Article Text

Abstract
Objective Microvascular obstruction (MVO) and intramyocardial haemorrhage (IMH) are known complications of myocardial ischaemia-reperfusion injury. Whereas MVO is an established marker for a poor clinical outcome, the clinical significance of IMH remains less well defined. Cardiovascular MR (CMR) and T2 weighted short tau inversion recovery (T2-STIR) imaging have been used to detect IMH and to explore its clinical importance. IMH is typically identified within the area-at-risk as a hypointense signal core on T2-STIR images. Because MVO will also appear as a hypointense signal core, T2-STIR imaging may not be an optimal method for assessing IMH. In this study, we sought to investigate the ability of T2-STIR to discriminate between MVO with IMH in a porcine myocardial ischaemia-reperfusion model that expressed MVO with and without IMH.
Method MVO with and without IMH (defined from both macroscopic evaluation and T1 weighted CMR) was produced in 13 pigs by a 65-min balloon occlusion of the mid left anterior descending artery, followed by reperfusion. Eight days after injury, all pigs underwent CMR imaging and subsequently the hearts were assessed by gross pathology.
Results CMR identified MVO in all hearts. CMR and pathology showed that IMH was present in 6 of 13 (46%) infarcts. The sensitivity and specificity of T2-STIR hypointense signal core for identification of IMH was 100% and 29%, respectively. T2-values between hypointense signal core in the pigs with and without IMH were similar (60.4±3 ms vs 63.0±4 ms).
Conclusions T2-STIR did not allow identification of IMH in areas with MVO in a porcine model of myocardial ischaemic/reperfusion injury in the subacute phase of a reperfused myocardial infarction.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Cardiovascular MR (CMR) using T2 weighted imaging with short tau inversion recovery (T2-STIR) is being used to detect microvascular obstruction (MVO) with intramyocardial haemorrhage (IMH) as markers of myocardial ischaemia-reperfusion. However, the validity of T2 weighted CMR in assessment of IMH has not been tested.
What does this study add?
In this study, we find that T2-STIR does not discriminate between MVO and IMH in an experimental model of myocardial ischaemia-reperfusion that expresses MVO with and without IMH during the subacute phase of a reperfused myocardial infarction.
How might this impact on clinical practice?
A comprehensive multicontrast CMR protocol is needed to evaluate the presence of MVO and IMH in acute myocardial infarction.
Introduction
Timely reperfusion is mandatory to salvage ischaemic myocardium and to reduce mortality in acute myocardial infarction.1 Reperfusion following prolonged ischaemia may, however, injure the myocardial microvasculature and cause microvascular obstruction (MVO).2 This is a serious condition because it prevents adequate myocardial blood perfusion despite patent coronary arteries. Severe myocardial microvascular injury may also trigger intramyocardial haemorrhage (IMH) due to extravasation of erythrocytes through the damaged endothelial wall.3–8 Whereas MVO is recognised as a strong predictor of ventricular remodelling and poor clinical outcome, it remains unknown whether IMH further aggravates the clinical outcome.9 To determine the clinical consequences of IMH, it is essential to develop a reliable, non-invasive imaging technique capable of differentiating between MVO, and MVO with IMH.10 ,11 Cardiovascular MR (CMR) utilises first-pass perfusion imaging and T2-weighted images to detect MVO and IMH. Specifically, T2 weighted short tau inversion recovery (T2-STIR) imaging was applied to detect IMH6 ,7 and to investigate the prognostic value of IMH defined from T2-STIR.6 ,7 ,12 ,13 Within the area-at-risk (AAR), usually identified by T2-weighted imaging as oedema, a hypointense core on T2-STIR images has been ascribed to paramagnetic effects of haemoglobin breakdown products, and has consequently been considered indicative of IMH.14 ,15 However, because MVO consists of non-oedematous tissue, a hypointense signal core within the AAR may not be specific for IMH.16 MVO and IMH represent two separate pathologies but often appear simultaneously since IMH is highly associated with MVO.16 We investigated the ability of T2-STIR imaging to detect IMH and to discriminate between IMH and MVO using a unique porcine model of myocardial ischaemia-reperfusion that expresses MVO and MVO with IMH.17
