Article Text

Abstract
Objective The study objective was to assess the association between 24 h ambulatory heart rate (HR), atherosclerosis risk factors and blood pressure (BP) in young non-hypertensive patients.
Methods We recruited 186 participants aged 18–45 years from a large urban academic Family Medicine outpatient practice, serving 40 000 individuals for this observational study. The main analyses were based on multiple linear regression, with mean 24 h BP (systolic BP (SBP) or diastolic BP (DBP)) as the outcomes, mean 24 h HR as the main predictor of interest, and controlling for age, gender, race, insulin sensitivity/resistance and endothelial function measured by strain gauge venous occlusion plethysmography.
Results HR was independently associated with mean 24 h SBP and DBP (SBP and DBP: p=0.042 and 0.001, respectively). In our analyses, associations were markedly stronger for ambulatory compared with office BP measurements. Endothelial dysfunction was associated with higher SBP (p=0.013); plasminogen activator inhibitor-1 was significantly associated with both SBP and DBP (p=0.041 and 0.015, respectively), while insulin resistance was not associated with either SBP or DBP. Insulin resistance and C reactive protein were significant predictors of HR (p=0.013 and 0.007, respectively).
Conclusions These findings suggest that HR may be a potential marker of elevated cardiovascular risk in young asymptomatic individuals, prior to the development of clinical hypertension or cardiovascular disease.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Resting heart rate (HR) is an independent predictor of cardiovascular and all-cause mortality in men and women with and without diagnosed cardiovascular disease.
What does this study add?
Most previous studies of HR have utilised resting HR. Three previous studies which analysed mean 24 h HR, as in our study, recruited individuals much older than those in our study. Our findings suggest that HR may be a potential marker of elevated cardiovascular risk in asymptomatic individuals, prior to the development of clinical hypertension or cardiovascular disease.
How might this impact on clinical practice?
Although epidemiological studies have consistently reported that resting HR is an independent predictor of cardiovascular and all-cause mortality, the importance of resting HR as a prognostic factor and potential therapeutic target is not yet generally accepted. Clinical strategies incorporating HR in risk stratification may have possible future utility in identifying asymptomatic individuals to target with individualised preventive therapy.
Introduction
Heart rate (HR) is a key determinant of coronary blood flow, an established marker of sympathetic nervous system (SNS) activity, and an independent predictor of cardiovascular morbidity and mortality in various adult patient populations with and without cardiovascular disease.1 Increased SNS activity increases blood pressure (BP) and contributes to the development and maintenance of hypertension.2 Multiple studies have demonstrated a correlation between increased SNS activity and higher BP elevation in patients with essential hypertension; this association is not present in secondary hypertension.3 Furthermore, elevated HR is present in a significant proportion of adult borderline hypertensives, beginning in childhood.4 These observations suggest that sympathetic activation is a specific feature of essential hypertension and that heightened SNS activity may play a pathogenetic role in hypertension pathophysiology and prognosis.5
It has been hypothesised that increased SNS activity may contribute to the pathogenesis of elevated BP via direct vasoconstrictive effects on blood vessels, via stimulation of release of adipokines and/or via SNS-mediated insulin resistance.6 Up to 70% of newly diagnosed hypertensive cases are attributable to obesity7; increased kidney and muscle sympathetic nerve activity (SNA) are found in obesity.8 Muscle SNA levels decline with weight loss and increase with weight gain.9 Compared with subcutaneous or lower body fat, visceral abdominal fat, which is the primary source of C reactive protein (CRP) and other proinflammatory adipokines, is more closely associated with increased resting HR and higher SNA in humans.10
Elevated HR has deleterious cardiovascular consequences in addition to elevation of BP. High resting HR may potentially accelerate atherosclerosis via its negative effects on the endothelium.11 There is a close relationship between shear stress and HR1; accelerated HR may promote endothelial shear stress.
