Article Text

Abstract
Background Population-based screening for atrial fibrillation (AF) is a promising public health strategy to prevent stroke. However, none of the published reports have evaluated comprehensive screening for additional stroke risk factors such as hypertension and diabetes in a pharmacy setting.
Methods The Program for the Identification of ‘Actionable’ Atrial Fibrillation in the Pharmacy Setting (PIAAF-Pharmacy) screened individuals aged ≥65 years, attending community pharmacies in Canada, who were not receiving oral anticoagulation (OAC). Participants were screened for AF using a hand-held ECG device, had blood pressure (BP) measured, and diabetes risk estimated using the Canadian Diabetes Risk Assessment Questionnaire (CANRISK) questionnaire. ‘Actionable’ AF was defined as unrecognised or undertreated AF. A 6-week follow-up visit with the family physician was suggested for participants with ‘actionable’ AF and a scheduled 3-month visit occurred at an AF clinic.
Results During 6 months, 1145 participants were screened at 30 pharmacies. ‘Actionable’ AF was identified in 2.5% (95% CI 1.7 to 3.6; n=29); of these, 96% were newly diagnosed. Participants with ‘actionable AF’ had a mean age of 77.2±6.8 years, 58.6% were male and 93.1% had a CHA2DS2-VASc score ≥2. A BP>140/90 was found in 54.9% (616/1122) of participants and 44.4% (214/492) were found to be at high risk of diabetes. At 3 months, only 17% of participants were started on OAC, 50% had improved BP and 71% had confirmatory diabetes testing.
Conclusions Integrated stroke screening identifies a high prevalence of individuals who could benefit from stroke prevention therapies but must be coupled with a defined care pathway.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Population-based screening for atrial fibrillation (AF) is a promising public health strategy to prevent stroke. Recently, increasing data are emerging from different countries on AF screening in the community setting; however, more studies are needed on the optimal screening methods, settings and target population applicable to different healthcare systems.
What does this study add?
This study is the first to screen individuals aged 65 years or older for AF using a hand-held ECG device in addition to measuring blood pressure and assessing diabetes risk in the pharmacy setting. This comprehensive stroke-screening programme was conducted in community pharmacies using an existing healthcare infrastructure, which may allow for more sustainability over time. We identified a high prevalence of individuals who could benefit from stroke prevention therapy. Although screening results were provided to the family physician, few individuals with newly diagnosed AF or known AF but undertreated had initiation of oral anticoagulation therapy.
How might this impact on clinical practice?
An integrated community stroke-screening programme is feasible. However, for screening to be effective, it must be coupled with a well-defined care pathway to ensure timely follow-up and treatment.
Introduction
Atrial fibrillation (AF) is the most common cardiac rhythm disorder1 and a leading cause of stroke.2 AF-related strokes are severe2 ,3 and costly,4 ,5 yet are highly preventable.6 ,7 There is great interest in population AF screening, using different screening technologies in a variety of settings,8 particularly among individuals aged 65 years or older in whom guidelines would recommend initiation of oral anticoagulation (OAC) therapy for detected AF.9 In two population-based studies10 ,11 of systematic AF screening using a single-time-point 12-lead ECG, an AF incidence of 1.5% was found in participants aged 65 years or older. The prevalence of undiagnosed AF was found to be twice as high when systematic AF screening was performed among those aged 75 and 76 years in Sweden using twice daily intermittent, ambulatory ECG recordings over a 2-week period.12 The STROKESTOP study12 demonstrated a very high rate of patient participation and acceptance of OAC therapy among elderly Swedes with newly diagnosed AF; however, implementing a similar screening programme may not be feasible in countries with differing models of healthcare delivery. This has necessitated the need for alternative AF screening strategies including programmes that build on an existing healthcare infrastructure, which may allow for more sustainability over the long term.
Pharmacies may provide an ideal setting for community-based AF screening; however, at present, data are limited in this setting.13 It has been estimated that 90% of the general population visits a pharmacy at least once a year.14 Patients with certain chronic diseases, which predispose to developing AF (such as hypertension and diabetes) visit the community pharmacist five times more frequently than their physician or other healthcare providers.15 Pharmacists are highly accessible and are often the first point of entry into the healthcare system.16 ,17 They can be an essential link between patients and other healthcare providers and have a proven record of management of cardiovascular risk factors.16 ,18–20 In an Australian study13 of 1000 pharmacy customers aged 65 years and older, AF screening with pulse check and smartphone-based ECG was found to be a feasible and cost-effective screening strategy with new AF diagnosed in 1.5% of screened individuals. Pharmacists strongly felt that sustainability of an AF screening programme was linked to combining it with other cardiovascular screening services.21
We thus undertook an integrated AF and stroke risk factor screening initiative among individuals aged 65 years or older who were attending a community pharmacy in two Canadian provinces.