Methods
Animal model
Fifteen female Danish Landrace pigs each weighing ∼40 kg were used for the experiments. The pigs were presedated with an intramuscular injection of Stressnil (1 mL/kg) and midazolam (1 mL/kg). After induction of anaesthesia with intravenous propofol (3.33 mg/kg) and endotracheal intubation, anaesthesia was maintained with sevoflurane (2.5%) and continuous rate infusion of fentanyl (3 mg/kg/h). The pigs were mechanically ventilated with a tidal volume of 425 mL (12 ventilations/min). By ultrasound guidance, an 8 F introducer sheath was inserted into the right common femoral artery. This was followed by an intravenous bolus injection of heparin (100 IU/kg). Coronary occlusion was induced by placing a 2.5 mm angioplasty balloon in the left anterior descending coronary artery (LAD) distal to the second diagonal branch artery and inflating it to 10 atm. The balloon occluded the LAD for 65 min, and was then deflated and removed. A coronary angiogram was performed following balloon inflation, to confirm occlusion, and also following balloon deflation, to confirm reperfusion. The animals were randomised to receive either intracoronary infusion of saline or dimethyl sulfoxide during reperfusion as a potential adjunctive therapy to reduce reperfusion injury. The details of the experimental protocol are described elsewhere.17
During the procedure, heart rate, ECG, blood pressure, temperature and oxygen saturation were continuously monitored. Ampicillin (2 mg) was administrated intravenously before and after the procedure, and acetylsalicylic acid (100 mg/day) was given orally after the procedure and continued until euthanasia. To prevent ventricular fibrillation, 150 mg of amiodarone was administered intravenously prior to the induction of myocardial infarction. If ventricular fibrillation was encountered, non-synchronised direct current defibrillation (150 J) was performed. The paddles were pressed against the anterior chest wall above the sternum on the right side and below the sternum on the left side. At the end of the experiment, the pigs were awakened and returned to their stables, where they stayed for 7–10 days (average 8.5 days) prior to CMR imaging, harvesting and evaluation by gross pathology.
CMR imaging
All the pigs underwent CMR imaging before euthanasia. The sedation protocol was as described above, except that continuous propofol infusion (10 mg/mL, 12 mL/h) was used instead of sevoflurane. CMR was performed on a 1.5 T MR system (Intera, Philips Medical Systems, Best, the Netherlands) with a five-element cardiac synergy coil. All images of the heart were obtained with the pigs in the supine position. First, a survey scan was performed to localise the heart and diaphragm, and then left ventricular (LV) function was assessed using a retrospective, ECG-triggered Balanced-Steady-State-Free-Precession (B-SSFP) breath-hold cine sequence in the cardiac short-axis, vertical long axis and horizontal long axis planes. In the cardiac short-axis, the LV volume was completely encompassed by contiguous 8 mm slices with a spatial resolution of 1.22×1.22 mm and a field of view (FOV) of 288×288 mm. The following imaging parameters were used: repetition time (TR) 3.0 ms; echo time (TE) 1.5 ms; flip angle 60°; 30 heart phases. To ensure a strong T2-weighting, a T2-STIR fast spin echo sequence with a long TE was obtained in the previously mentioned short-axis orientation to assess AAR. The sequence was navigator-gated and cardiac-triggered. The following imaging parameters were used: TR 2400 ms; TE 100 ms; echo train length 20; fat inversion time 180 ms; flip angle 90°; spatial resolution 0.54 mm×0.54 mm in-plane; number of averages 2; slice thickness 8 mm; FOV 320×320 mm; 14 slices.