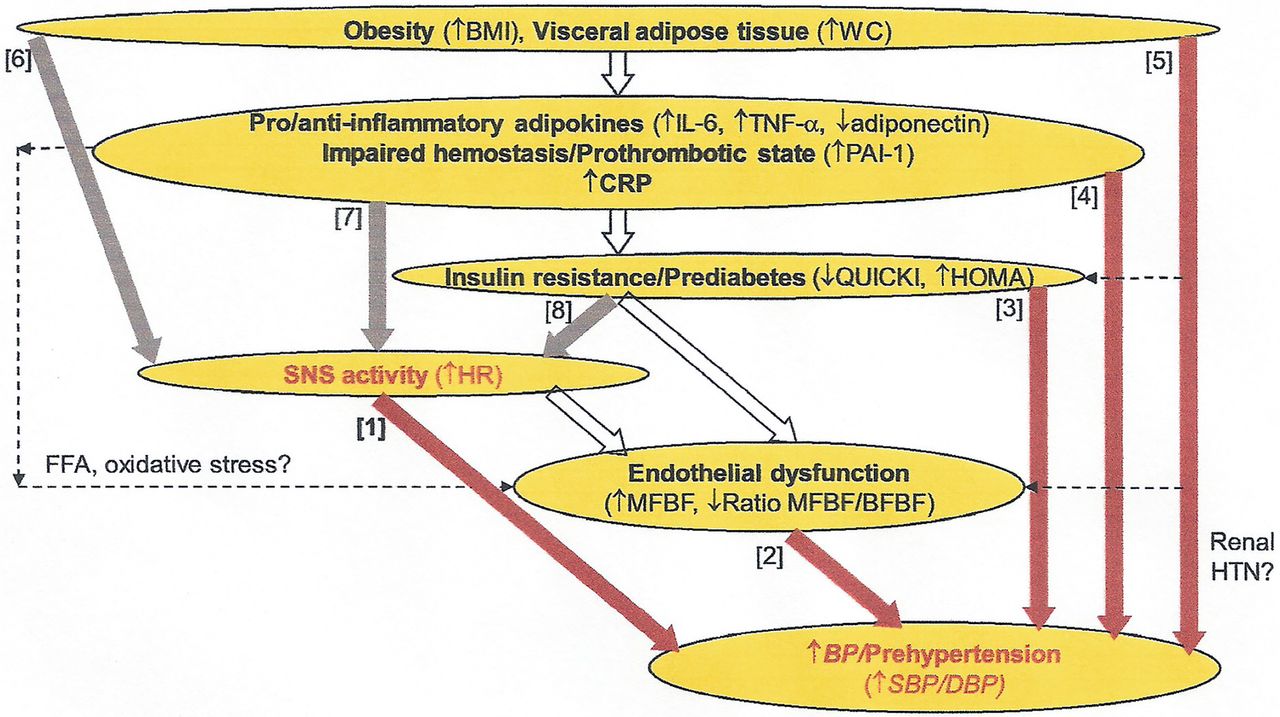
To further investigate the potential role of HR in the early pathophysiology of atherosclerosis, we analysed data from a cohort of non-hypertensive young adults. The primary study objective was to evaluate the direct link between ambulatory 24 h HR and ambulatory 24 h BP (figure 1, pathway [1]), accounting for other potential risk factors that may also independently impact BP, including endothelial dysfunction, insulin resistance, inflammatory markers and measures of adiposity (figure 1, pathways [2]–[5]). The secondary study objective was to assess potential determinants of HR (figure 1, pathways [6]–[8]).

{kind=link}
Diagram of potential causal pathways linking atherosclerotic risk factors. BFBF, baseline forearm blood flow; BMI, body mass index; DBP, diastolic blood pressure; FFA, free fatty acids; HOMA, homoeostatic model assessment; HR, heart rate; HTN, hypertension; IL-6, interleukin-6; MFBF, maximum forearm blood flow; PAI-1, plasminogen activator inhibitor-1; SBP, systolic blood pressure; SNS, sympathetic nervous system; TNF, tomour necrosis factor; QUICKI, quantitative insulin sensitivity check index; WC, waist circumference.
Research methods and procedures
Participants/study design
Data were collected using an observational cross-sectional study design from a cohort of volunteers enrolled in an ongoing investigation of the role of adipokines and insulin resistance in the pathogenesis of hypertension. Participants were recruited from a large urban academic Family Medicine outpatient practice, serving 40 000 individuals in Philadelphia, Pennsylvania, USA. Inclusion criteria were age between 18 and 45 years and absence of hypertension: office systolic BP (SBP) <140 mm Hg and diastolic BP (DBP) <90 mm Hg. Exclusion criteria were diabetes, pregnancy, hypertension, coronary or cerebrovascular disease, collagen vascular disease, organ failure (heart, kidney, liver), and statin medication use. The study was approved by the Thomas Jefferson University Institutional Review Board, and written informed consent was obtained from all participants.