Methods
Study design
The Program for the Identification of ‘Actionable’ Atrial Fibrillation: In the Pharmacy Setting (PIAAF-Pharmacy) was a prospective cohort study of community-based screening to identify ‘actionable’ AF in Alberta and Ontario pharmacies between October 2014 and April 2015. The Human Research Ethics Committee at the University of Alberta (Pro00048198) and the Hamilton Integrated Research Ethics Board approved the study. A total of 30 pharmacies (15 in each province) were invited to participate in the study. Each pharmacy had a study team comprising a pharmacist, a session coordinator and volunteers. Each member of the team was educated using an online module on AF, hypertension, diabetes and screening tools. Any person aged 65 years or older entering the pharmacy was eligible to participate in one screening session unless they were unable to provide consent or were known to have AF and taking OAC therapy. AF history was based on self-report. Screening sessions were advertised through local newspapers, flyers displayed within each pharmacy, verbal notification from the pharmacists, social media, Heart and Stroke Foundation of Canada and pharmacy websites, and through AF screening information sessions conducted in conjunction with senior activities.
Screening procedures
After informed written consent was obtained, a volunteer recorded participant demographics, comorbidities and medications and then helped the participant complete a 15-min assessment consisting of (1) a 30 sec, single-lead ECG using a hand-held device (HeartCheck, CardioComm); (2) two automated blood pressure (BP) readings using a validated BP kiosk (PharmaSmart); and (3) completion of the Canadian Diabetes Risk Assessment Questionnaire (CANRISK) diabetes questionnaire (for participants aged 65–74 years).22 This questionnaire is validated, and predicts a 1% annual incidence of diabetes for low-risk individuals, 17% for intermediate-risk individuals and 33% risk among high-risk individuals. Educational material and counselling on stroke risk factors was provided to each participant along with an opportunity to speak with the pharmacist. Single-lead ECG readings were downloaded to CardioComm by the session coordinator, read by a technician and confirmed independently by two study cardiologists. Each single-lead ECG had a predetermined score assigned for the quality of the recording as determined by a cardiologist: 1-excellent (atrial activity clearly visible or absent), 2-acceptable (atrial activity not reliably seen but rhythm interpretation possible on the basis of the R-R interval), 3-poor (excessive noise or poor contact) and 4-uninterpretable. Participants who were suspected of having AF on the single-lead ECG were recommended to have a 12-lead ECG within 24–72 hours. If the 12-lead demonstrated a sinus rhythm, external cardiac monitoring was recommended. A letter outlining screening results and recommendations was provided to the participant, pharmacist and family physician (FP). A 6-week follow-up visit with the FP was suggested for participants in whom screening detected AF, and these patients all had a scheduled 3-month follow-up at a local AF clinic. At the 3-month visit, participants with ‘actionable AF’ were asked the following questions: (1) if they were aware that AF could increase risk of stroke (yes or no); (2) Were they satisfied with the screening session? (very satisfied, somewhat satisfied, not satisfied); and (3) Were they satisfied with the educational material provided during the session? (very satisfied, somewhat satisfied, not satisfied). BP measurement and medication review was also performed to assess for initiation of OAC therapy.
Primary outcome
The primary outcome was the prevalence of ‘actionable’ AF, defined as newly diagnosed AF, or previously diagnosed AF in an individual who was not receiving OAC. AF was defined as a 30 sec, single-lead ECG recording with irregular rhythm without p-waves.
Secondary outcomes
Secondary outcomes included: (1) rates of suboptimal BP control (≥140/90 mm Hg or ≥130/80 if history of diabetes) among participants with and without known hypertension (2) rates of low, intermediate and high risk for diabetes; (3) feasibility of a combined cardiovascular screening programme in the pharmacy setting as determined by enrolment rate; (4) use of OAC therapy in participants with ‘actionable’ AF at 3 months; (5) quality (excellent, acceptable, poor, uninterpretable) of ECG recording; and (6) agreement between the technician's interpretation and the Cardiologist's interpretation of single-lead ECG.
Statistical analysis
We hypothesised that the prevalence of ‘actionable’ AF detected by screening participants aged ≥65 years using a single-lead ECG will be higher than 1%. Assuming a 2% prevalence of ‘actionable’ AF and a two-sided significance level of 5%, an error margin of 0.6% (absolute) around this prevalence is desirable (95% CI 1.1% to 2.9%) where the lower bound of the 95% CI of 1.1% is the level below which screening of AF is likely to be not cost-effective. Based on these assumptions, the required sample size was 1000 participants. Continuous variables are reported as means±SD and categorical variables as numbers and percentages. For continuous variables, the Wilcoxon test was used and χ2 test for proportions. ‘Actionable’ AF was expressed as true positives divided by the total number screened with the accompanying 95% Poisson CIs. The level of agreement between the technician's interpretation and the cardiologist's interpretation of the single-lead ECG was calculated using Cohen's κ. Two-tailed p values of <0.05 were considered significant.