We obtained T2-mapping in six animals by a multislice spin echo sequence. The sequence was navigator-gated and cardiac-triggered. The following imaging parameters were used: TR 1100 ms; TE (8, 16, 24, 32, 40, 48, 56, 64) ms; flip angle 90°; spatial resolution 1.33×1.33 mm in-plane; slice thickness 8 mm; FOV 320×320 mm; 14 slices.
T1-weighted inversion recovery (T1W-IR) gradient echo (GRE) imaging was obtained in the same short-axis slices for the purpose of identifying IMH, as previously described.18 The sequence was navigator-gated, free-breathing and cardiac-triggered. The following imaging parameters were used: TR 3.5 ms; TE 1.13 ms; flip angle 30°; spatial resolution 1×1 mm in-plane; slice thickness 8 mm (over contiguous slices); FOV 320×320 mm and 14 slices. Before the acquisition of the T1W IR sequence, a TI scout (Look Locker sequence) was performed for the purpose of obtaining the most appropriated TI to null the signal intensity from blood. Typically, the TI was found to be optimal at approximately 500 ms.
Subsequently, gadolinium enhanced first-pass myocardial perfusion and late gadolinium enhancement (LGE) was performed for the purpose of identifying areas of MVO and myocardial infarction, respectively. An intravenous bolus dose of 0.2 mmol/kg Gd-DTPA (Gadobutrol, Gadovist, Bayer Schering Pharma, Berlin, Germany) was administered manually. First-pass perfusion imaging was performed using a fast gradient echo sequence with the following parameters: TR 2.5 ms; TE 1.3 ms; flip angle 18°; spatial resolution 2.8×3.0 mm in-plane; slice thickness 10 mm; FOV 256×256 mm; three slices acquired in the LV short-axis using a 5 mm inter-slice gap.
LGE was acquired 15 min after gadolinium injection, using a three-dimensional phase sensitive inversion recovery-prepared T1-weighted gradient echo sequence with the following parameters: TR 5.78 ms; TE 2.78 ms; echo train length 20; inversion time ∼320 ms; flip angle 25°; spatial resolution 1.5×1.5 mm; slice thickness 8 mm; FOV 350×350 mm; 14 slices acquired in the LV short-axis with no interslice gap. Following CMR, the pigs were kept under anaesthesia and moved to the operating room for organ harvesting.
Harvesting and pathology
Midline sternotomy was performed and a snare placed around the LAD distal to the second diagonal branch at the same site as the previous balloon occlusion. Twenty-five millilitres of 10% Evans blue dye was then injected into the left auricle and allowed to circulate for approximately 10 s, to delineate the AAR.18–20 The animal was subsequently euthanised and the heart excised. The heart was then cut into consecutive 8 mm-thick slices in short-axis planes. Each slice was photographed with a digital camera (Nikon, Tokyo, Japan) for the purpose of registering myocardial infarction, IMH and AAR.
Data analysis
CMR images
One observer (WYK), blinded to the distribution of the groups, analysed all the CMR images, using the semiautomatic, freely available software Segment V.1.9 R3697. First, LV volumes and function were calculated on the end-diastolic and end-systolic phases of the short-axis cine images. Second, myocardial infarct size was determined in the LGE images by a semiautomated algorithm accounting for partial volume effects.21 The infarct size was expressed as a percentage of the LV myocardium (infarction volume/LV myocardium volume×100%). The AAR was quantified from T2-STIR images by a semiautomated algorithm (AAR/LV myocardium volume×100%).22 The salvaged myocardial percentage was defined as the difference between the infarct size and AAR. Finally, the hypointense signal core within the AAR was defined by ROI analysis as a core with signal intensity measuring two SDs lower than the signal intensity of the AAR.23 ,24 The ROI defined by the hypointense signal core was used on the T2-mapping images to extract T2 values. On the T1W IR images, myocardium with mean signal intensity more than two SDs above the mean signal intensity from remote myocardium was defined as IMH (18). MVO was defined and quantified on the LGE images from visual inspection of no contrast enhancement within the infarct core. All CMR images were matched and aligned.