Measurements and data collection
Information was collected on sociodemographic characteristics and current health behaviours. Height and weight were measured and body mass index (BMI) was calculated as weight divided by height squared (kg/m2).
BP and HR
Resting SBP and DBP and HR were measured at the office with a Dinamap cuff. In addition, the participants were also provided with an oscillometric device (Spacelabs 90217A, Spacelabs) for 24 h ambulatory BP monitoring (ABPM), with readings set at 20 min intervals while awake, and 60 min intervals while asleep. Mean 24 h SBP, DBP and HR were calculated, as well as the means of these measures during the awake and asleep periods. SBP, DBP and HR variability were also computed, as the within-participant SD of the ambulatory measurements.
Endothelial function
Minimal forearm vascular resistance (MFVR) at maximal vasodilation is considered an integrated measure of vascular resistance in the forearm.12 We assessed forearm vascular resistance and forearm blood flow non-invasively using plethysmography according to the method of Sivertsson.13 First, we measured baseline forearm blood flow (BFBF) at rest and maximum forearm blood flow (MFBF) during postocclusive reactive hyperaemia. We then calculated both baseline forearm vascular resistance (BFVR=baseline mean arterial pressure (MAP) divided by BFBF) and minimum forearm vascular resistance (MFVR=postocclusive MAP divided by MFBF). The main measures used in the analyses were the per cent increase in FBF and the per cent decrease in FVR (computed as (MFBF−BFBF)/BFBF×100 and (BFVR−MFVR)/BFVR×100, respectively). Several groups have assessed the reproducibility of venous occlusion plethysmography. Roberts et al (1986) demonstrated good within-participant reproducibility for unilateral blood flow measurement, used in this study, with a coefficient of variation of ∼10%.
Insulin resistance
Fasting plasma samples were obtained following an overnight fast and analysed using a Glucostat analyser (YSI, Model 27). Insulin was assayed using a solid phase radioimmunoassay, ‘Coat-A-Count’ (Diagnostic Products Corporation). We computed two common indices of insulin sensitivity. The homoeostatic model assessment (HOMA) index was computed as the product of fasting glucose (mM/L) and fasting insulin (uU/mL), divided by 22.5. The quantitative insulin sensitivity check index (QUICKI) was computed as the reciprocal of the sum of the log fasting glucose (mg/dL) and the log fasting insulin (uU/mL). We used QUICKI in the main analyses, as it tends to have a more symmetric (normal) distribution than the HOMA and does not require logarithmic transformation.14
Inflammatory markers
We measured five inflammatory markers: plasminogen activator inhibitor-1 (PAI-1), interleukin 6 (IL-6), tumour necrosis factor α (TNFα), adiponectin and high-sensitive CRP. Assays were performed using commercially available ELISA kits, which have coefficients of variation 4–6%.
Statistical analyses
The main study objective was to assess the association of HR and HR variability with BP (figure 1, pathway [1]), controlling for other risk factors, mainly endothelial function and insulin resistance (figure 1, pathways [2] and [3]). The main analyses were based on multiple linear regression, with mean 24 h BP (SBP or DBP) as the outcomes, mean 24 h HR or HR variability as the main predictor of interest, and controlling for age, gender, race, endothelial function and insulin sensitivity/resistance. Although endothelial dysfunction and insulin resistance may develop as a consequence of hypertension, they are also possible contributors to the pathogenesis of hypertension. Therefore, we controlled for them in order to isolate the independent association between HR and BP. Additional analyses also controlled for inflammatory markers and measures of adiposity (figure 1, pathways [4] and [5]). We also carried out similar analyses with office measurements of BP and HR, instead of the 24 h ambulatory averages.
The secondary study objective was to evaluate the extent to which HR is impacted by other atherosclerotic risk factors, specifically measures of adiposity, inflammation and insulin resistance (figure 1, pathways [6] through [8]). The main analyses were again based on multiple linear regression, with mean 24 h HR as the outcome, and measures of adiposity, inflammatory markers and insulin sensitivity/resistance as the predictors of interest.