Results
Participation
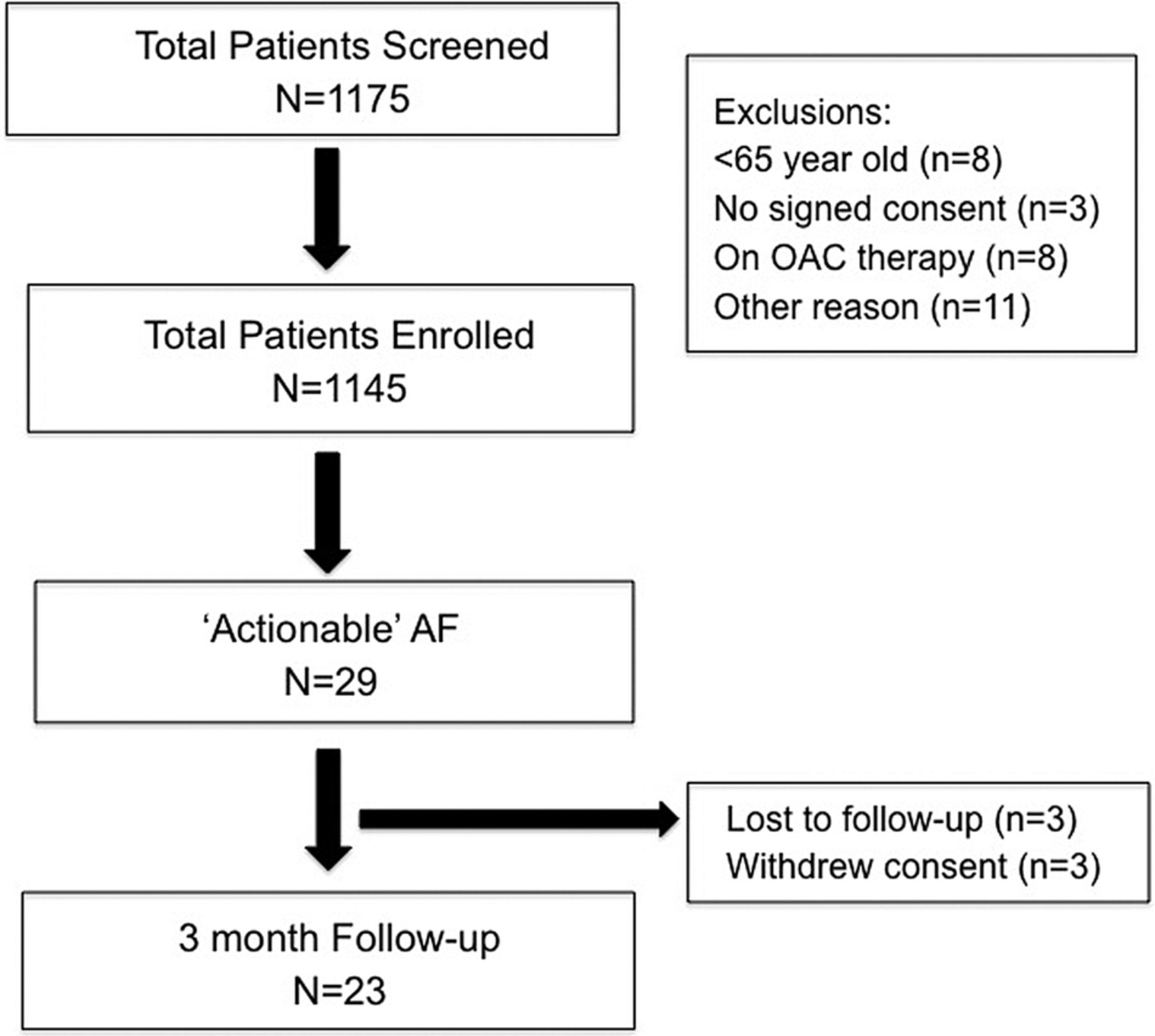
A total of 1175 participants attended a screening session (figure 1). Of these patients, 30 were excluded for the following reasons: 8 were aged under 65 years, 3 did not sign the consent form, 8 were on OAC therapy and 11 had other reasons for not participating, leaving 1145 participants in the PIAAF-Pharmacy study.

Participation in opportunistic screening for AF among those aged 65 years or older in community pharmacies. AF, atrial fibrillation; OAC, oral anticoagulation.