Pathology
Two observers by consensus (SFP and ESSH) analysed all photographed gross pathological images of the myocardial slices using the Adobe Photoshop software (Adobe Systems Inc, San Jose, California, USA). The IMH volume was identified and measured as a distinct red to reddish black area within the AAR of the LV myocardium. MVO was not assessed in the pathology.
Statistics
The significance of group differences was evaluated using the Mann-Whitney U test and the Wilcoxon matched-pairs signed rank test was used to evaluate the amount of IMH in percentage of the left ventricle on T1W IR images compared to gross pathology. Data are presented as mean and 95% CIs. A value of p<0.05 was considered statistically significant. The association between IMH and MVO, and presence of hypointense signal core on T2-STIR images, was tested with a 2-tailed Fisher's exact test. T2-mapping values were tested using a one-way analysis of variance with Holm-Sidak's multiple comparisons correction. Statistical analysis was performed with GraphPad Prism (6.05, GraphPad Software, La Jolla, California, USA).
Results
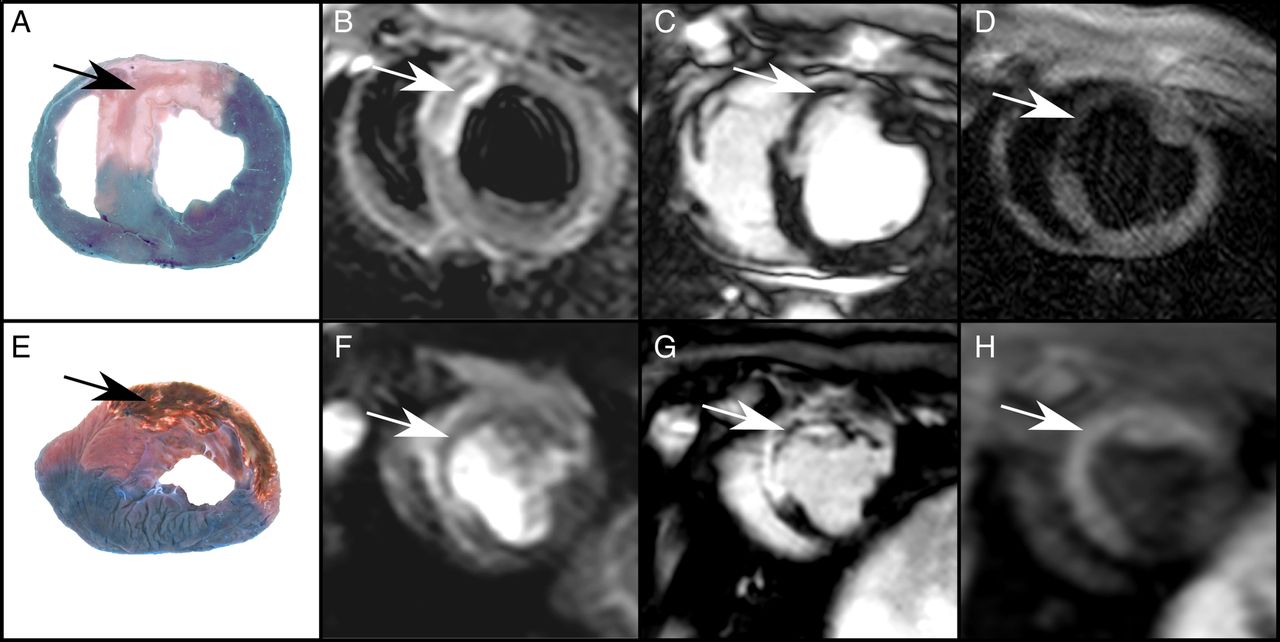
All CMR examinations and experimental procedures were successfully completed. Figure 1 shows representative pathological photographs and CMR images of MVO (−IMH) and MVO (+IMH). Examples from gross pathology assessment are shown in figure 2. The CMR and gross pathology results are summarised in table 1. Two pigs displayed neither MVO nor IMH. Global CMR parameters did not show any significant difference in ejection fraction or LV volumes between the two groups. AAR, infarct size and myocardial salvage also did not show any difference between the groups. The MVO size measured as a percentage of LV on LGE images showed no difference in the MVO (+IMH) group compared with the MVO (−IMH) group, 2.1% vs 1.7%, respectively. The sensitivity and specificity of T2-STIR hypointense signal core to detect IMH was 100% and 29%, respectively, as shown in table 2. T1W IR showed that 0 out of 7 (0%) had IMH in the MVO (−IMH) group compared with 6 of 6 (100%) pigs in MVO (+IMH) group (p<0.01). Wilcoxon matched-pairs signed rank test showed no difference between the IMH % LV measured on T1W IR (range 12–39% LV) compared with gross pathology (range 5–27% LV) (p=0.09, difference 6.4% LV, CI (−2.86 to 15.76), median 5.1%, Q1=2.1, Q3=10.6).