Because of their skewed distributions, IL-6, adiponectin, CRP and FVR per cent decrease were log-transformed in all analyses. Statistical analyses were conducted in SAS V.9.4 (SAS Institute; Cary, North Carolina, USA). The study was powered at 80% or higher for detecting outcomes as noted for these analyses. Missing data were not imputed.
Results
The analyses were based on data from 186 participants. Ambulatory BP and HR measurements were based on an average of 42 readings per participant for the awake period and 8 readings per participant for the asleep period (SD=9 and 2, respectively). Table 1 summarises the characteristics of the study participants. No participant was hypertensive, while 44 (24%) were prehypertensive by either their office BP (ie, office SBP 120–139 mm Hg or DBP 80–89 mm Hg) or their 24 h BP (ie, 24 h SBP 130–134 mm Hg or 24 h DBP 80–84 mm Hg). These included 8 (4%) classified as prehypertensive by both office and 24 h BP, 18 (10%) with white coat prehypertension (ie, office but not 24 h) and 18 (10%) with masked prehypertension (ie, 24 h but not office). Finally, 66 participants (35%) were ‘SBP non-dippers’, that is, their ambulatory mean SBP had dropped less than 10% from their awake to their sleep period.
Study participant characteristics (N=186)
Table 2 presents the correlations of mean 24 h BP and the various risk factors, including mean 24 h HR and HR variability. HR was a modest predictor of DBP but not SBP. By contrast, endothelial dysfunction, measured as the FBF per cent increase or the FVR per cent decrease, was significantly associated with SBP but not DBP. Insulin sensitivity (QUICKI) was significantly and inversely related with both SBP and DBP. All these unadjusted results were qualitatively similar when office measurements were substituted for mean 24 h values (not shown), as office and mean 24 h measures were highly correlated (correlation=0.67 for SBP, 0.53 for DBP, 0.74 for HR; all p<0.001).
Correlations (p values) of HR and other atherosclerotic risk factors with SBP and DBP (N=186)
Table 3 presents the main results regarding the association of 24 h HR with 24 h SBP and DBP (figure 1, pathway [2]), controlling for age, gender, race, endothelial function (FBF % increase from baseline to maximum during postocclusive reactive hyperaemia, figure 1, pathway [2]), and insulin sensitivity (QUICKI, figure 1, pathway [3]). An increment of 10 bpm in the 24 h HR (about 1 SD) was associated with higher 24 h SBP and DBP, by and average of 1.3 mm Hg (p=0.042) and 1.7 mm Hg (p=0.001), respectively. FBF per cent increase was significantly associated with SBP but not DBP (p=0.013 and 0.499, respectively), while QUICKI was not associated with either SBP or DBP (p=0.218 and 0.283, respectively).
Multivariable results for HR and other atherosclerotic risk factors as determinants of SBP and DBP (N=186)
In additional analyses that adjusted for inflammatory markers and BMI (figure 1, pathways [4] and [5]), the effect of HR on SBP was somewhat attenuated (mean SBP difference=0.6 mm Hg per 10 bpm in HR, p=0.422), but that on DBP remained unchanged (mean DBP difference=1.7 mm Hg per 10 bpm in HR, p=0.001). Furthermore, PAI-1 was also a significant predictor of both SBP (mean difference=1.4 mm Hg per 25 mg/mL PAI-1, p=0.041) and DBP (mean difference=1.1 mm Hg per 25 mg/mL PAI-1, p=0.015). Findings were very similar when waist circumference (WC) was substituted for BMI (results not shown).
Awake and asleep HR were both associated with 24 h SBP (p=0.040 and 0.068, respectively) and 24 h DBP (p=0.001 and 0.062). Not surprisingly, the awake HR mean was more strongly associated with the awake SBP and DBP, while the asleep HR mean was more strongly associated with the asleep SBP and DBP. Finally, we did not find any significant association between 24 h HR variability and BP (p=0.443 for SBP and 0.561 for DBP).
The main analyses were also repeated using office measurements of HR and BP instead of their 24 h ambulatory averages. The associations were generally similar as those seen with ambulatory measurements, although their strength was attenuated by about one-third to one-half. As a consequence, neither HR nor PAI-1 was significantly associated with BP, although FBF per cent increase was a significant predictor of office SBP (results not shown).