Prevalence of ‘actionable’ AF
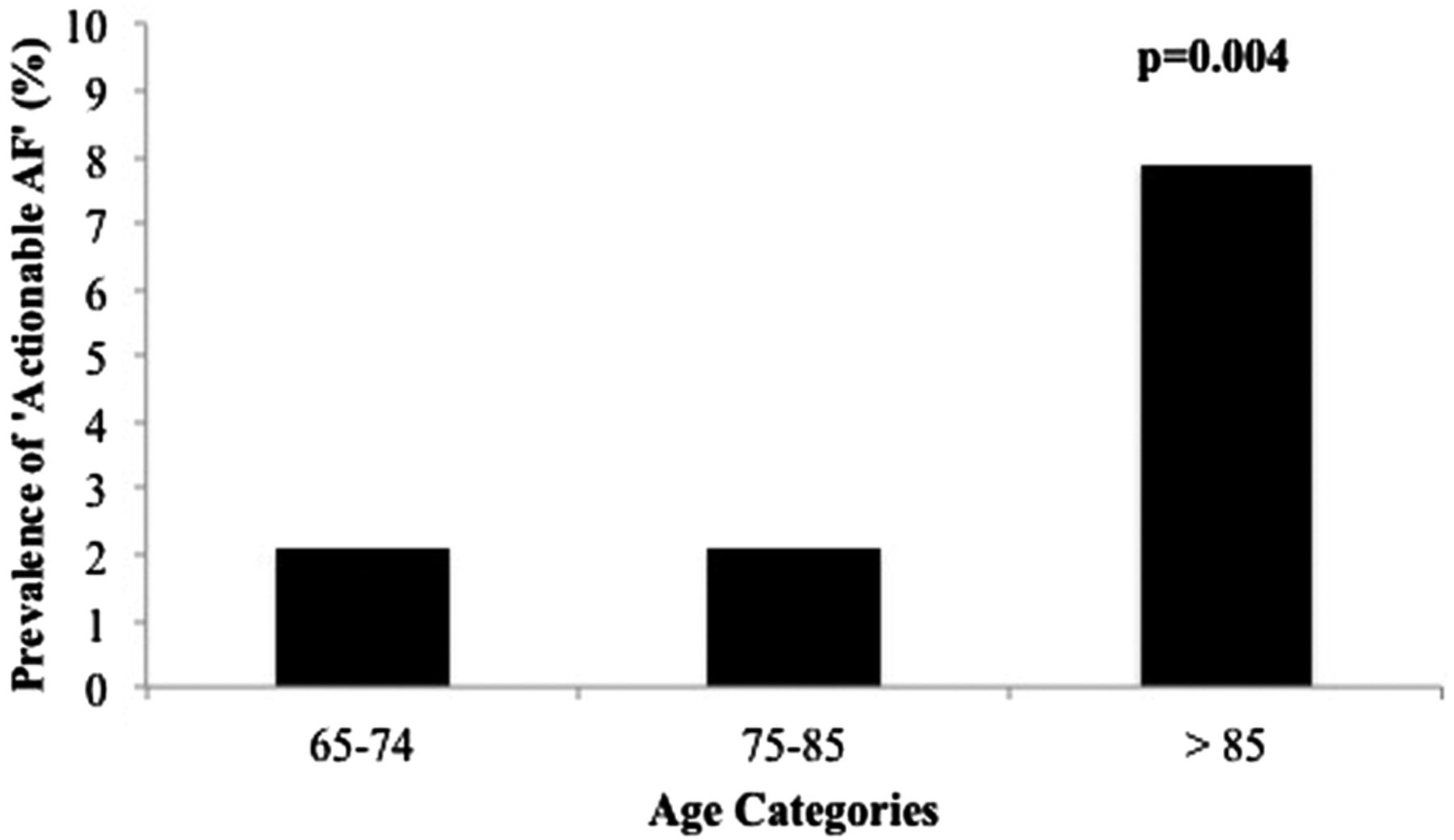
The prevalence of ‘actionable’ AF was 2.5% (95% CI 1.7 to 3.6; n=29); of these 27 patients had newly diagnosed AF (2.4% (95% CI 1.6 to 3.4)). The prevalence of ‘actionable’ AF according to age categories is shown in figure 2 (p=0.004). The prevalence increased with age, and was 7.9% among individuals aged >85 years. Baseline characteristics are shown in table 1. Participants with ‘actionable AF’ had a mean age of 77.2±6.8 years; 58.6% were male and 93.1% had a CHA2DS2-VASc score ≥2.
Baseline characteristics of participants in the PIAAF-Pharmacy study
