and postoperative characteristics
NT-proBNP levels and dynamics
The dynamic response of NT-proBNP to intervention was different between groups (figure 1A–E). All groups showed a significant increase of NT-proBNP from the preintervention levels to the first postprocedural day with a further increase to day 3, except for the TAVI group who peaked at postprocedural day 1. The dynamic response of NT-proBNP to surgery, ΔNT-proBNP from preoperatively to the third postoperative day was lower in the AR (SAVR) group compared with the AS (SAVR) and AS+CABG (SAVR) groups; ΔNT-proBNP 2055 (1136–3080) ng/L versus 3020 (1881–4700) ng/L and 3524 (2250–5810) ng/L; P<0.01 and P<0.001. Patients undergoing isolated procedure for AS had lower NT-proBNP at the 6-month follow-up compared with the preoperative levels, regardless of the type of procedure (TAVI or SAVR) (figure 1B,C). The AS+CABG (SAVR) and AR (SAVR) groups showed no significant decrease in NT-proBNP from preoperative measurement to the 6-month follow-up. However, patients with NT-proBNP concentrations above the URL at preoperative evaluation decreased from 2380 (1810–3920) ng/L to 1205 (320–3860) ng/L, P=0.01 in the AS+CABG (SAVR) group and from 1370 (920–5060) ng/L to 850 (310–1160) ng/L, P=0.02 in the AR (SAVR) group.

N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels for patients undergoing surgical aortic valve replacement (SAVR) (A), patients undergoing transcatheter aortic valve replacement (TAVI) (C) and for the three large subgroups of patients undergoing SAVR based on cardiac pathology (B, D and E). Data are shown as median and 25th to 75th percentile. Wilcoxon signed-rank test with Bonferroni correction was used for repeated comparisons within groups.
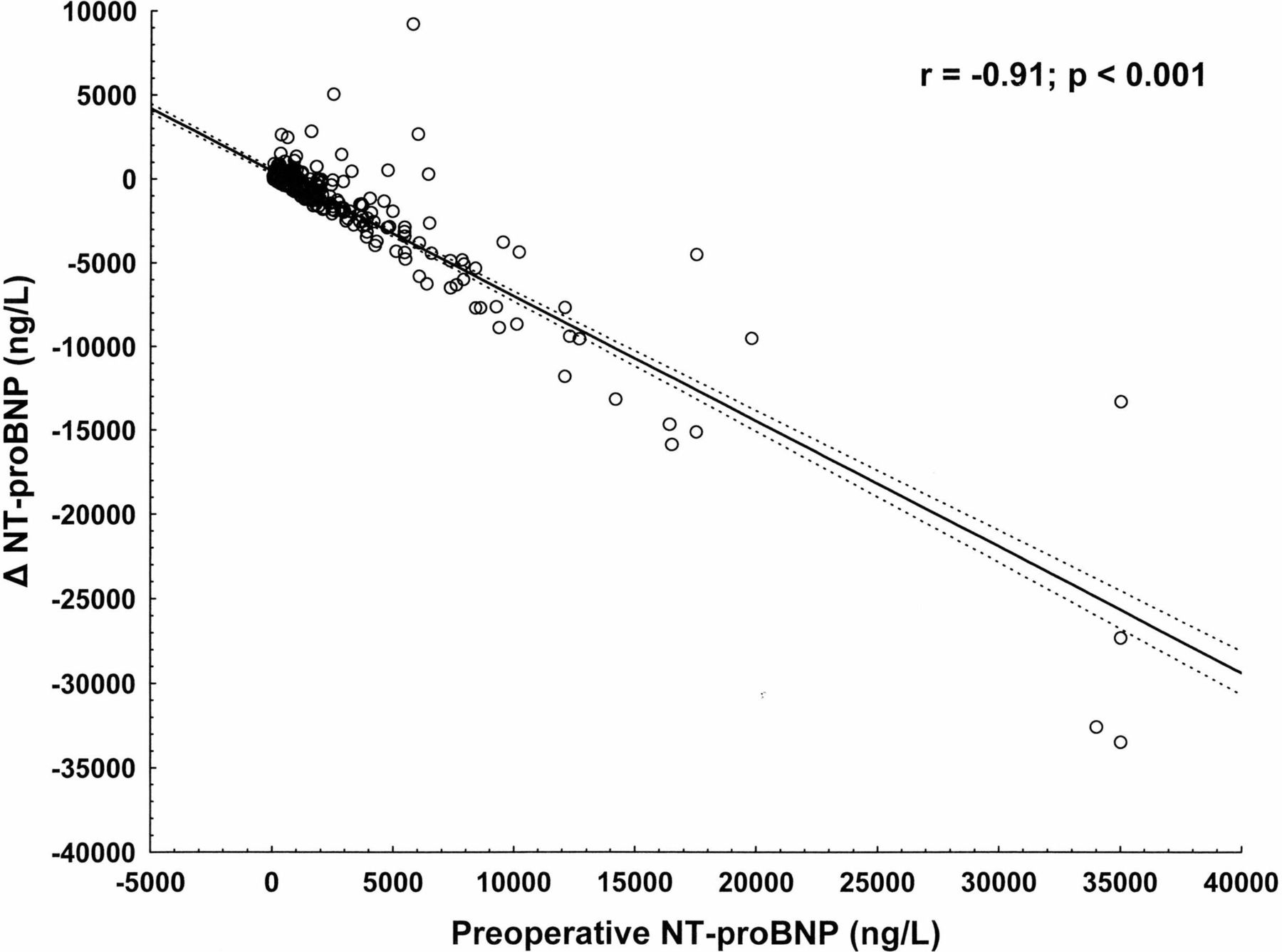
A significant correlation was seen between preintervention NT-proBNP and a decrease in NT-proBNP from preintervention to 6-month follow-up (r=−0.9; P<0.01) for the whole cohort (figure 2). No significant correlation was found between CCT or ECCT and ΔNT-proBNP from preoperatively to the third postoperative day, r=−0.004; P>0.99 respectively r=−0.025; P>0.99 in the All-SAVR group.