Table 4 presents the results regarding the association of BMI, inflammatory markers and insulin sensitivity/resistance with 24 h HR (figure 1, pathways [6]–[8]). QUICKI showed a very strong inverse association with HR (p=0.013). Higher CRP was significantly associated with higher HR (p=0.007), while similar associations of PAI-1 and IL-6 with HR were marginally significant (p=0.093 and 0.077, respectively). Unexpectedly, we also found a significant inverse association between TNFα and HR (p=0.015). Neither BMI nor WC (results not shown) was significantly associated with HR.
Atherosclerotic risk factors as determinants of HR (N=175)
Discussion
Mean 24 h HR was independently associated with mean 24 h SBP and DBP, CRP, and QUICKI. The findings from this study of young non-hypertensive individuals suggest that 24 h HR is associated with known risk factors for atherosclerosis prior to the development of diabetes or sustained hypertension. The magnitude of these associations was modest but still potentially clinically meaningful, particularly given that these young individuals did not exhibit any clinical manifestations of atherosclerosis or cardiovascular disease. Although this study specifically excluded hypertensive individuals, a sizable proportion of participants (35%) were SBP non-dippers, and masked prehypertensives (8%), possibly indicating the presence of early stage cardiovascular pathology already underway.
In contrast to HR, HR variability was not significantly associated with BP. Previous studies of HR variability demonstrating an association with BP15 and adipokines16 were conducted in older individuals, suggesting that HR may be an earlier, more sensitive marker of autonomic dysfunction than HR variability. Alternatively, HR variability is typically determined from 24 h ECG recordings. However, HR variability has also previously been calculated as the mean of the SD of HR from ABPM reports as in our study.15 We chose this methodology as we do not have 24 h ECG monitoring equipment. ABPM-calculated HR variability was found in the cited reference to be a significant predictor of carotid intima-media thickness in older hypertensive patients. Our lack of statistically significant findings for HR variability in this study could either be because this alternate methodology may be a less sensitive method for detecting HR variability compared with 24 h ECG monitoring, or due to the inclusion of younger, healthier patients in this study in whom HR variability may not be pathologically altered. Study findings may have been additionally limited by the moderate sample size of 186 participants.
Many inter-related factors contribute to raised BP. Among the factors that have been intensively studied are salt intake, obesity and insulin resistance, the renin-angiotensin system, the SNS, genetics, endothelial dysfunction, smoking, alcohol intake, and exercise. We have not included all possible determinants of BP in order to limit the complexity of our analyses in this study; we chose to focus on the variables noted in figure 1: obesity (BMI), insulin resistance, SNS and endothelial dysfunction.
This study presents evidence of an association between elevated SNA, as represented by elevated HR, and atherosclerotic risk factors which have also been implicated in the pathogenesis of elevated BP: endothelial dysfunction, measures of adiposity, insulin resistance and inflammatory cytokines.17 Endothelial dysfunction is central to the initiation and progression of atherosclerosis, since vascular endothelial cells secrete several antiatherogenic substances including the potent vasodilator nitric oxide.18 Overall, research to date suggests that visceral adiposity is a stronger predictor of endothelial activation than overall adiposity. Insulin resistance is associated with systemic coronary artery disease risk factors, including adiposity; increasing evidence suggests that defective insulin signalling in atherosclerotic lesional cells also contributes to disease progression.19
Elevated levels of inflammatory adipokines promote endothelial dysfunction, hypertension and atherosclerosis.17 Both CRP and IL-6 are molecular markers associated with atherosclerosis and its progression, with IL-6 showing more consistent results and stronger independent predictive value than other inflammatory markers.20 Conclusive in vitro and in vivo findings clearly indicate a proatherogenic role of IL-6.21 IL-6 signalling has been shown to contribute to both atherosclerotic plaque development and plaque destabilisation, while elevated PAI-1 levels appear to increase the risk of atherothrombotic events and may also promote the progression of vascular disease.22
We found that measures of adiposity (BMI or WC) were not significantly associated with HR24 (figure 1, pathway [6]), when insulin resistance and inflammatory markers were controlled for. QUICKI (figure 1, pathway [8]), as well as CRP and to some extent PAI-1 (figure 1, pathway [7]) were independently associated with SNS activity. This suggests that the latter factors may be intermediaries in the main causal pathway linking adiposity to SNS activity. However, we also found an unexpected protective effect of TNFα on HR24 (figure 1, pathway [7]). This could be explained by the fact that plasma TNFα values are usually low. Measurement of TNFα receptors, a better marker of TNFα activity, was not part of the study protocol.