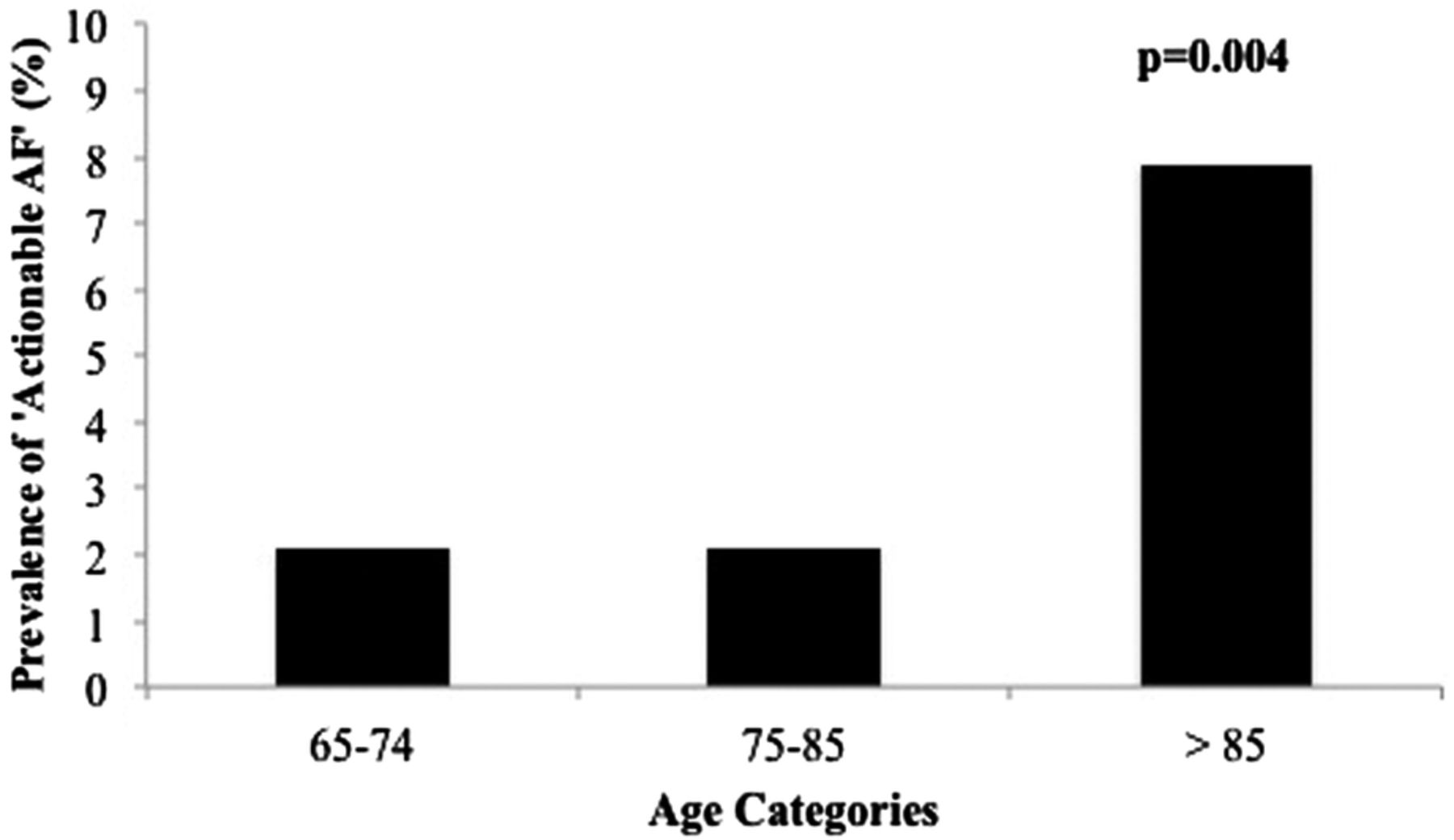
Prevalence of ‘actionable AF’ by age groups. AF, atrial fibrillation.
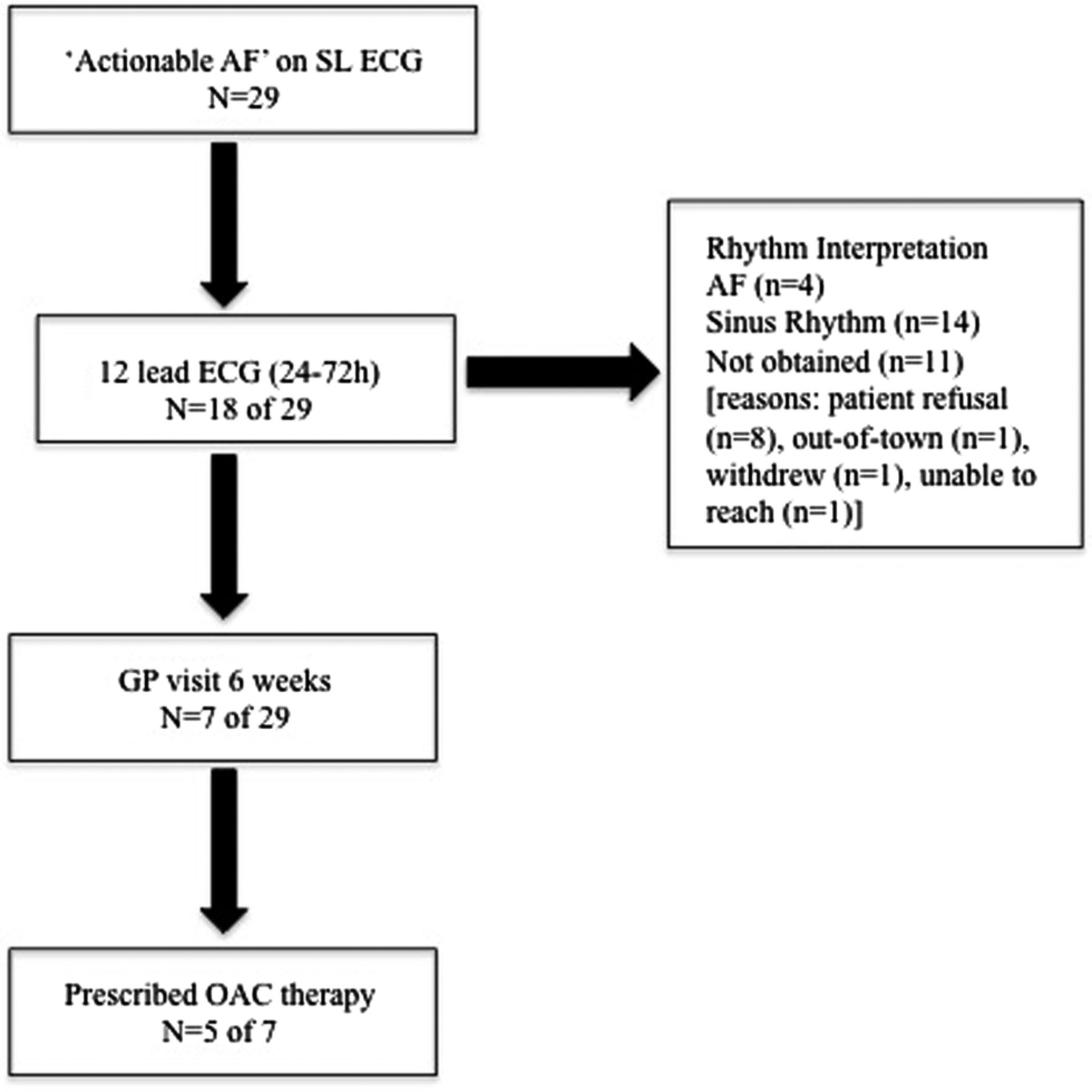
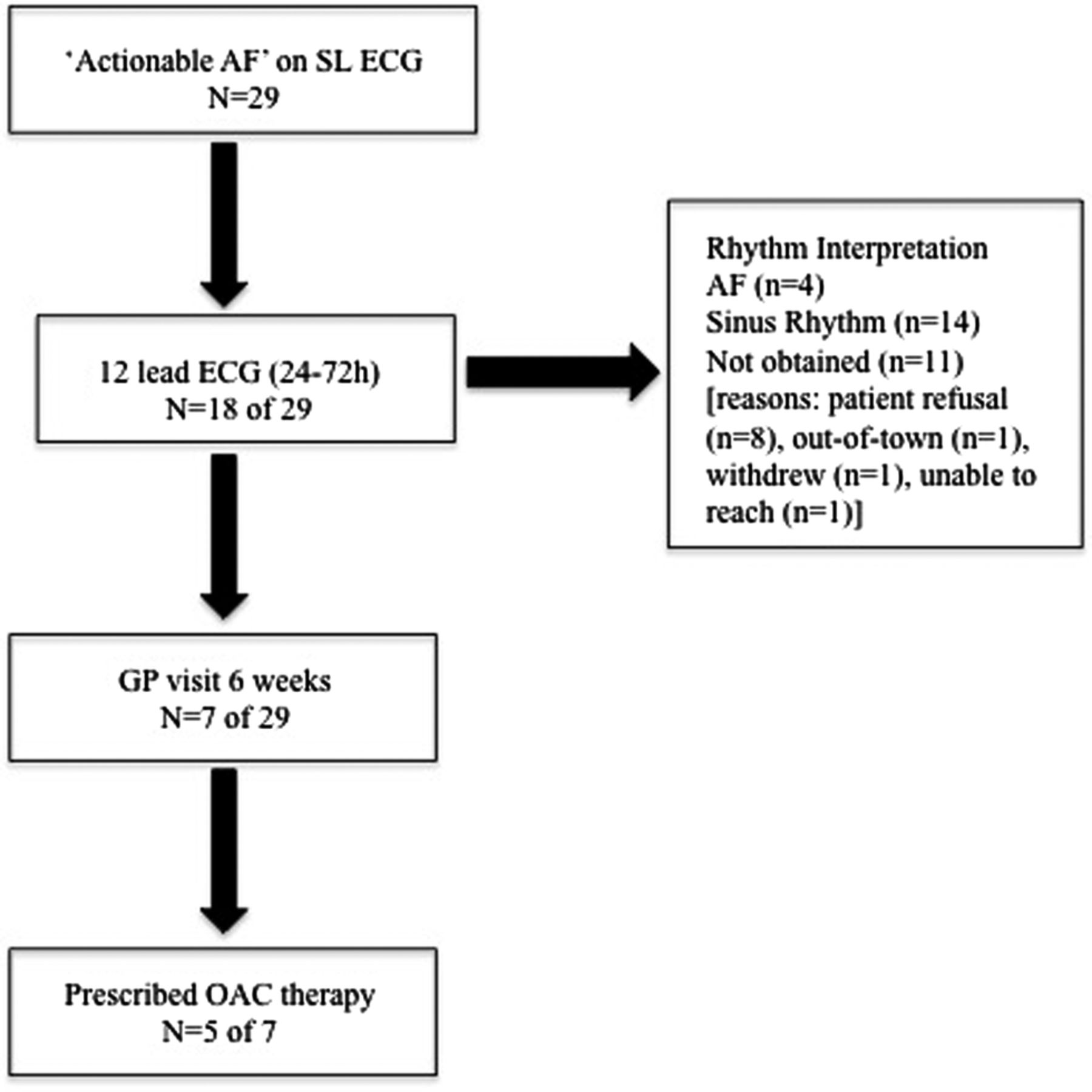
A 12-lead ECG was performed in 18/29 participants with ‘actionable’ AF (figure 3). AF was demonstrated in four participants while the remainder were in sinus rhythm. Of the 29 participants with ‘actionable’ AF, 7 were seen within 6 weeks by their FP or in an AF clinic because there was no FP (n=1).
{kind=link}
{kind=link}
{kind=link}
Flow of participants with ‘actionable AF’ with a SL ECG. AF, atrial fibrillation; GP, general practitioner; OAC, oral anticoagulation; SL, single-lead.
BP and diabetes screening
Over half of all participants screened (616/1122) were found to have a suboptimally controlled BP (table 2). Of the participants with a history of hypertension, 58.2% (249/428) were found to have a BP≥140/90 mm Hg, and 77.7% (122/157) with both a history of hypertension and diabetes were found to have a BP≥130/80 mm Hg. Among participants without a history of hypertension, 42.7% (204/478) were found to have an average BP≥140/90 mm Hg. Of patients found to have ‘actionable’ AF, 51.7% (15/29) had suboptimal BP.