{kind=link}
{kind=link}
Correlation between the N-terminal pro-B-type natriuretic peptide (NT-proBNP) change from preoperatively to 6-month follow-up (ΔNT-proBNP) and the preoperative levels of NT-proBNP.
Comparisons of NT-proBNP between the groups are shown in table 2. The TAVI group had higher levels of NT-proBNP preoperatively both at enrolment and prior to the intervention and lower levels at day 3 compared with the AS-SAVR group.
Comparison of NT-proBNP (ng/L) between the groups
The three multivariable linear regression models for variables associated with the postoperative rise of NT-proBNP for all the patients, for the All-SAVR group and for the TAVI group are presented in table 3. For the whole cohort, left ventricular ejection fraction <45%, surgical AVR and postoperative heart failure were related to the postoperative NT-proBNP elevation.
Multivariable linear regression models to test the relationship between the maximum rise of NT-proBNP and other clinical variables
Patients who at enrolment had NT-proBNP >URL had a shorter waiting time to intervention compared with those with NT-proBNP <URL, 94 (57–152) and 134 (99–193) days, respectively (P<0.001).
NT-proBNP and mortality
One-year mortality was 3% (n=11) in the SAVR group and 13% (n=16) in the TAVI group, P<0.001. NT-proBNP was significantly higher preoperatively and early postoperatively in the All-SAVR group and in the AS (SAVR) group for those who died within 1 year after surgery. There was no difference in preoperative or early postoperative NT-proBNP levels between survivors and non-survivors in the TAVI group (table 4). NT-proBNP preoperatively and on postoperative days 1 and 3 revealed significant discriminatory power with regard to 1-year mortality in the All-SAVR, AS (SAVR) and AS+CABG (SAVR) groups. ROC analyses performed are presented in table 5. NT-proBNP elevation from preoperative values to the first and third postoperative day did not demonstrate significant discrimination with regard to 1-year mortality.
NT-proBNP (ng/L) values measured before and after surgery in relation to 1-year mortality
ROC analysis with AUC for NT-proBNP and 1-year mortality
Discussion
Main findings
Despite a median of 4 months from preoperative evaluation to intervention, none of the groups increased in NT-proBNP during the waiting time. After an early transient postoperative increase of NT-proBNP, a decrease in NT-proBNP to or below the preoperative level could be seen in all patient groups at the 6-month follow-up. In the All-SAVR group, both the preoperative and the early postoperative NT-proBNP levels were related to 1-year mortality. This association was not found in the patients undergoing TAVI.