Results of CMR and gross pathology
Sensitivity and specificity of T2-STIR for detection of IMH

Upper row shows myocardial infarction with MVO (−IMH) (indicated by arrows) on pathology (A), T2-STIR (B), late gadolinium enhancement (LGE) images (C) and T1W IR (D). Lower row shows myocardial infarction with MVO (+IMH) (indicated by arrows) on pathology (E), T2-STIR (F) and LGE images (G), and T1W IR (H). IMH, intramyocardial haemorrhage; MVO, microvascular obstruction; T2-STIR, T2 weighted short tau inversion recovery.

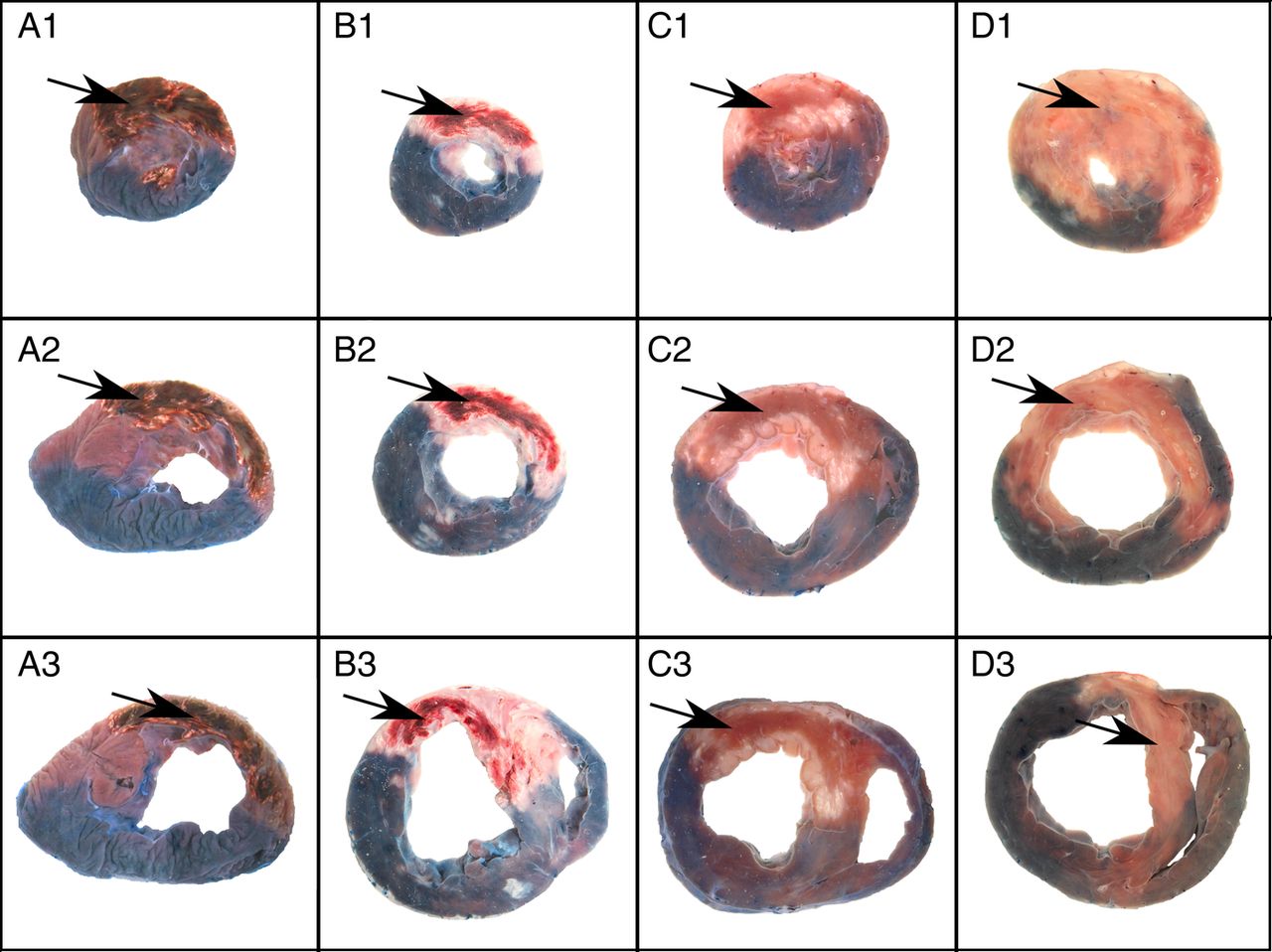
Examples from gross anatomical pathology. A (1–3) and B (1–3) show three slices from two pigs in the MVO (+IMH) group, where the arrows indicated areas defined as IMH. C (1–3) and D (1–3) show three slices from two pigs in the MVO (−IMH) group, where arrows points to the AAR where there is no indication of IMH. AAR, area-at-risk; IMH, intramyocardial haemorrhage; MVO, microvascular obstruction.
The measured T2-values are visualised in figure 3. The T2-values (n=7) from hypointense signal core in MVO (−IMH) (mean 63.0 ms) and hypointense signal core in MVO (+IMH) (mean 60.4 ms) showed no difference (p=0.9, difference −2.57 ms, CI (−9.76 to 4.61)). In the MVO (−IMH) infarcts, the T2-values from remote myocardium (mean 58.3 ms) and the hypointense signal core (mean 63.0 ms) also showed no difference (p=0.9, difference 4.60 ms, CI (−3.66 to 12.9)). Also, in the MVO (+IMH) infarcts, the T2-values from the remote myocardium (mean 58.0 ms) and the hypointense signal core (mean 60.4 ms) showed no difference (p=0.9, difference 2.35 ms, CI (−1.96 to 6.65)). Significant differences in T2-values between infarcted myocardium versus remote, hypointense signal core and salvaged myocardium, are listed in table 3.
Comparison of T2-values from left ventricular myocardium

{kind=link}
{kind=link}
{kind=link}
The mean T2-values with SDs are shown for each location of interest from both groups. IMH, intramyocardial haemorrhage; LGE, late gadolinium enhancement; MVO, microvascular obstruction.