Distribution of blood pressure and atrial fibrillation (AF) status
The CANRISK diabetes risk questionnaire was completed for 492 participants who were aged between 65 and 74 years without a known history of diabetes. The majority of screening participants were found to have an intermediate (231/492, 47.0%) or high risk (214/492, 43.4%) for diabetes. The risk of diabetes according to AF status is shown in table 3.
Diabetes risk and atrial fibrillation (AF) status
Three-month follow-up for ‘actionable’ AF
For participants with ‘actionable’ AF, 23/29 attended a 3-month follow-up visit in an AF clinic. During the 3-month visit, the vast majority of participants (19/23) were aware that AF increased the risk of stroke. All participants were very satisfied (18/23) or somewhat satisfied (5/23) with the screening session and 96% were very satisfied or somewhat satisfied with the educational material provided on stroke risk factors. The 12-lead ECG demonstrated AF in 5 participants, sinus rhythm in 16 participants and was not performed in 2 patients. Of the participants with ‘actionable’ AF who were seen by their FP or in AF clinic at 6 weeks (7 of the 29), five were started on OAC. Of the participants with uncontrolled BP, half had BP control at follow-up and 71% were further assessed for a diagnosis of diabetes with a confirmatory blood test. At the 3-month visit, another eight patients were prescribed OAC therapy, one had a watchman device; one had haematuria and eight preferred no OAC. Of the eligible patients, 61.9% (13/21) were prescribed appropriate stroke prevention therapy.
Following the screening session, one patient who had a history of stroke was seen in the emergency department (ED) and was found to have AF on single-lead ECG and sinus rhythm on 12-lead ECG at 6 weeks but was not started on OAC. Subsequently, the patient had ECG-documented AF, which converted to sinus rhythm at the time of an ED visit. OAC therapy was started at the 3-month follow-up visit. No participants were hospitalised because of AF.
ECG data
The quality of ECG recording was categorised as excellent in 421 (37.0%), acceptable in 642 (56.4%) and poor in 75 (6.6%). There were 14 of the 75 poor single-lead ECGs which were completely uninterpretable (1.2%). For the single-lead ECG interpretation, the simple κ statistic between the technician's interpretation and the cardiologist's interpretation was κ=0.79 (CI 0.75 to 0.83).
Discussion
To the best of our knowledge, this large, community-based AF screening programme is the first to include integrated screening for additional stroke risk factors in the pharmacy setting. Among patients aged ≥65 years, 2.5% had ‘actionable’ AF identified, for which they were not currently receiving guideline-recommended OAC therapy. Among these individuals, nearly 60% also had suboptimally controlled BP and 80% were at intermediate or high risk for developing diabetes, two additional conditions which could be treated to improve cardiovascular outcomes. The screening programme was well received by participants and over 80% demonstrated retained learning regarding the risk of stroke due to AF. However, despite sending the FP a summary of screening results, a copy of the cardiologist-interpreted single-lead ECG and a summary of the Canadian AF guidelines, only 17% of patients identified to have actionable AF had been started on OAC at 3 months.
In our study, we found that among participants with ‘actionable’ AF, a recommendation for a 6-week follow-up with their FP occurred less than a quarter of the time. Similarly, an AF screening study in Belgium found that OAC use was low with only 5.4% of eligible participants with ‘actionable’ AF taking OAC therapy after being provided instructions to consult their general practitioner or cardiologist.23 In comparison, in the STROKESTOP study,12 almost all (>99%) of the participants offered a structured follow-up with a cardiologist attended an appointment and 74% with ‘actionable’ AF were initiated on OAC. There are several explanations that could account for the lower rates of follow-up visits and initiation of OAC in our study including the absence of a scheduled FP visit; follow-up was left to the discretion of the FP who may have not read the screening letter and/or agreed with recommendations or deferred scheduling because of the 3-month specialist visit. Participants and pharmacists who were also provided with letters of screening results and recommendations may have left the decision to the FP and taken less of an active role. Our study highlights the challenge of screening without a rigorous plan for follow-up and although this may be a reflection of real-world practice, improved care pathways are needed so stroke screening is linked to the initiation of stroke prevention therapies. This may involve direct access to AF clinics, or increased pharmacist's involvement through prescribing OAC in collaboration with FPs.
In a systematic review of AF screening studies that included 30 cross-sectional studies and 122 571 patients using a single-time-point screen with either pulse check or ECG across any setting, the incidence of newly diagnosed AF was 1% in patients overall, increasing to 1.4% in patients aged 65 years or older.8 The two studies10 ,11 included that were population-based found a 1.5% incidence of previously undiagnosed AF using systematic AF screening with a 12-lead ECG. This finding was consistent with the only opportunistic AF screening study (SEARCH-AF) performed in Australian pharmacies using pulse check and a single-lead ECG in the pharmacy setting.13 Our study also performed in pharmacies using a hand-held ECG device alone and found a higher incidence of previously undiagnosed AF, a difference that can be attributed to the number of participants over the age of 85 years in whom AF was detected (n=7; incident AF 7.9%) compared with none in the SEARCH-AF study. It may also be possible that participants attending screening sessions were unaware of a prior diagnosis of AF, which would have lowered our rate of incident AF.