Despite the evidence presented in these and other studies, the exact mechanism by which the SNS mediates its deleterious effects on BP remains unknown. Possible additional mechanisms that we did not explore in this study include activation of the renin-angiotensin-aldosterone system, impaired baroreceptor reflexes, sleep apnoea-activated chemoreceptor reflexes and adipose tissue-derived leptin-mediated SNS activation.6 Also, although our analyses took into account various links between many known or suspected risk factors of atherosclerosis, our data were cross-sectional and cannot establish temporal relationships or causal pathways.
Although multiple epidemiological studies have consistently reported that resting HR is an independent predictor of cardiovascular and all-cause mortality in men and women with and without diagnosed cardiovascular disease, the importance of resting HR as a prognostic factor and potential therapeutic target is not yet generally accepted. Resting HR has been previously found to be a predictor of all-cause mortality in older (aged 45–64 years) prehypertensive older patients.23 HR has also been associated with CRP in elderly men and women (aged 55–75 years),24 middle-aged Israeli men (mean age of about 45 years),25 and with both insulin resistance and CRP in young Japanese men (aged 18–26 years).26 For this study, we specifically recruited young non-hypertensive individuals (including normotensives and prehypertensives) as we aimed to study individuals who have not yet progressed to clinical disease. An additional strength of our study is its diverse population, with substantial fractions of both African-Americans and Asians. African-Americans have not been well studied regarding ambulatory monitoring, although hypertension occurs more commonly and is associated with greater morbidity and mortality in African-Americans compared with Caucasians.27
Most previous studies of HR have utilised resting HR. HR recorded over 24 h has previously been reported to have a better reproducibility (correlation 0.73, with a mean change of only 0.7 bpm over a 3-month interval in 839 hypertensive patients) than office HR (Palatini et al, 2000). Twenty-four-hour HR could therefore be a better prognostic indicator than traditional measurement of resting HR.
Three previous studies analysed mean 24 h HR in individuals much older than those in our study, one with patients with a mean age of 52,28 and the other among patients aged 55–75 years.29 The large ABP-International study of 7600 Caucasians and Asians reported independent predictive value for night-time HR, but not daytime or 24 h HR, for cardiovascular, but not all-cause mortality.28 Similar findings were reported in a study of 653 elderly Europeans.29 However, ambulatory HR did not add additional prognostic information over office HR in a third study of nearly 5000 elderly hypertensive Europeans.30 In our analyses, associations were markedly stronger for 24 h measurements than for office (resting) measurements, suggesting that the 24 h measures may be more sensitive than their office (resting) counterparts in young non-hypertensive adults.
Conclusions
In conclusion, HR, an established indicator of SNS activity, was associated with elevated BP, CRP and insulin resistance in non-hypertensive individuals. This finding suggests that HR may be a potential marker of elevated cardiovascular risk in asymptomatic individuals, prior to the development of clinical hypertension or cardiovascular disease. Furthermore, our findings suggest that the link of adiposity with HR may be mediated by inflammatory markers and insulin resistance. Prospective longitudinal studies are needed to further elucidate the causal pathways that link adiposity, inflammation, insulin resistance, endothelial function and HR, and the degree to which HR measured in early life can predict the incidence of atherosclerosis and cardiovascular disease. Clinical strategies incorporating HR in risk stratification may have possible future utility in identifying asymptomatic individuals to target with individualised preventive therapy.
References
Footnotes
Contributors Both CC and CD contributed to the work by meeting all four of the following authorship criteria: substantial contributions to the conception or design of the work; also, the acquisition, analysis or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Funding for this study was provided by NIH grant HL096593.
Competing interests None declared.
Ethics approval Thomas Jefferson University Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Extra data is available by emailing CC at Cynthia.Cheng@jefferson.edu.