Discussion
The results of this study showed that, within the AAR, a hypointense signal core on T2-STIR images may represent IMH as well as MVO, leaving the specificity for IMH insufficient. No difference was found in T2-values within the hypointense signal core between MVO (−IMH) and MVO (+IMH). Furthermore, no difference was detected in T2 values between hypointense signal core and remote myocardium. This finding illustrates the challenge of defining AAR by T2-weighted sequences during the subacute phase in the presence of reperfusion injury. Gross pathology confirmed our T1W IR CMR findings by showing a perfect match between the two in terms of identifying IMH. In a postmortem study, Jackowski et al25 previously showed that hypointense signal core on T2-STIR images might represent pathologies other than IMH, for example, non-oedematous myocardial tissue; nevertheless, we believe that this study is the first to confirm this assumption by validating the results of T2-STIR imaging against gross pathology in a subacute porcine model of reperfusion injury. In another experimental study, a porcine model of IMH demonstrated a correlation between hypointense signal core on T2-STIR images and histopathologically confirmed IMH.7 In contrast to our study, the porcine model expressed only MVO with IMH. Consequently, the ability of CMR T2-STIR to differentiate between IMH and MVO could not be addressed. Several previous studies have used T2-STIR to detect IMH in patients with acute myocardial infarction for the purpose of exploring its clinical consequences.6 ,12 ,13 ,23 ,26–30 In light of the present results, a comprehensive multicontrast CMR protocol is preferable for evaluation of the clinical consequences of IMH. To increase the accuracy of CMR IMH detection, a multisequence approach with T2*-weighted or T1-weighted sequences has been proposed in addition to T2-STIR.31–33 The T2*-weighted sequences are very sensitive to paramagnetic effects from haemoglobin degradation products, and may be more specific for IMH. However, such sequences are time-consuming, provide negative contrast resulting in signal void and may consequently be vulnerable to motion artefacts. T1-weighted sequences take advantage of the very short T1-relaxation of methaemoglobin, and detect methaemoglobin with positive contrast, which optimises differentiation of IMH from adjacent normal myocardium.18 Since T1-weighted sequences depend on the haemoglobin breakdown product at the methaemoglobin stage, it is only useful in the subacute phase (>7 days).34
Limitations
MVO was only assessed by CMR. Future studies using thioflavin-S staining might be a possible method to identify the MVO zones by pathological examination.35 The presence of IMH on gross pathology was based on visual assessment. Histological analysis of IMH was not carried out due to suboptimal preservation of the hearts. However, the presence of IMH was also demonstrated with T1W IR performed in the subacute phase, which has been demonstrated to be a reliable marker of haemorrhage containing methemoglobin.36 Indeed, we found a perfect agreement between gross pathology and T1W IR on determining the presence of IMH. The presence of IMH in reperfused acute ischaemic myocardium is most likely a continuum of extravasation of minute to large amounts of erythrocytes through severely damaged endothelial cells. Thus, neither visual inspection nor T1W IR CMR may have detected smaller amounts of IHM. Since the optimal time to visualise AAR from myocardial oedema is either acute or after 1 week, it is possible that imaging as late as 10 days postinfarction will result in reduced amounts of oedema within the AAR.
Conclusion
T2-weighted CMR, when performed in the subacute phase, does not allow discrimination between MVO with and without IMH as defined by macroscopic evaluation and T1W IR CMR. A comprehensive multicontrast CMR protocol is needed to evaluate reperfusion-induced IMH in acute myocardial infarction.
References
Footnotes
ESSH and SFP contributed equally.
Contributors ESSH took part in formulating the study design, carried out the CMR scans, contributed with work on the animal model, performed analysis of the CMR and pathology data, performed the statistical analysis and wrote the manuscript with feedback from the co-authors. SFP carried out all the procedures related to the animal model, took part in formulating the study design and drafting of the manuscript, and revised it critically for intellectual content. SBP took part in formulating the study design and drafting of the manuscript, and revised it critically and contributed to important intellectual content of the manuscript. UK contributed to procedures related to the animal model and drafting of the manuscript, and revised it critically for intellectual content. NHS contributed to procedures related to the animal model and drafting of the manuscript, and revised it critically for intellectual content. HEB took part in formulating the study design and drafting of the manuscript, and revised it critically and contributed to important intellectual content of the manuscript. WYK took part in formulating the study design and the CMR sequence setup, analysed the CMR data, contributed towards drafting of the manuscript, and revised it critically and contributed to important intellectual content of the manuscript. All the authors have read and approved the final manuscript.
Funding This work was supported by the Danish Council for Strategic Research (11-115818) and (10-093499), and by a research grant from the Danish Diabetes Academy, supported by the Novo Nordisk Foundation.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.