Prior work18 ,19 have shown that community pharmacies are an effective setting for screening of cardiovascular risk factors and that pharmacist involvement in disease monitoring and optimisation of drug therapies for cardiovascular risk factors increases adherence to guideline-directed targets and improves outcomes.19 ,20 There are several reasons to explain this positive impact: (1) pharmacists are highly accessible, particularly important since physicians are managing a higher prevalence of chronic diseases, resulting in patient healthcare demands that can often exceed their capacity to address them;24 ,25 (2) pharmacists are consistently ranked as highly trusted professionals,26 allowing them to establish important patient–provider relationships; and (3) pharmacies are frequently visited and may allow screening to extend to individuals who do not access traditional healthcare settings. However, pharmacy screening can introduce a selection bias for several reasons: individuals who visit pharmacies may be ‘healthier’ because they perform activities such as going to the pharmacy; those who visit pharmacies more frequently may be able to take advantage of occasional screening sessions and individuals who attend screening session may already suspect they have the condition.
Our study demonstrated that a comprehensive approach to stroke prevention that includes AF screening is feasible in the pharmacy setting. AF screening can also be integrated with other pharmacist-run programmes such as vaccinations. A recent study from 10 primary care practices in the Netherlands found newly diagnosed AF in 1.3% of participants aged 65 years or older during a single screening session performed for influenza vaccination.27
In the few studies that exist, opportunistic AF screening has been cost-effective.28 In a clinical trial among patients aged 65 years or older comparing systematic AF screening (12-lead ECG) or opportunistic AF screening (pulse check and 12 lead if pulse was found to be irregular) with routine care, opportunistic screening was found to be more cost-effective.29 These data currently are the basis of the only AF screening guidelines.30 Recent advances in ECG technology have contributed to lowering the cost of screening. The SEARCH-AF study performed a modelled cost-effective analysis extending pharmacy-based iPhone ECG AF screening to the community for those aged 65–84 years and found an incremental cost-effectiveness ratio of €3142 (US$4066) per quality-adjusted life-year with warfarin and €30 481 (US$20 695) for preventing one stroke, estimates lower than acceptable thresholds.13 Our study uses comparable technologies and also extends screening to include other cardiovascular risk factors, making it an attractive approach for AF screening.
Limitations
There are several limitations to our study that warrant discussion. First, screening was performed at a single time point, and therefore we most likely missed participants with paroxysmal AF. Second, volunteers and research staff but not pharmacists implemented screening sessions, and as such, understanding how an integrated cardiovascular screening programme could be integrated into a pharmacist's daily workflow is less clear. Prior work16 ,18 ,19 has demonstrated that it is feasible for pharmacists to perform AF, BP and diabetes screening. Third, single ECG interpretations required a cardiologist for interpretation because the hand-held ECG device did not have a built-in AF algorithm to provide real-time results. This may change with the development of highly specific automatic algorithms for AF detection.31 Fourth, we could have overdiagnosed some cases of new AF when participants could have had a prior diagnosis and were unaware because history of AF was based on self-report alone. However, the prevalence of ‘actionable’ AF remains unchanged since these patients were not on OAC therapy and our definition of ‘actionable’ includes both newly diagnosed and previously diagnosed AF when anticoagulation was not prescribed. Fifth, the lack of confirmation of AF diagnosis on a subsequent ECG could imply a higher rate of paroxysmal AF or false positives. Sixth, the CANRISK questionnaire's intended use is among patients aged 40–74 years and given the age of our screening population, we may have missed participants who could have benefited from an additional blood test for confirmation of type 2 diabetes with an alternative questionnaire. Seventh, we were not able to determine the screening denominator because of the overlap in catchment area. Finally, we had scheduled follow-up for only patients with ‘actionable’ AF and therefore were unable to determine whether abnormal screening results for BP and diabetes resulted in a change in management for these two conditions among participants without AF.
Conclusions
Integrated cardiovascular screening in the pharmacy identifies a significant proportion of ‘actionable’ AF and other modifiable stroke risk factors. Comprehensive, community-based screening for stroke risk factors is a promising public health strategy and to be effective must be coupled with a well-defined care pathway to ensure timely follow-up and treatment. Future studies are needed to connect screening results with next steps to management.
References
Footnotes
Funding The PIAAF-Pharmacy study was supported by the Canadian Stroke Prevention Intervention Network, Boehringer Ingelheim and in-kind support from CardioComm. RKS received a grant from the University Hospital Foundation. JSH has a personnel award from the Heart and Stroke Foundation, Ontario Provincial office (MC7450).
Competing interests FRQ has received consulting fees from Boehringer Ingelheim and Servier and has research grants from Boehringer Ingelheim and Bayer. DC has consulting fees from Daiichi-Sankyo, Boehringer Ingelheim, Bayer, Pfizer and Bristol-Myers Squibb; research grants from Daiichi-Sankyo, Boehringer Ingelheim, Bayer, Pfizer and Bristol-Myers Squibb. SJC receives consulting fees from Bristol-Myers Squibb and JSH has research grants from Boehringer Ingelheim, Bayer, Pfizer and Bristol-Myers Squibb.
Ethics approval Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.