NT-proBNP preoperatively
In this study, we found no increase in NT-proBNP prior to aortic valve intervention despite a median waiting time of 126 days in the SAVR group and 121 days in the TAVI group. Interestingly, even though the results of the NT-proBNP measurements were blinded, those patients with NT-proBNP >URL at enrolment had a significantly shorter waiting time compared with those with NT-proBNP <URL. This supports the association between NT-proBNP levels and factors influencing the timing of the intervention, such as the severity of valve disease, heart function and functional class.14 15 Variations in preoperative levels of NT-proBNP in published studies may reflect different timings of the intervention in relation to the disease course and comorbidities.8 16
NT-proBNP dynamics in patients undergoing SAVR
NT-proBNP displayed a steep peaked curve in all of the SAVR subgroups postoperatively. No difference in ΔNT-proBNP from preoperatively to the third postoperative day was seen between the AS (SAVR) and the AS+CABG (SAVR) groups. The AR (SAVR) group demonstrated a significantly smaller increase in ΔNT-proBNP compared with the other groups. Apart from being younger and to a lesser degree being female, the AR (SAVR) group also had significantly lower postoperative levels of NT-proBNP at postoperative days 1 and 3. These differences are probably less dependent on the trauma induced by surgery since CCT and ECCT showed no correlation with ΔNT-proBNP, but rather with patient-related factors including the degree of heart dysfunction.6 8 17
Postoperative NT-proBNP elevation is obviously mainly related to the procedure, but it is also influenced by age, preoperative left ventricular function, degree of perioperative ischaemia as suggested by postoperative CK-MB and postoperative heart failure according to the multivariable linear regression model. The SAVR procedure itself independently correlated to NT-proBNP elevation as demonstrated in the regression model for the whole study population. The negative correlation between LVEF <45% and postprocedural NT-proBNP elevation might be explained by already high NT-proBNP levels preoperatively in patients with low LVEF and who therefore present a lower increase in NT-proBNP.
NT-proBNP dynamics in patients undergoing TAVI
In agreement with previous studies, an elevation of NT-proBNP was seen after both catheter-mediated and surgical intervention, with a less pronounced and earlier peak after TAVI compared with open heart surgery.18–21 The higher concentrations of NT-proBNP preoperatively and at the 6-month follow-up in the TAVI group could reflect the higher risk profile of this group. The earlier and less pronounced peak is probably explained by the less traumatic nature of the TAVI procedure. Furthermore, LVEF and postoperative CK-MB explained 20% of the variance in the postprocedural NT-proBNP elevation.
At the 6-month follow-up, the TAVI group having the highest preoperative level of NT-proBNP displayed the most marked decrease, although still remaining on a significantly higher level than the other groups. On the other hand, all the groups, except for the TAVI group, had a median NT-proBNP level below the age-related URL, which may have prevented a significant reduction of NT-proBNP in these groups.
NT-proBNP and mortality
There is an ongoing debate on the optimal timing of surgery and valve implantation and the benefit of serial measurements of NT-proBNP.22 Our results show that high preoperative and early postoperative NT-proBNP is associated with postoperative mortality in SAVR, and this is consistent with previous studies.23–25 An intervention to correct aortic valve disease has a beneficial effect on NT-proBNP concentrations when elevated preoperatively, even in those patients with the highest preoperative concentrations. On the other hand, we could not find a relationship between preoperative or early postoperative NT-proBNP levels and mortality in the TAVI group. This is in contrast to other studies26 27 but in accordance with the results presented by Seiffert et al.28 A possible explanation might be that postoperative mortality in TAVI in certain circumstances might be more related to periprocedural complications than to preoperative myocardial dysfunction. Another explanation might be that the patients undergoing TAVI are older and they have more comorbidities, which are the suggested common dominant denominators for adverse outcome.29 Thus, the discriminating power of NT-proBNP on mortality is reduced compared with the SAVR group.
Limitations
Even though this is one of the largest cohorts of patients undergoing surgical aortic valve procedures followed prospectively from preoperative evaluation to 6 months postoperatively, one limitation is the low number of events, which allowed detection of cut-off values of NT-proBNP and mortality only in the AS (SAVR) and AS+CABG (SAVR) groups. Some data, such as periprocedural atrial fibrillation and rapid pacing duration in patients undergoing TAVI, with potential to influence postprocedural NT-proBNP were not available in this study.
Conclusions
NT-proBNP in the perioperative course can be used to identify patients at increased risk of 1-year mortality in SAVR but not in TAVI. The dynamics of NT-proBNP showed different patterns in the SAVR and TAVI groups and the levels were higher preoperatively and at the 6-month follow-up in the TAVI group. Intervention had a favourable effect on NT-proBNP independently of pathophysiology, type of procedure and the preprocedural level. High preoperative and early postoperative NT-proBNP values should, however, act as a prognostic warning signal calling for increased attention regarding both diagnostic and therapeutic measures.
Acknowledgments
The authors thank Inger Huljebrant and Miriam Johansson for their excellent work on data collection and patients’ follow-up, and Mats Fredrikson for statistical analyses.
References
Footnotes
Contributors HH, RS, FV: study design, data collection, data analysis, initial drafting, critical review and final revision. JH: data analysis, initial drafting, critical review and final revision. All authors reviewed and approved the final draft of this manuscript. They take full responsibility for all parts of this paper.
Funding Financial support was received from the Medical Research Council of Southeast Sweden (FORSS) and ALF grants from County Council of Östergötland and Linköping University, Sweden.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Regional Ethical Review Board of Ostergotland, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.